
Abstract
Objective:
To demonstrate the efficacy of locking plate osteosynthesis performed by an L-shaped lateral approach in patients with Sanders type III and IV intra-articular calcaneal fractures with posterior facet displacement.
Methods:
Fifty-three patients with Sanders type III or IV unilateral calcaneal fractures treated with locking plates and additional bone grafting were included in the study. Böhler and Gissane angles, and heel height values were measured on the radiological examinations. Clinical results of the patients were evaluated using the American Orthopaedic Foot and Ankle Society and Maryland evaluation criteria. The presence of arthrosis was investigated with Broden’s view. Preoperative and postoperative values were evaluated.
Results:
The mean Gissane angle was 119.32°, the mean Böhler angle was 9.47° and the mean heel height was 40.82 mm on radiographs at initial presentation of the patients. The mean Gissane angle was 114.63°, the mean Böhler angle was 23.33° and the mean heel height was 47.84 mm on the early postoperative radiographs of the patients. In patients, a mean 4.69° recovery was achieved in the Gissane angle, 13.86° in Böhler angle and 7.02 mm in heel height. On the most recent follow-up, Böhler angle was 21.49°, Gissane was 114.88° and the mean heel height was 46.95 mm. The mean American Orthopaedic Foot and Ankle Society score and Maryland score were 86.91 and 86.53, respectively, on the last follow-up.
Conclusion:
Internal fixation and grephonage using low-profile locking plates provides good functional results to patients since it facilitates anatomic restoration of the subtalar joint and correction of calcaneal height, width and varus/valgus heel.
Keywords
Introduction
Calcaneal fractures are the most common of all tarsal fractures and constitute 1%–2% of all fractures.1–3 Of these fractures, 60%–65% are displaced intra-articular fractures. 4 Displaced intra-articular fractures cause high morbidity. In this respect, calcaneal fractures constitute a great socioeconomic burden. 5
Axial loading caused by falls is the most common mechanism of injury in calcaneal fractures. 6 The conservative treatment of calcaneal fractures entails many complications. Among these are pain, restricted movement of the ankle and subtalar joints, widening of the heel or difficulty in walking due to a decrease in heel height, deformity, peroneal stenosis beneath the fibula, peroneal tendonitis or peroneal dislocation.7–9 Surgical treatment aims to provide early rehabilitation by anatomical and stable reduction and to avoid destructive soft tissue problems.
In the literature, there are wide-ranging treatment approaches to calcaneal fractures, with options such as non-intervention, conservative treatment, open reduction, primary subtalar arthrodesis, delayed primary arthrodesis or calcanectomy.9,10 In surgical treatments, the most preferred approach is intervention by extensile lateral incision. In this intervention, performed with an L-shaped incision, in which the peroneal tendons, sural nerve and calcaneofibular ligament are lifted in the form of a flap, the lateral calcaneal wall is raised off, and especially the central part of the calcaneus is decompressed and the reduction of articular surfaces is achieved. A stable reduction can be achieved by filling bone defects with bone grafts.
This study aims to demonstrate, in mid-term clinical and radiological outcomes, the efficacy of locking plate osteosynthesis performed by an L-shaped lateral approach in patients with Sanders type III and IV intra-articular calcaneal fractures with posterior facet displacement.
Methods
This retrospective research study was approved by Institutional Review Board with the number 2014.83728/2A4. Written informed constant to participate was obtained from all patients in the study. From May 2016 to December 2020, patients with Sanders type III or IV unilateral calcaneal fractures treated with locking plates and additional bone grafting were included in the study.
The inclusion criteria were age more than 18 years, fractures involving the posterior facet classified as Sanders type III or IV, closed fractures and 1 year of follow-up data available. The exclusion criteria consisted of coexistent ipsilateral or contralateral lower extremity injury and/or previous calcaneal disease.
Patients who had the suitable criteria were included in the study.
Intra-articular fractures with joint displacement more than 1 mm, displacement of fracture fragments, shortening and calcaneus with more than 10° valgus or 5° varus, and a Böhler angle less than 15° were operated. After lifting the depressed fragments and joint restoration, defect area was filled by a cancellous bone chip allograft (Aloha Hans Biomed, Daejeon, Korea).
Soft tissue condition was carefully observed. 6.70 (range: 2–18) days. The injury–surgery interval was 6.7 days on average (range: 2–18). The patient was positioned in lateral decubitus and preliminary reduction is checked using lateral, Broden, axial and internal oblique views. The posterior facet of the subtalar joint is definitively fixed with two cortical lag screws, taking care to avoid perforation of the joint (Figure 1).

