
Abstract
Objective:
Reproductive rights violations are a serious public health concern worldwide, particularly in Sub-Saharan Africa, where more than 38.83% of victims live. Understanding the status of husbands’ knowledge and involvement helps to establish important programs and interventions. However, there are limited data related to husbands’ roles in women’s reproductive rights in the study setting. Therefore, this study aimed to assess husbands’ knowledge and involvement in women’s reproductive rights and their associated factors in Harar, eastern Ethiopia.
Methods:
A community-based cross-sectional study was conducted among 611 husbands in March 2020. A systematic random sampling technique was used to select the study participants. Data were collected using a structured and pretested interviewer-administered questionnaire. Data were entered using EpiData 3.1 and analyzed with SPSS Version 22. A multivariable logistic regression model was applied to examine the factors associated with the outcome variable using an adjusted odds ratio with a 95% confidence interval, and a p-value < 0.05 was considered statistically significant.
Results:
The levels of husbands’ knowledge and involvement were 48.3% and 40.1%, respectively. Social media utilization (adjusted odds ratio = 4.97, 95% confidence interval = 2.79–8.85), partners’ discussion (adjusted odds ratio = 2.33, 95% confidence interval = 1.60–3.39), and type of facility: hospital (adjusted odds ratio = 3.21, 95% confidence interval = 1.23–8.36) and health post (adjusted odds ratio = 2.86, 95% confidence interval = 1.20–6.94) were factors associated with knowledge of husbands. Likewise, the experience of using reproductive services (adjusted odds ratio = 2.15, 95% confidence interval = 1.52–3.03), partner discussion (adjusted odds ratio = 1.95, 95% confidence interval = 1.35–2.82), social media utilization (adjusted odds ratio = 1.74, 95% confidence interval = 1.05–2.89), and age 40–49 years (adjusted odds ratio = 1.99, 95% confidence interval = 1.19–3.32) were factors associated with husbands’ involvement.
Conclusion:
Less than half of the husbands were knowledgeable and involved in executing partners’ reproductive rights. Promoting and creating effective media utilization is important for creating awareness of reproductive rights. Moreover, working on reproductive health service utilization, women empowerment, and making open discussions between partners are crucial to increase the knowledge and involvement of husbands.
Introduction
A reproductive right is the right of an individual to decide and choose about reproduction free of discrimination, coercion, and violence.1–3 The roles and responsibilities of men in the reproductive rights of women marked an important milestone internationally during the mid-1990s.4,5 These rights include freedom from coercion, discrimination, and violence; the equal relationship between women and men in matters of sexual relations and reproduction; mutual respect; and shared responsibilities for sexual behavior.1,2,6 Before this time, relevant policies, programs, and strategies were exclusively focused on women and promoted their roles in improving reproductive rights. The first global initiative that urged to extend the focus beyond women and emphasized that the shared responsibility of men was the Cairo International Conference on Population and Development (ICPD). 1 Subsequently, the World Health Organization (WHO) and other international organizations began to target men in programs related to reproductive health.1–3
Inadequate knowledge and lack of male involvement and support for sexual and reproductive health rights and services are seen by many women as a cause of intimate partner violence (IPV) and a barrier to accessing services in low-income countries.1,7,8 Globally, one out of three women experiences IPV. 9 These violations are a serious public health concern worldwide. However, the problem is more common in low- and middle-income countries (LMICs) especially in Sub-Saharan Africa, where 38.83% of the women are abused by their intimate partners.3,10–15 Women’s reproductive rights need attention because they pose a serious challenge to the health of women and their families.1,3,16
Lack of partners’ knowledge of reproductive rights is among the primary factors related to IPV.7,8 The burden of IPV during pregnancy is multidimensional. Violence is related to physical, sexual, psychological, emotional, and access to reproductive health, such as family planning. 16 For example, inadequate utilization of healthcare services, unintended pregnancies, inadequate prenatal care, pregnancy-related distress (antepartum, intrapartum, and postpartum depression), induced abortion, and sexually transmitted infections that are responsible for the burden of maternal morbidity and mortality.16–23
Available evidence in LMICs indicates that inadequate knowledge and involvement of husbands in the reproductive rights of women, lack of reproductive education, and spousal discussions are the common causes of violations in the reproductive rights of women.22,24–29 Likewise, the major contributing factors related to male partners’ involvement in partners’ reproductive rights are accessibility and utilization experience of reproductive health services, lack of spousal discussions on reproductive health and transportation access, and time to reach a health institution.30–32
