
Abstract
It is uncommon to observe a nonunion of an isolated ulnar shaft fracture after surgical treatment; therefore, complications due to this nonunion are very rare. Adults are more likely to develop nonunions compared to children. We report the case of a 34-year-old man, who had a left ulnar shaft fracture, treated with a screwed plate. Four months later, a septic nonunion occurred causing a type 3 Monteggia equivalent lesion with a lateral dislocation of the radial head. We describe the consecutive methods of treatment that resulted in complete bone consolidation. The case report aims to underline the diagnostic particularities and the therapeutic challenges of this rare complication.
Introduction
Isolated ulnar shaft fractures had a reputation of nonunion when a non-operative treatment was used. The ulna is the stationary bone of the forearm that was most likely to fail to heal following a fracture. 1 Thanks to the evolution of treatment options, ulnar nonunions became uncommon. The potential risk factors are open fractures, associated infections, inadequate stability, and insufficient metabolic response. 2 Monteggia fractures include a proximal third fracture of the ulnar shaft associated with a radiocapitellar joint dislocation. 3 Therefore, an ulnar shaft nonunion followed by a radiocapitellar joint dislocation is a very rare complication of an initially isolated ulna fracture. Our case report aims to underline the diagnostic particularities and the therapeutic challenges of such a series of events.
Case report
A 34-year-old, right-handed man was admitted to the emergency department following a closed trauma of his left upper extremity; he fell on his forearm with a flexed elbow. Clinical examination found deformity and swelling of the forearm without open wounds or neuro-vascular abnormalities, with palpable pulses and maintained range of motion at the hand and the wrist. Radiographs revealed an isolated fracture of the proximal third of the ulnar shaft (Figure 1). Three days after the injury, the patient underwent an open reduction internal fixation of the left ulna. Anatomic reduction of the ulna fracture was obtained, and fixation was achieved with a small-fragment dynamic compression plate (Figure 2). After the healing of the surgical wound, we referred the patient for physical therapy.
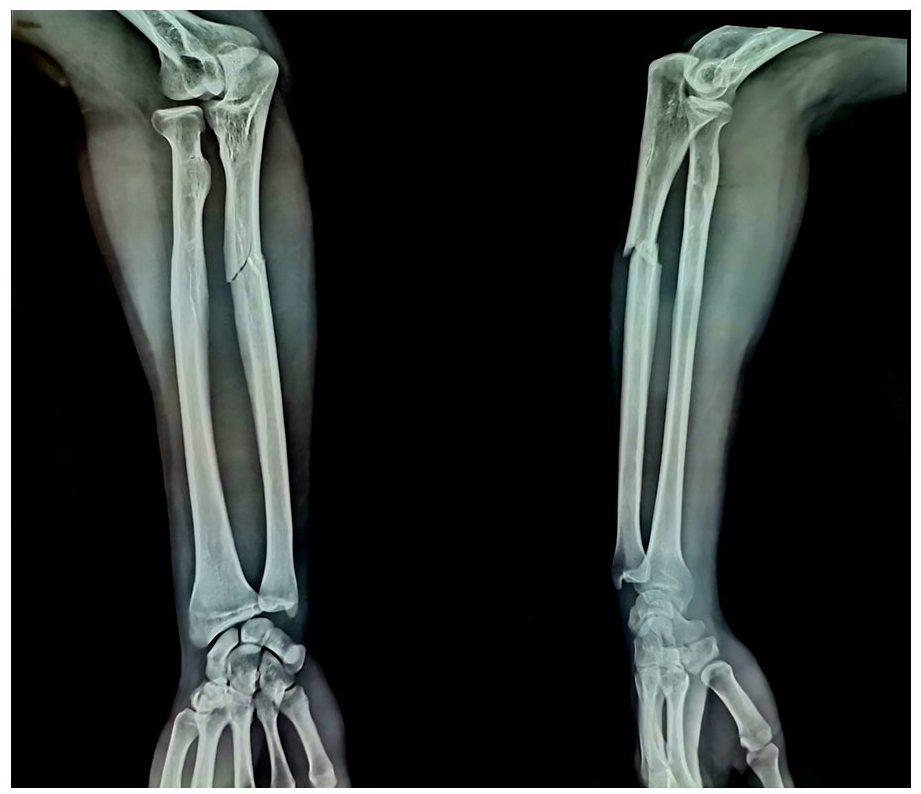
Anteroposterior and lateral radiographs of the left forearm show a fracture of the proximal third of the ulnar shaft.
