
Abstract
Background:
Outbreaks of healthcare-acquired infections have been linked to contaminated medical devices such as electronic thermometers, sphygmomanometers, stethoscopes, latex gloves, masks, neckties, white coats and other.
Objective:
The aim of this study was to assess non-critical healthcare tools as a potential source of healthcare-acquired bacterial infections and associated factors in public health hospitals of Harar, eastern Ethiopia from March 2016 to February 2017.
Methods:
A hospital-based cross-sectional study was conducted on 212 non-critical healthcare tools owned by different health professionals. The data were collected from each owner using self-administered questionnaire. Swab specimens were collected from 187 stethoscopes and 25 sphygmomanometers using sterile cotton tips. Bacterial investigation and antimicrobial susceptibility tests were performed using standard culture tests. The data were double entered into EPI-Data version 3.1 and exported into the Statistical Package for Social Sciences version 16 for analysis.
Result:
The overall prevalence of non-critical healthcare tool contamination was 53.8%. A total of 137 bacterial strains were isolated. Staphylococcus aureus was the most frequent isolate (35%). Resistance to two or more different classes of antimicrobial was found to be 19.3%. The proportion of stethoscopes or sphygmomanometers contamination owned by the health professionals who were not cleaned regularly before and after examining each patient was found to be high (77%). The majority of non-critical healthcare tools used by health professionals working in the intensive care unit were contaminated (75%) followed by medical wards (73.5%).
Conclusion:
This study confirmed that the majority of the stethoscopes and sphygmomanometers were contaminated with pathogenic bacteria known to be associated with healthcare-acquired infections. Most of the healthcare workers did not practice stethoscope and sphygmomanometers disinfection. Strict and careful decontamination of stethoscopes and sphygmomanometers need to be in place before use.
Background
Healthcare-acquired infections (HCAIs) are a major public health problem worldwide and remain a significant hazard for hospitalized patients and healthcare workers, particularly in developing countries like Ethiopia, where resources and the awareness of infection prevention and control are limited. It has long been recognized as crucial factors bedeviling the quality and outcomes of healthcare delivery.1,2 Healthcare workers can transmit pathogenic microorganism including antibiotic-resistant pathogens through their hands and contaminated medical devices such as electronic thermometers, sphygmomanometers, stethoscopes, gloves, masks, neckties, pens, badges and white coats.2–6
Medical equipment used in the non-critical care setting is less likely to have standard disinfection and cleaning protocols than equipment in the critical care setting. Thus, medical care equipment is more likely to carry a considerable number of pathogenic bacterial strains. 7 The contamination of stethoscope particularly the diaphragm is reported mainly due to lack of regular disinfection (before and after examining each patient). 8 Furthermore, antibiotic-resistant bacteria may be transmitted from one patient to another through medical devices. 9 Stethoscope is an important instrument; if used without disinfection, it might bring the risk of infection to the patient and may continuously impose the risk serially to all patients. Stethoscopes used by medical practitioners, students and health workers have been shown to be a potential vector in the transmission of HCAIs. The disinfection of devices is not done as a routine by most health professionals.10,11 Draping of stethoscopes around the neck is commonly seen as a practice, resulting in the risk of recontamination of the diaphragm of the stethoscope from unclean earpieces, with normal flora and pathogenic bacterial strains harboring the ears of the healthcare workers. A single stethoscope often used for all inpatients and outpatients. The universal and unavoidable use of the stethoscope and its direct contact with multiple patients makes it an important potential factor in the dissemination of microorganisms from one patient to another.12,13
In resource-poor settings such as most developing countries, rates of HCAI exceed 20%, 14 but available data are scanty and more research is urgently needed in developing and transitional countries.