To achieve the Sustainable Development Goals (SDGs), the United Nations agenda is related to gender equality and empowering all women, which is very important to ensure universal access to sexual and reproductive rights for women seated for 2030. 1 Likewise, the Ethiopian minister of health set seven strategic directions to protect women’s reproductive and human rights.9,33 Appropriate and effective promotion of the participation and support of men in the protection of women’s reproductive rights requires an understanding of the current status of husbands’ knowledge and involvement helps to set important programs and interventions on maternal healthcare needs in general and respecting women’s reproductive rights in particular. Examining male partners’ knowledge and involvement in women’s reproductive rights has important implications for improving maternal health service utilization and reducing maternal morbidity and mortality. It also has great implications for planning an effective intervention strategy to improve their knowledge and involvement in maternal health service utilization. There are limited data related to husbands’ knowledge and involvement and its associated factors on women’s reproductive rights in eastern Ethiopia. Therefore, this study aimed to assess husbands’ knowledge and involvement in women’s reproductive rights and their associated factors in Harar, eastern Ethiopia.
Methods and materials
Study setting and design
A community-based, cross-sectional study was conducted in March 2020. The study was conducted in Harari Regional State, eastern Ethiopia which is located 526 km from Addis Ababa, the capital city of Ethiopia. The region had an estimated 226,000 population with 125,000 urban, and the remaining were rural populations. 34 This region is structured with nine woredas (districts), six urban and three rural, and comprises nineteen city kebeles (smallest administration unit) and seventeen rural kebeles. We included all married male partners who lived in Harar city. However, male partners who were severely ill and temporarily not available in the city during the study period were excluded.
Sample size and sampling procedure
The sample size was determined using a single population proportion formula considering the following assumptions: 5% level of significance (α = 0.05), 95% confidence interval (CI), a design effect of 1.5, and a proportion of 50% (to obtain the maximum sample). Therefore, the final sample size for this study was 633 with 10% non-response rate

We used a multi-stage sampling technique to select four districts using simple random sampling. From the selected district, we selected two kebeles from each district using a simple random sampling technique. After that, we distributed the sample to the selected eight kebeles based on the proportionately allocated sample size. Finally, we employed the required study subjects using a systematic random sampling technique. A sampling interval (k) was 5 for each kebele to select male partners, where the first eligible man was selected using the lottery method.
Data collection methods
Data were collected using a pretested structured questionnaire adapted and modified from different studies in the local context.7,35 The questionnaire was translated from English into local languages (Afaan Oromo and Amharic). It was then translated back into English to maintain consistency. The questionnaire contained three parts: socio-demographic characteristics, husband’s knowledge, and involvement related to sexual and reproductive rights and reproductive health-related questions. Data were collected through face-to-face interviews with eight trained diploma nurses and midwives, and two supervisors checked and monitored the data collection process daily.
Knowledge of husbands was measured using 11 standard reproductive right questions, each scored 1 and 0 (1 = correct and 0 = incorrect). Those who scored above the mean scored value of knowledge measuring questions were considered knowledgeable. Likewise, husbands’ involvement was defined as partners’ current support or help to their partner in the use or exercise of her reproductive rights. We used seven questions to assess husbands’ level of involvement in partners’ reproductive rights and each scored 1 and 0 (1 = correct and 0 = incorrect). Those partners who scored at or above the mean value of involvement measuring questions were categorized as having good involvement in their partners’ reproductive rights. 35
Data quality control
Two days of training were provided to all data collectors and supervisors. We conducted a pretest on 5% (32 participants) of the sample size out of the selected district (Hakim district not included in the final sample) before the actual data collection. Based on the findings of the pretest, we made minor modifications to the questionnaire. The data collection process was closely supervised, and the completeness of each questionnaire was checked by the investigators and supervisors daily. During data cleaning, a logical checking technique was used to identify the errors. Finally, double data entry was performed to verify the consistency of the data.