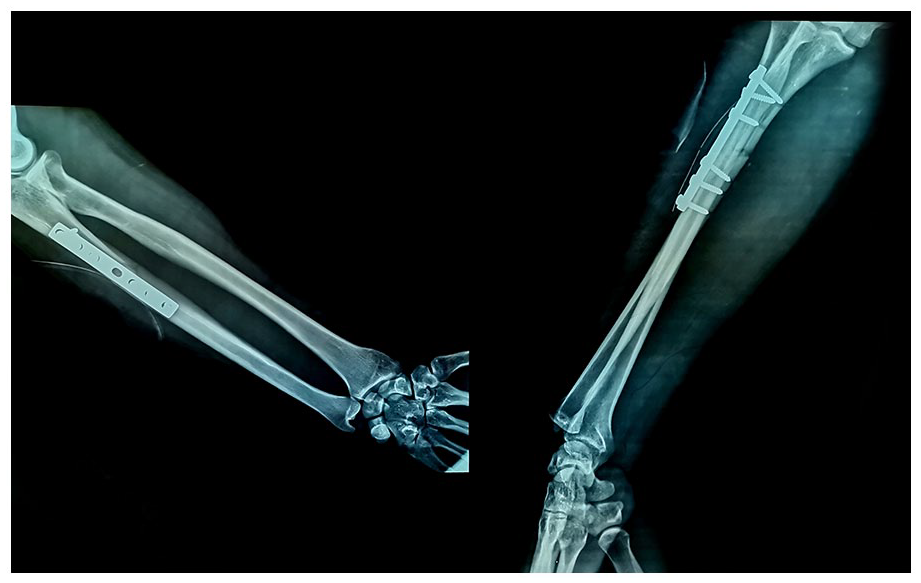
Postoperative left forearm radiographs show the reduction and the fixation of the ulnar shaft fracture.
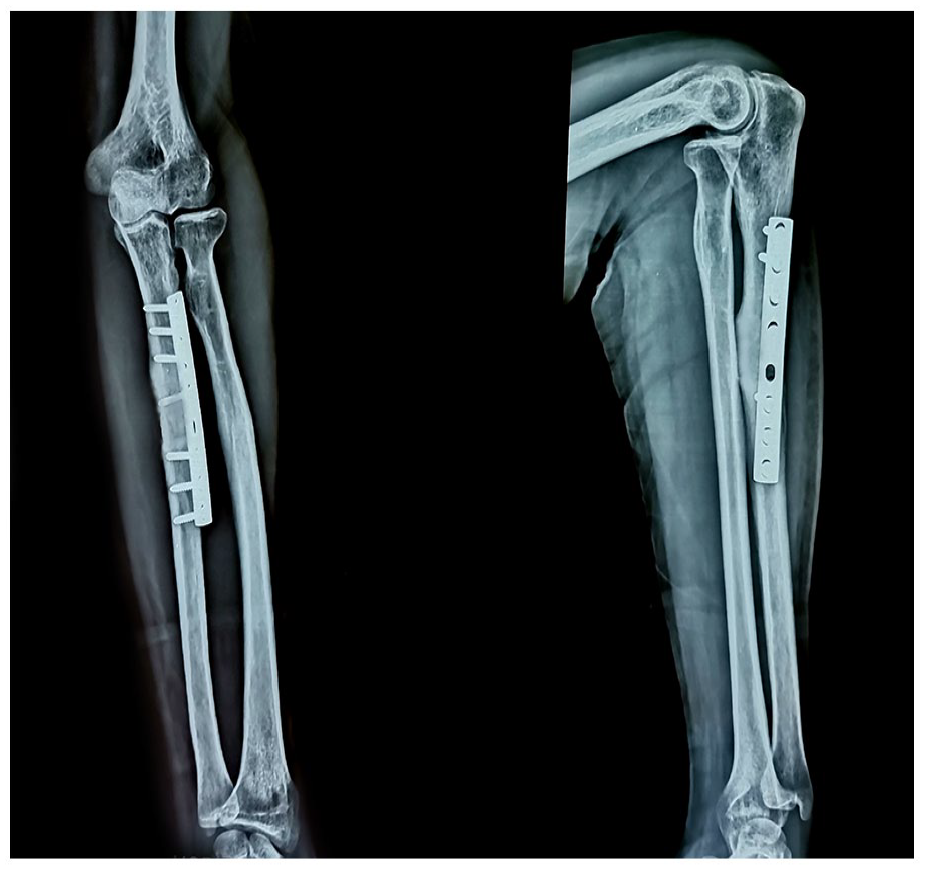
In the third control, 2 months postoperatively, the patient had swelling and tenderness of the surgical scar with a local rise in temperature. Radiographs revealed a focal opacity and an absence of osseous consolidation. The patient underwent surgical debridement and evacuation of pus under general anesthesia, without plate removal. Samples were sent for culture sensitivity. Methicillin-resistant Staphylococcus aureus was isolated and cultured. Antibiotics (oral clindamycin and ciprofloxacin) were given and the limb was immobilized in an above-elbow cast for 6 weeks. At 4 months after injury, the diagnosis of septic nonunion was made based on the absence of consolidation on the X-rays and the persistent signs of local infection. The patient had a plate removal (Figure 3) with extensive debridement and irrigation. More antibiotics were given (oral ciprofloxacin) for another 6 weeks due to the presence of methicillin-resistant Staphylococcus aureus in the first culture.