Healthcare workers often overlook non-critical healthcare tools including stethoscopes and sphygmomanometers as sources of infection. Studies have, however, demonstrated a significant risk of transmission of HCAI with these devices. 15
Patients who acquire HCAIs require additional diagnostic tests, therapeutic treatments and prolonged hospital stay. The Centers for Disease Control and Prevention (CDC) states that cleaning and disinfecting environmental surfaces are fundamental in reducing their potential contribution to the incidence of HCAIs. 16
Identifying the bacterial pathogens causing HCAIs from non-critical healthcare tools and their antimicrobial susceptibility pattern would help to make awareness of the magnitude of the problem and inherent dangers associated with HCAIs. It would also help to reduce the exposure of the hospitalized patient to multidrug-resistant pathogens in the hospital, and thus improve the clinical condition of the patients. There was a scarcity of data on non-critical healthcare tools used by staffs and students as a potential source of healthcare-acquired bacterial infections in eastern Ethiopia. This study was aimed to assess non-critical healthcare tools (stethoscopes and sphygmomanometers) used by staffs and students as a potential source of healthcare-acquired bacterial infections and associated factors in public hospitals of Harar, eastern Ethiopia.
Materials and methods
Study area and period
The study was conducted from March 2016 to February 2017 at two public hospitals (Hiwot Fana Specialized University Hospital and Jugal Hospital). Hiwot Fana Specialized University Hospital is a large and complex teaching hospital found in Harar town. The hospital is expected to serve about 5.8 million people in the eastern part of Ethiopia. A total of 300 students from different departments in Haramaya University, College of Health and Medical Sciences, Jigjiga University, Harar Nursing College and other private institutions attached to the hospital for practical training. Jugal Hospital is found in the Harari Regional State. It also serves as a practice site for Haramaya University students. It has a total number of 120 beds. 17
Study design and population
A cross-sectional study was conducted among stethoscopes and sphygmomanometers used by students and staffs in the outpatient department (OPD), pediatric, surgery, gynecology and obstetrics and internal medicine wards.
Sample size determination
The sample size for stethoscope contamination was determined using a single-population proportion formula considering the prevalence of contamination reported in Jimma University Specialized Hospital (85.8%), 18 95% confidence level and a 5% margin of error. The final sample size for stethoscope contamination was 187. While all sphygmomanometers used in selected wards of the two hospitals during study were included in the study.
Sampling technique
Health professionals (specialist, general practitioners, health officer and nurses) and students along with their respective stethoscopes were allocated proportionally to Hiwot Fana Specialized University Hospital and Jugal Hospital based on their total number. Accordingly, 149 from Hiwot Fan Specialized University Hospital and 38 from Jugal Hospital were selected using simple random sampling (lottery) method by using the attendance sheet of the respective wards as a sampling frame.
Method of data collection
A structured questionnaire developed from different kinds of literature2,16,18–21 was used as a data collection tool. Before the actual data collection was pursued, the questionnaire was pretested on 5% of the sample size out of the study area to ensure its validity. The questionnaire was amended based on the pretest feedback. A questionnaire consisted of two parts: socio-demographic characteristics and infection prevention/ disinfection practice
The data were collected using a self-administered questionnaire after written consent was obtained from each participant. Then, a swab sample was collected from each stethoscope or sphygmomanometers at a convenient time for health professionals when they were free of disturbance in the hospital. The participants were not informed the date of sample collcetion.