Data processing and analysis
The data were coded and entered into EpiData Version 3.1 and exported to the Statistical Package for Social Sciences (SPSS) Version 22 statistical software for analysis. A univariate analysis was used to describe the frequency distribution variables. We coded the outcome variables as “1” for knowledgeable and good involvement, whereas “0” for not knowledgeable and poor involvement of husbands. The association between the outcome and independent variables was analyzed using a logistic regression model. Covariates with a p-value ⩽ 0.25 were retained and entered into the multivariable logistic regression analysis using a forward stepwise approach. A multicollinearity test was performed to determine the linear correlation among the independent variables using the variance inflation factor (>10) and standard error (>2). The goodness-of-fit test was performed using the Hosmer–Lemeshow test (>0.05). Adjusted odds ratio (AOR) with 95% CI using a p-value < 0.05 was considered a statistically significant association with the outcome variable.
Results
Socio-demographic characteristics
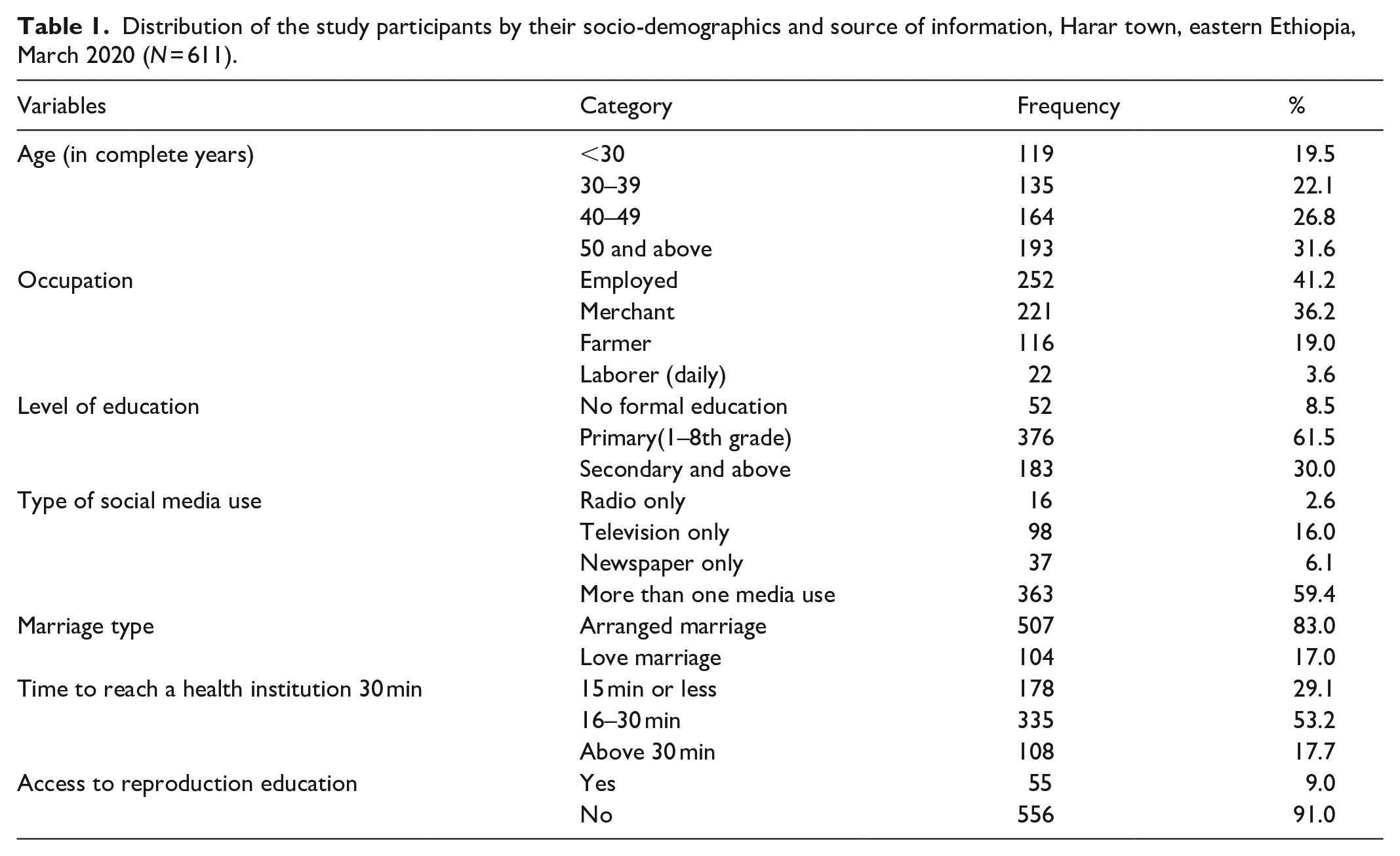
A total of 611 study participants were included in the study, yielding a response rate of 96.5%. The age of respondents ranged from 20 to 79 years (mean ± standard deviation (SD) = 44 ± 13.79). Two hundred fifty-two (41.2%) participants were employed. One hundred eighty-three (30.0%) husbands had a secondary and higher level of education. More than four-fifths (84.1%) of the respondents used social media, of which nearly three-fourths (75.3%) used more than one social media weekly. A total of 513 (82.3%) respondents lived near the health facilities (less than 30 min). The majority 556 (91%) reported that they had no access to reproductive health education (Table 1).