Anteroposterior and lateral radiographs of the left elbow show the nonunion site after plate removal.
At 8 weeks after plate removal, white blood cell count and erythrocyte sedimentation rate (ESR) were 6100/mm3 and 8 mm/h, respectively, with no other signs of infection. The limb was immobilized with an above-elbow cast. At that time, the radiographs revealed a lateral dislocation of the radial head, resembling a type 3 Monteggia fracture (Figure 4). The patient had another surgery where the ulnar diaphysis nonunion was radically resected along with fibrous tissue and samples were sent for culture sensitivity. The bone marrow canal was opened with a drill on both ends of the nonunion. After the reduction of the fracture, an autogenous corticocancellous bone graft from the left iliac crest was retrieved and inserted into the nonunion site. A screwed dynamic compression plate (with a screw fixed in the graft) allowed us to obtain full stability and reduction of the ulnar shaft leading to the reduction of the radial head. The cultures were negative.

Anteroposterior and lateral radiographs of the left elbow and forearm show a lateral dislocation of the radial head with an ulnar shaft nonunion, resembling a type three Monteggia fracture.
After this fourth surgery, physical therapy started in the third week and the patient had a control every 4 weeks. Six months postoperatively, the patient did not complain of pain. Physical examination revealed full flexion and extension of the left elbow as well as pronation and supination movements in the left forearm (Figure 5). Radiographs showed full osseous consolidation (Figure 6).

Flexion (a), extension (b), pronation (c), and supination (d) range of motion at 6 months of follow-up.
Anteroposterior and lateral radiographs of the left forearm show an osseous consolidation of the ulnar shaft with a reduced radiocapitellar joint at 6 months of follow-up. The reduction seems more obvious from the anteroposterior view.
Discussion
Nonunion is an uncommon complication of isolated ulnar shaft fractures. A potential risk factor such as an infection should be investigated to provide the correct solution for bone consolidation. 4 The best method of treatment of ulnar shaft fractures is still controversial. Although some authors recommend above elbow plaster 5 while others prefer a short cast. 6 Internal fixation is still preferred as the treatment of choice by some. 7 In cases involving infection, the formation of necrotic and lytic bone with pus inhibits union. 8 The fundamentals of any septic nonunion treatment are debridement, antibiotics, alignment, stability, soft tissue coverage, and bone grafting. The bone defect left after debridement needs to be reconstructed once the infection has been eliminated. 9 Defects of up to 6 cm can be strongly grafted with a cancellous or tricortical autograft. The advantages of a tricortical graft are as follows: intrinsic stability, the option to use compression plating (instead of bridging plating), fixation of the graft itself with a screw, and rapid incorporation without the need for timely remodeling after cancellous grafting. 10
All Monteggia fractures in the adult population should be treated surgically; open reduction with internal fixation should be the method of choice. 11 The anatomic reduction of the ulna is critical for the reduction of the radiocapitellar joint. The proximal ulna has a dorsal angulation of about 6° that we should restore when obtaining reduction and fixation. Application of a straight plate can cause malalignment of the proximal ulna (thus persistent dislocation of the radial head). 12 The most common complications that can happen after fixation of Monteggia fractures are as follows: dislocations are hardware irritation/prominence, radial and ulnar neuritis, elbow stiffness, heterotopic ossification, persistent radial head subluxation, and radioulnar synostosis. 13
Conclusion
A septic nonunion after an isolated ulnar shaft fracture is rare. The instability and displacement of the ulna can lead to a radial head dislocation resulting in a Monteggia equivalent fracture. Anatomic reduction of the ulnar diaphysis is usually sufficient for the reduction of the radiocapitellar joint. The reported association of lesions is very rare and can be challenging. The treatment plan requires a multidisciplinary process involving a radiologist, a physical therapist, an infectious disease specialist, and an orthopedic surgeon.
Footnotes
Acknowledgements
The authors have no acknowledgment.
Authors’ contribution
The authors confirm their contribution to the paper as follows: study conception and design: N. N. and K. B.; data collection: W. C. and H. K.; draft manuscript preparation: A. M. and A. H. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.