Posterior facet.
Böhler and Gissane angles, and heel height values were measured on the radiological examinations of the patients at the initial presentation (Figure 2). Clinical results of the patients were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) 11 and Maryland 12 evaluation criteria. The presence of arthrosis was investigated with Broden’s view. Post-traumatic subtalar joint arthritis classification was assessed. 13 A 10-year experienced musculoskeletal radiologist evaluated the X-rays. A 10-year experienced senior orthopaedic surgeon evaluated the patients. Intra-observer reliability score was evaluated.

Radiographic parameters.
The change in shoe size of patients, the time to stepping down and the time to return to work were recorded. Preoperative and postoperative values were evaluated statistically.
Surgical technique
All surgical operations were performed on the radiolucent table, in the lateral decubitus position and using a high thigh tourniquet. Only the extended lateral approach was used in all patients. An L-shaped incision was made 4 cm above the lateral malleolus, starting from the middle of the Achilles tendon and posterior border of the fibula and extending to the base of the fifth metatarsal (Figure 3).

L-shaped incision.
A subperiosteal flap was created by preserving the soft tissue and sural nerve with sharp dissection. By retracting the flap superiorly with K wires passed to the talus and cuboid bone and forcing the foot to inversion; the lateral wall of the calcaneus, the posterior facet and the calcaneocuboid joint were clearly revealed. The fragmented lateral wall fragment was removed from the calcaneus in the form of a lid. If the fragment in the lateral wall was not completely separated, it was removed from the cortex with an osteotome. The collapsed posterior facet was clearly revealed. The collapsed piece was placed in its normal place (Figure 4). Then, the posterior facet was fixed temporarily with K wires directed towards the sustentaculum. Reduction of the calcaneocuboid joint was also achieved and temporary fixation was performed. Lateral and axial images were taken with fluoroscopy and the posterior facet, calcaneocuboid joint, sustentaculum reduction and trunk varus/valgus alignment were checked (Figures 5 and 6). Schanz screw was used to provide varus and valgus heel height. After the reduction was achieved, the facet reduction was preserved with a screw directed from the thalamic region of the posterior facet to the sustentacula, then a low-profile titanium- or steel-locked calcaneus plate (True Lock, Truemed) was placed on the lateral calcaneal wall for permanent fixation. Lag screw application can also be performed to fix the main parts. The orientation of the screws used in plaque fixation is one of the most important points for internal fixation. Tight fixation should be ensured by directing the screws into the dense bone tissue under the sustentaculum lateral, posterior articular surface and the attachment of the Achilles tendon. Fixation was achieved with cortical or cancellous locking screws.

Osteotome usage.

Lateral view.

Axial view.
The surgeries were performed by the same senior surgeon.
Statistical analysis
SPSS 20.0 for Windows 7 (IBM, Inc., Armonk, NY, USA) was used for statistical analysis. Categorical variables are reported as numbers and percentages, while numerical variables are reported as means and minimum–maximum ranges. When the numerical variables provided a normal distribution condition, the independent two group comparisons were compared using the Student’s t-test, and when the normal distribution condition was not met, the independent two group comparisons were compared using the Mann–Whitney U test. The ratios in the groups were compared with chi-square analysis. For all tests, the statistical significance was defined as an alpha level of p < 0.05.
In power analysis, the sample size was 56 at 80% power (G_Power Version 3.1.7).
Results
A total of 53 patients out of 142 were included in the study. Eighty-nine patients were excluded. Demographic changes of the patients were shown on Table 1. The mean postoperative follow-up time of the patients was 28.98 months (range: 12–100).
Demographic changes of the patient.

The mean Gissane angle was 119.32° (range: 83°–150°), the mean Böhler angle was 9.47° (range: −18° to 40°), the mean heel height was 40.82 mm (range: 32–51) on radiographs at initial presentation of the patients. The mean Gissane angle was 114.63° (range: 92°–140°), the mean Böhler angle was 23.33° (range: −10° to 44°), the mean heel height was 47.84 mm (range: 35–56) on the early postoperative radiographs of the patients (Table 2). In patients, a mean 4.69° recovery was achieved in the Gissane angle, 13.86° in Böhler angle and 7.02 mm in heel height. On the most recent follow-up, Böhler angle was 21.49° (range: −8° to 44°), Gissane was 114.88° (range: 94°–134°). The mean heel height was 46.95 mm (range: 34–56). In the postoperative follow-up, it was found that three patients had overcorrection compared to the foot on the opposite side. The restoration of the anatomy was compared to contralateral side. There was no statistical difference between the early postoperative Gissane and Böhler angle and the last follow-up Gissane angle in patients (p = 0.577). There was no statistical difference between the early postoperative and the most recent follow-up heel heights (p = 0.634).
Radiological measurements.