Distribution of the study participants by their socio-demographics and source of information, Harar town, eastern Ethiopia, March 2020 (N = 611).
Knowledge of husbands about partners’ reproductive rights
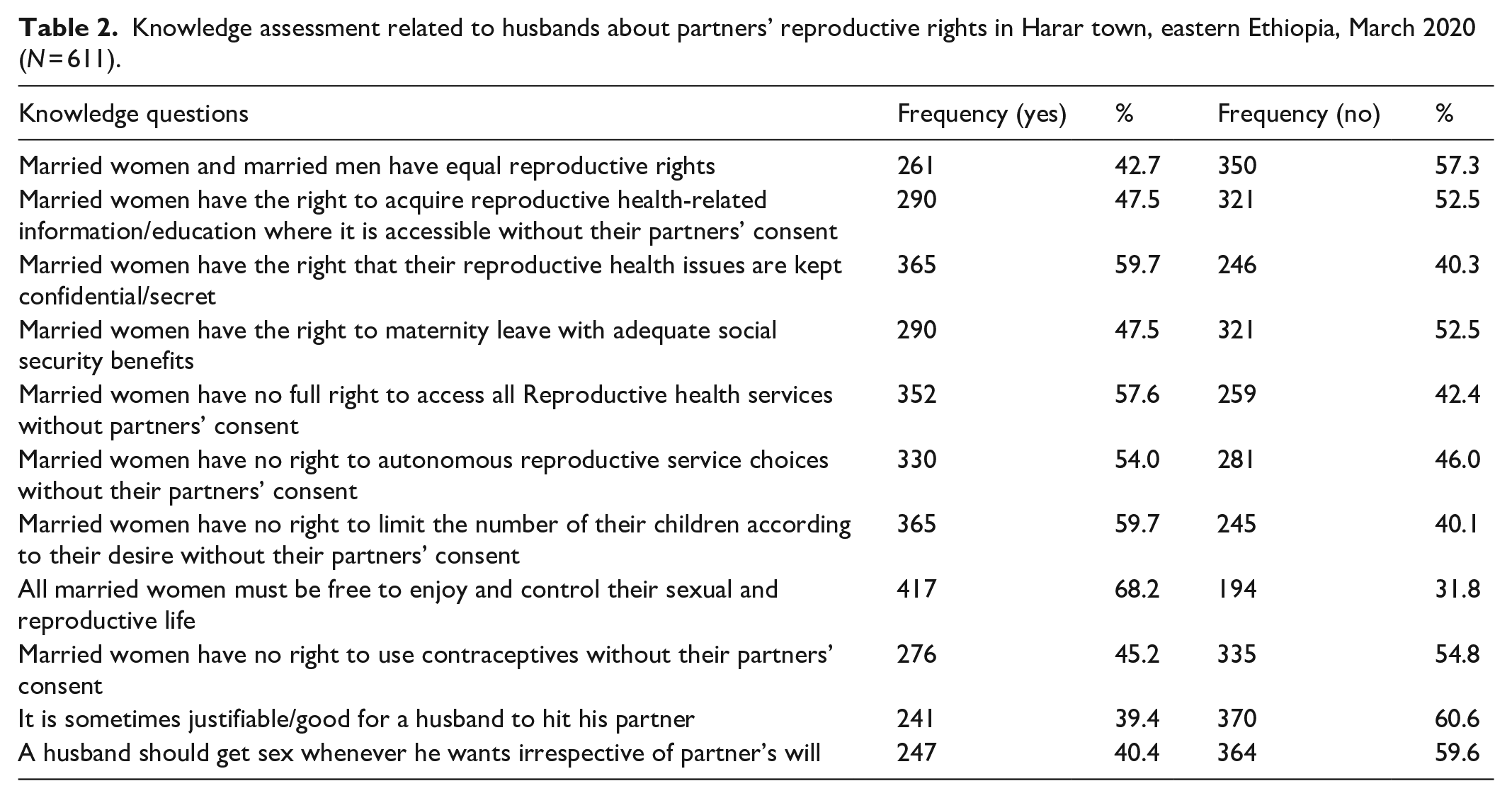
The mean knowledge score was 5.64 (SD ± 1.65) with a minimum score and a maximum score of 2 and 10, respectively. Accordingly, 48.3% (95% CI = 44.5%–52.2%) of the husbands were knowledgeable about the reproductive rights of women (Figure 1). Two hundred sixty-one (42.7%) participants responded that women and men have equal reproductive rights. More than two-thirds (68.2%) of husbands agreed that all married women must be free to enjoy and control their sexual and reproductive health (Table 2).

Knowledge of husbands about partners’ reproductive rights Harar town, eastern Ethiopia, March 2020 (N = 611).
Knowledge assessment related to husbands about partners’ reproductive rights in Harar town, eastern Ethiopia, March 2020 (N = 611).
Husband involvement in partners’ reproductive rights
Less than half of the husbands had good involvement in partners’ reproductive rights (40.1% (95% CI = 36.2%–44%)). The mean score of involvement was 3.53 (SD ± 1.65). The minimum and maximum scores were 1 and 7, respectively. The majority (70.0%) of the study participants did not support the use of contraceptive methods for their partners, and 328 (53.7%) did not support reproductive education access to their partners. However, 346 (56.6%) participants supported partners in using reproductive services such as prenatal care, facility-based delivery, and postnatal care (Table 3).
Response of husband involvement questions about partners’ reproductive rights in Harar town, eastern Ethiopia, March 2020 (N = 611).

The reasons for the non-involvement in the reproductive rights of women were being busy with other life issues, religion, living in different places, lack of knowledge, and money as presented in Figure 2.

Reasons for non-involvement of husbands in partners’ reproductive rights for each question in Harar town, eastern Ethiopia, March 2020 (N = 611).
Factors associated with husband knowledge in partners’ reproductive rights
In the multivariable logistic regression analysis, social media use, discussion on reproductive health, and type of nearby health facility were found to be significantly associated with husbands’ knowledge of the reproductive rights of women. Male partners who used social media were nearly five times (AOR = 4.97, 95% CI = 2.79–8.85) more likely to be knowledgeable than their counterparts. Partners who had an open discussion on their reproductive health were two times (AOR = 2.33, 95% CI = 1.60–3.39) more likely to be knowledgeable about partners’ reproductive rights than those partners who did not have a discussion. Moreover, male partners who had a nearby hospital (AOR = 3.21, 95% CI = 1.23–8.36) and health post (AOR = 2.86, 95% CI = 1.20–6.94) were approximately three times more likely to be knowledgeable about partners’ reproductive rights compared with their counterparts as shown in Table 4.