Wound necrosis and dehiscence were observed in one patient after the first month. In five (8.8%) patients, superficial wound dehiscence developed in 2 to 5 days after surgery. Implants applied for fixation were removed in two patients after surgery. Sudeck’s atrophy developed in two patients in the postoperative sixth month.
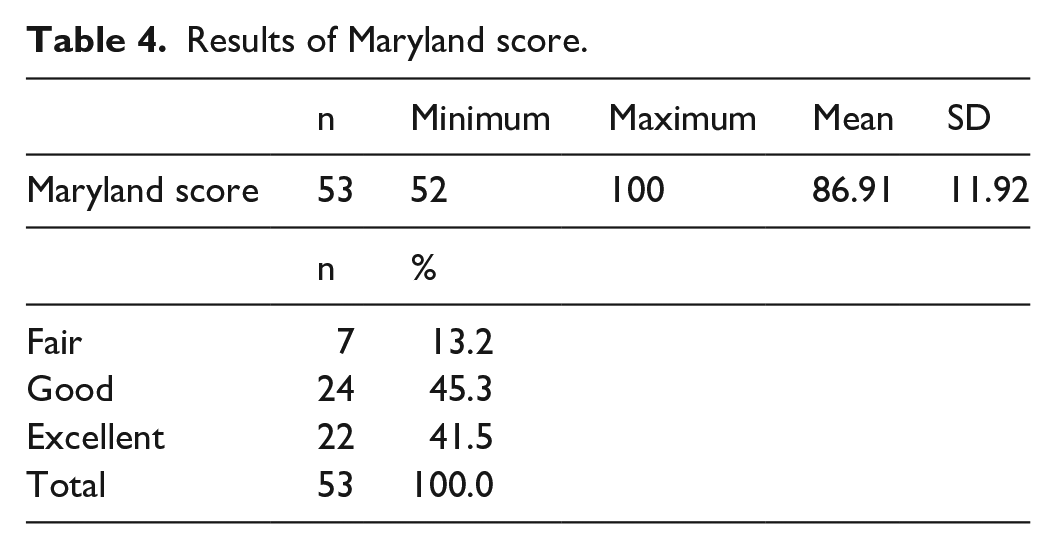
The mean AOFAS score (Table 3) and Maryland score (Table 4) was 86.91 (range: 52–100) and 86.53 (range: 52–100), respectively, on the last follow-up of the patients.
Results of AOFAS score.

AOFAS: American Orthopaedic Foot and Ankle Society.
Results of Maryland score.
On the most recent outpatient follow-up of the patients, the mean shoe size did not change in 32 (56.1%) patients, increased by 1 in 21 (36.8%) patients and by 2 in 4 (7%) patients. Subtalar arthrosis was not detected in 30 (52.6%) feet. Type I arthrosis was detected in 20 (35.1%) feet. Type II arthrosis was detected in 7 (12.3%) feet. There was no statistically significant difference between subtalar arthrosis and fracture types (p = 0.65; Figure 7).