Factors associated with knowledge of husbands about partners’ reproductive rights in Harar town, eastern Ethiopia, March 2020 (N = 611).

COR: crude odds ratio; AOR: adjusted odds ratio.
Significant at: *p < 0.05; **p < 0.001.
Factors associated with husband involvement in partners’ reproductive rights
In the multivariable logistic regression analysis, discussion on reproductive health, experience, age, and social media use were significantly associated with male partners’ involvement in the reproductive rights of women. Male partners who had experience in using reproductive services were two times (AOR = 2.15, 95% CI = 1.52–3.03) more likely to be involved in partners’ reproductive rights compared with partners who did not have such experiences. Furthermore, male partners who discussed reproductive health with their wives were two times (AOR = 1.95, 95% CI = 1.35–2.82) more likely to be involved in partners’ reproductive rights compared with partners who did not have such a discussion. Moreover, husbands who had used social media were 1.74 times (AOR = 1.74, 95% CI = 1.05–2.89) more likely to be involved in partners’ reproductive rights than those partners who did not use social media. Moreover, those who were in the age group between 40 and 49 years were two times (AOR = 1.99, 95% CI = 1.19–3.32) more likely to be involved in partners’ reproductive rights compared to their counterparts (Table 5).
Factors associated with the involvement of husbands on partners’ reproductive rights in Harar town, eastern Ethiopia, March 2020 (N = 611).

COR: crude odds ratio; AOR: adjusted odds ratio.
Significant at: *p < 0.05; **p < 0.001.
Discussion
In the United Nations 36 2030 Agenda for Sustainable Development, the international community has established the SDGs and set the target for countries to reduce the maternal mortality ratio to less than 70 per 100,000 live births by 2030. Ethiopia has declared its commitment to achieve SDG targets. This indicates that Ethiopia needs to accelerate the progress through expanding initiatives with a men-inclusive approach and promoting their involvement in the reproductive health of women. Therefore, a holistic approach is required. If men are involved and supported as equal partners, better outcomes in sexual and reproductive health and right indicators, such as contraception acceptance, safer sexual behaviors, use of reproductive health services, and reduction in sexual and reproductive health-related morbidity and mortality, can be expected. 37
This study aimed to assess husbands’ knowledge and involvement in the reproductive rights of women in Harar, eastern Ethiopia. In this study, 48.3% (95% CI = 44.5–52.2) of husbands were knowledgeable about the reproductive rights of women. This finding was in agreement with a study conducted in northern Ethiopia (Shire town, 47.1%). 38 This might be due to the similarity of the community health development army and health extension workers (HEWs) in which they are promoting, creating awareness, and developing social media access. However, this finding was lower than that reported in studies conducted in Ghana (53.8%), 8 southern Ethiopia (Wolaita Sodo, 54.5%), 7 and northern Ethiopia (Gonder, 57.7%). 39 This finding was higher than that reported in studies conducted in India (9.1%) 35 and northwest Ethiopia (Adet Tana Haik, 25.96%). 40 This disparity might be due to the differences in sample size, socio-economic, cultural, religious, and level of education and awareness.
Moreover, about 40.1% (95% CI = 36.2–44.0) had good partners’ reproductive rights involvement. This finding was in line with studies conducted in Bangladesh (40%), 22 southern Ethiopia (Bale zone, 41.4%), 24 and Afar, Ethiopia (42.2%). 29 This agreement might be because there is a rising development intervention in many of these countries such as community health promotion, awareness creation, and the development of social media access. However, this finding was lower than that reported in studies conducted in Tanzania (50.6%) 29 and Nepal (57.6%). 41 This finding was higher than that of a study conducted in Ethiopia (Harar, 19.7%). 21 This difference might be due to differences in socio-economic, socio-cultural, level of education, time of the study, accessibility, and implementation of reproductive health services.
Male partners who had used social media were five and two times more likely to be knowledgeable and involved in partners’ reproductive rights compared to their counterparts, respectively. This finding was in line with that of a study conducted in Bangladesh.22,42 A possible explanation might be providing continuous and multidimensional community awareness through social media, particularly on reproductive rights, empowerment of women, and individual rights increase male partners’ knowledge and involvement in women’s reproductive rights.9,22
Moreover, male partners who had a hospital and health post nearby were almost three times more likely to be knowledgeable about partners’ reproductive rights. This is because access to health facilities can provide information, and reproductive health services to the nearby community, which increases husbands’ knowledge and involvement in their partners’ reproductive rights. In addition, the accessibility of nearby health facilities can change the perceptions, beliefs, health norms, and practices of male partners toward women’s reproductive rights.8,39,43 Furthermore, male partners who had discussed with their wives reproductive health were two times more likely to be knowledgeable and involved in women’s reproductive rights. This finding is in agreement with studies conducted in Bangladesh 22 , India, 44 and Kenya. 45 This is the fact that an open discussion of male partners with women’s reproductive rights could increase the level of knowledge and involvement in women’s reproductive rights. In addition to this, a discussion between partners resulted in discussing their reproductive issues with health care providers, and this increased knowledge and involvement of husbands’ on women’s reproductive rights.16,39,45
Male partners aged 40–49 years were almost twice as likely to be involved in partners’ reproductive rights. This finding is in line with that of a study conducted in Ghana. 13 In this study, the majority were mature age, and the level of education was secondary and above that might increase their involvement in partners’ reproductive rights.
As per this study, male partners’ educational levels, occupation, access to reproductive education, and experience of using reproductive services were not significantly associated with husbands’ knowledge and involvement in partners’ reproductive rights. This contradicts with studies conducted in India, 35 Bale Zone, Ethiopia, 24 Arba Minch, Ethiopia, 46 Bangladesh, 22 and southern Ethiopia. 7 The reason might be a disparity in the study sample and community health nurses in India and HEWs in Ethiopia play a pivotal role in this difficulty.3,16,25
This study had some limitations; due to the study’s cross-sectional nature, it did not show causal relationships between variables. As we had used the self-reporting (interview response) method, recall bias is also a limitation. It might also have a social desirability bias. The absence of an internationally validated level of knowledge and involvement is another limitation of this study. However, scientific procedures were used to minimize the possible effects of these limitations such as using easy and simple words to understand, giving time to memorize, and explaining the aims of the study to minimizing sensitive words. In addition, we had provided intensive training for data collectors and supervisors before the actual data collection on how to approach and interview the participants. Therefore, using appropriate and scientific procedures at the time of interviewing participants addresses these limitations.
Conclusion
Less than half of the husbands were knowledgeable and involved in their partners’ reproductive rights. The use of social media, the type of nearby health facility, and spousal discussion of reproductive health showed a significant association with husbands’ knowledge of partners’ reproductive rights. Moreover, partners’ discussion on reproductive issues, the experience of reproductive service use, social media use, and age 40–49 years showed a significant association with male partners’ involvement in partners’ reproductive rights. Hence, emphasis should be placed on awareness creation through effective media utilization to improve male partners’ knowledge and involvement in women’s reproductive rights. Moreover, improving the accessibility of nearby health facilities working on reproductive health service utilization, women empowerment, and open discussions between partners are crucial to increase the knowledge and involvement of husbands.
Footnotes
Acknowledgements
The authors thank Haramaya and Dire Dawa Universities for their financial and unreserved technical support. The authors also extend their gratitude to the Regional Health Bureau, district heads, and the study participants for collaborations. Last but not the least, the authors also thank friends for their wonderful feedback on the manuscript’s scientific content.
Authors contributions
AM, YD, and TA conceived and designed the study. AD drafted the manuscript. AS, YB AD, and YD extensively reviewed the manuscript and incorporated intellectual input. All authors read, provided feedback, and approved the final version of the manuscript.
Availability of data and materials
All the data of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the Institutional Health Research and Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences, Haramaya University. Following approval, a written official letter of cooperation was given to the district administrators. The administrators were informed about the objective of the study including the risks, benefits, and confidentiality issues.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Haramaya University, Ethiopia. The funder has no role in the study selection, data collection, analysis, conclusion, and recommendation.
Informed consent
Informed written consent was obtained from all the participants. Furthermore, confidentiality was assured throughout the process.