Results graph.
Discussion
In the conservative treatment of calcaneal fractures which is preferred due to the technical difficulty and high complication rates of surgical treatment, an anatomical and stable reduction is rarely achieved. In addition, calcaneal deformities such as shortening, loss of height and widening that may occur with conservative treatment, as well as subtalar joint and peroneal tendon problems, and problems such as pain and functional impairment are commonly encountered. With osteosynthesis and grephonage performed by the lateral approach, complication rates are reduced and significant improvement is achieved in functional outcomes.
Depending on the impaction, separation and rotation of the fracture parts formed in intra-articular fractures, loss of height in the calcaneus, expansion of the heel and extensive damage to the joint surfaces may occur. 14 Any decrease observed in the Böhler angle is a sign of a collapse of the posterior joint surface. This angle may be decreased in both intra-articular and extra-articular fractures. Böhler angle less than 0° on the patient’s presentation to the hospital increases the probability of subtalar arthrodesis by 10 times. 15 In a previous study, it was stated that the results are better in non-displaced calcaneal fractures and poorer in non-operated displaced fractures with the restoration of Böhler angle < 10°. 16 The locking plate and bone graft support we used for the restoration of the Böhler angle and the stabilization of reduction was important for our good results.
Seventy-five percent of calcaneal fractures are intra-articular fractures in which the posterior talar joint surface is affected. 14 The main purpose of surgical treatment can be summarized as the configuration of the subtalar joint, especially the posterior joint surface, and the restoration of the height and width of the calcaneus. 17 Numerous publications are showing that conservative treatment fails in displaced intra-articular fractures.18,19 Surgery is an effective treatment especially in male patients with multiple trauma who are engaged in hard physical work. In this regard, Schepers T. et al. 20 have proved that surgical treatment is superior in intra-articular calcaneal fractures.
Previously, the most important criterion for successful treatment of calcaneal fractures was considered to be the correction of the calcaneal shape, especially the Böhler angle. 21 For this reason, the medial approach was preferred to provide better correction of the extra-articular surface of the calcaneus. On the contrary, today the restoration of the posterior articular surface is known to be the most important factor that yields successful results and a lateral incision is preferred, which allows better control on the joint. 22 Higher rates of complication with medial intervention and insufficient reductions of the subtalar joint with indirect reduction have been reported. 23 In our study, the lateral incision was preferred and sufficient improvements of the Böhler angle were achieved, requiring no additional medial incision. The efficacy of lateral incision was demonstrated as well as its sufficiency for anatomical reduction. We raised the fasciocutaneous flap containing the sural nerve and peroneal tendon to preserve these structures. We have been diligent at several points to prevent wound healing complications. Patient selection and surgical timing are critical. We waited until the oedema resolved. The application of the ‘no-touch’ technique without damaging subcutaneous tissues and the lifting up of the lateral cortex respecting the vascular pedicle were effective in our low rates of complication.
Although controversial, filling the defective gap in the calcaneus with auto- or allograft is important for ensuring secondary stability. 20 Restoring the heel width prevents chronic peroneal tendinitis caused by the rupture of the lateral calcaneal wall while restoring the calcaneal height ensures the preservation of the length of the Achilles tendon and the plantar flexion force. 7 After the graft is placed, stability is achieved by using a low-profile calcaneal plate. In our cases, it was observed that filling the defective area with graft during surgery contributes to secondary stability and helps preserve reduction. One of the main implications of our study is the demonstration of the efficacy of allograft by using the locked plate in maintaining the joint level and calcaneal height corrected during surgery.
Since most of the patients with calcaneal fractures are middle-aged working men, the morbidity and loss of labour force caused by the fracture are massive. 20 A study reported that an economic analysis of displaced intra-articular calcaneal fractures showed that the rate of delayed subtalar arthrodesis was lower, the quality of life was higher and the treatment was less costly in the group who underwent surgery as primary treatment. 4 Several studies have reported that the surgically treated patient group with calcaneal fracture had 1.5 times less pain than the non-surgically treated group. They have also reported that the rate of delayed subtalar arthrodesis in the non-surgical treatment group was 5.5 times higher. 20 None of our cases underwent arthrodesis. All of our patients returned to their jobs in the 13th month at the latest. Favourable results were obtained in terms of pain and stability.
Although non-surgical treatment reduces the risk of complications related to surgery, it also causes symptomatic malunion due to the calcaneal height and configuration not being restored. Typical findings of calcaneal malunion are subtalar arthritis due to posterior facet and calcaneocuboid joint incompatibility, heel widening and sub-fibular impingement of the peroneal tendons due to expansion of the lateral calcaneal wall, reduction of ankle dorsiflexion due to decrease in calcaneal height and hindfoot malalignment and varus deformity due to displaced calcaneal tuberosity.9,24 This study supports the surgical treatment of displaced calcaneal fractures with open reduction and internal fixation.
In the literature, it has been reported that even a 1 mm pathological cascade of the joint disrupts the load distribution on the subtalar joint and causes gait abnormality. 5
The anatomical reduction is claimed to be necessary for favourable clinical outcomes but does not guarantee it due to possible cartilage damage.6,16 There are numerous publications advocating treatment with a closed reduction in type IV fractures.25,26 However, there are also many studies indicating the superiority of surgical treatment over closed treatment. Considering the literature advocating surgery in type IV fractures, surgery arguably shortens the time to return to work, significantly prolongs the progress to subtalar fusion and is cost-effective. 4
In the literature, the most common complications after surgical treatment are flap necrosis and deep or superficial infection with a reported rate of 5%–15%.18,21 Arthritis and pain accompanying wound healing are the most common complications. These are almost inevitable for any type of fracture, but it is possible to reduce their incidence by carefully selecting patients, monitoring postoperative treatment and recruiting experienced surgeons.
Among the limitations of our study are the low number of patients, the retrospective design, the high healing potential of the calcaneus and its cancellous bone structure influencing favourable outcomes.
Conclusion
In Sander type III and IV calcaneal fractures, the method of internal fixation and grephonage using low-profile locking plates provides good functional results to patients since it facilitates anatomic restoration of the subtalar joint and correction of calcaneal height, width and varus/valgus heel.
Footnotes
Author contributions
A.V. was involved in the study design, data collection and analysis; Y.O. was involved in data collection and analysis; B.E.K. contributes towards article writing and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Hamidiye Institutional Review Board (2014.83728/2A4).
Informed consent
Written informed consent was obtained from all subjects before the study.