Before taking a swab from the noncritical tool, both hands of data collectors were cleaned with an alcohol-based instant hand sanitizer and powder-free, disposable, gloves were worn throughout the work per sample to prevent contamination. Sterilized cotton swab moisten by sterile normal saline was rotated and swiped from overall parts of the stethoscope and sphygmomanometers’ area. The swab was placed immediately in Amie’s transporting media. The collected samples were coded by a unique identification number and transferred to the Bacteriology Laboratory of the Department of the Medical Laboratory Sciences, Haramaya University within 30 min of collection.22,23
Culture isolation and identification of bacteria
Aseptically collected sample was streaked onto blood agar and MacConkey agar plates (Oxoid, LTD, UK) following the standard techniques described. 22 The inoculated plates were incubated aerobically at 37°C for 24–48 h. Primary isolation of bacteria was made based on their colony characteristics and Gram reaction. Further identification of the bacterial organism to species level was carried using biochemical tests.24,25 In brief, Gram-negative bacteria were identified by doing a series of biochemical tests like triple sugar iron agar, indole, Simmon’s citrate agar, oxidase, urease test, Motility–Indole–Urea (MIU) and methylene red. Mannitol salt agar, catalase and coagulase tests were used for identification of Gram-positive bacteria. Colony count ⩾20 CFU/diaphragm was considered as significant contamination. 18
Antimicrobial susceptibility test
The antimicrobial susceptibility test was done using the Kirby–Bauer disk diffusion method based on the Clinical Laboratory Standards Institute (CLSI) guideline. 24 In brief, pure culture (4–5 colonies) were added to a sterile tube containing 5 mL of normal saline (0.85% NaCl) and mixed gently until it forms a homogeneous suspension equivalent to 0.5 McFarland standards. Sterile cotton swabs were dipped into the suspension, excess fluid was removed by gentle rotation of the swab against the inner surface of the tube, and the bacterial suspension over the entire surface of Mueller Hinton agar (Oxoid Ltd, UK) was inoculated and left at room temperature for 3–5 min to dry. Antimicrobial disks such as cefoxitin (30 μg), ciprofloxacin (5 μg), amoxicillin (30 μg), erythromycin (15 μg), norfloxacin (10 μg), cefotaxime (30 μg), tetracycline (30 μg), trimethoprim–sulfamethoxazole (1.25/23.75 µg) and vancomycin (30 μg) were placed at least 24 mm away from each other and 15 mm from the edge to avoid the overlapping zone of inhibition. It was gently pressed to ensure that the disk attached to the agar surface of the plate. Inoculated plates were incubated at 37°C. After overnight incubation, the diameter zone of inhibition was measured using a digital caliper. The results were read to the nearest millimeter and interpreted as resistance (R), intermediate (I) and sensitive (S) based on CLSI criteria. Bacterial isolates resistant to two or greater than two from a different class of antimicrobial group were classified as resistance to two or more antimicrobial. 24
Data processing and analysis
Data were double entered into EPI-Data version 3.1 and transferred to the Statistical Package for Social Science (SPSS) software version 16 for analyzing. Descriptive statistics were used to summarize different variables and presented in the form of texts and tables. Bivariate and multivariate logistic regressions were carried out to identify factors associated with a bacterial contamination of stethoscope or sphygmomanometers. Those variables in the bivariate logistic regression analysis with a p value less than or equal to 0.25 were considered as a candidate for multivariate logistic regression analysis. A variable with p value less than 0.05 at 95% confidence interval (CI) in the multivariate logistic model was considered as statistically significant.
Quality assurance
All culture media were prepared following the manufacturer’s instructions, and their sterility was checked by incubating 3%–5% of the batch at 37°C overnight and observed for growth. Culture media, which showed any growth, was rejected and replaced by a new sterile batch. The reference strains such as Staphylococcus aureus (ATCC25923) for blood agar and Escherichia coli (ATCC-25922) and Pseudomonas aeruginosa (ATCC-27853) for MacConkey agar were used for quality control of culture. Depending on the bacterial species, culture media was incubated aerobically at 35°C–37°C and observed for the degree of growth, size of colonies and other characteristics.
The quality of antimicrobial agents was checked against S. aureus (ATCC 25923) and E. coli (ATCC 25922). The inhibition zone was felt within the pre-set standard zone of inhibition. 24 The questionnaire was pretested on 5% of the sample size out of the study area to ensure its validity. Training on data collection and samples was given to data collectors by investigators before commencement of actual data collection. The data collection was closely supervised by supervisors and the investigators. Completeness of each questionnaire was checked daily during the data collection period. Double data entry was done by two data clerks into EpiData. The consistency of the entered data was cross-checked by comparing the two separately entered data.
Result
Sociodemographic characteristics
A total of 212 study participants along with their stethoscope or sphygmomanometer were participated in the study. The response rate was 100%; 117 (55.2%) were females. The professionals include medical students (134), clinical specialists, general practitioners and health officer (23), anesthetists (10) and nurses (45). These health professionals were working in different wards, namely, OPD (42), pediatrics ward (16), emergency ward (49), medical ward (49), surgical ward (26), gynecology and maternity wards (10) and intensive care unit (20) (Table 1).
Sociodemographic characteristics of study participants in Hiwot Fana Specialized University Hospital and Jugal Hospital, Harar, Ethiopia, 2017 (n = 212).

Infection prevention/disinfection practice
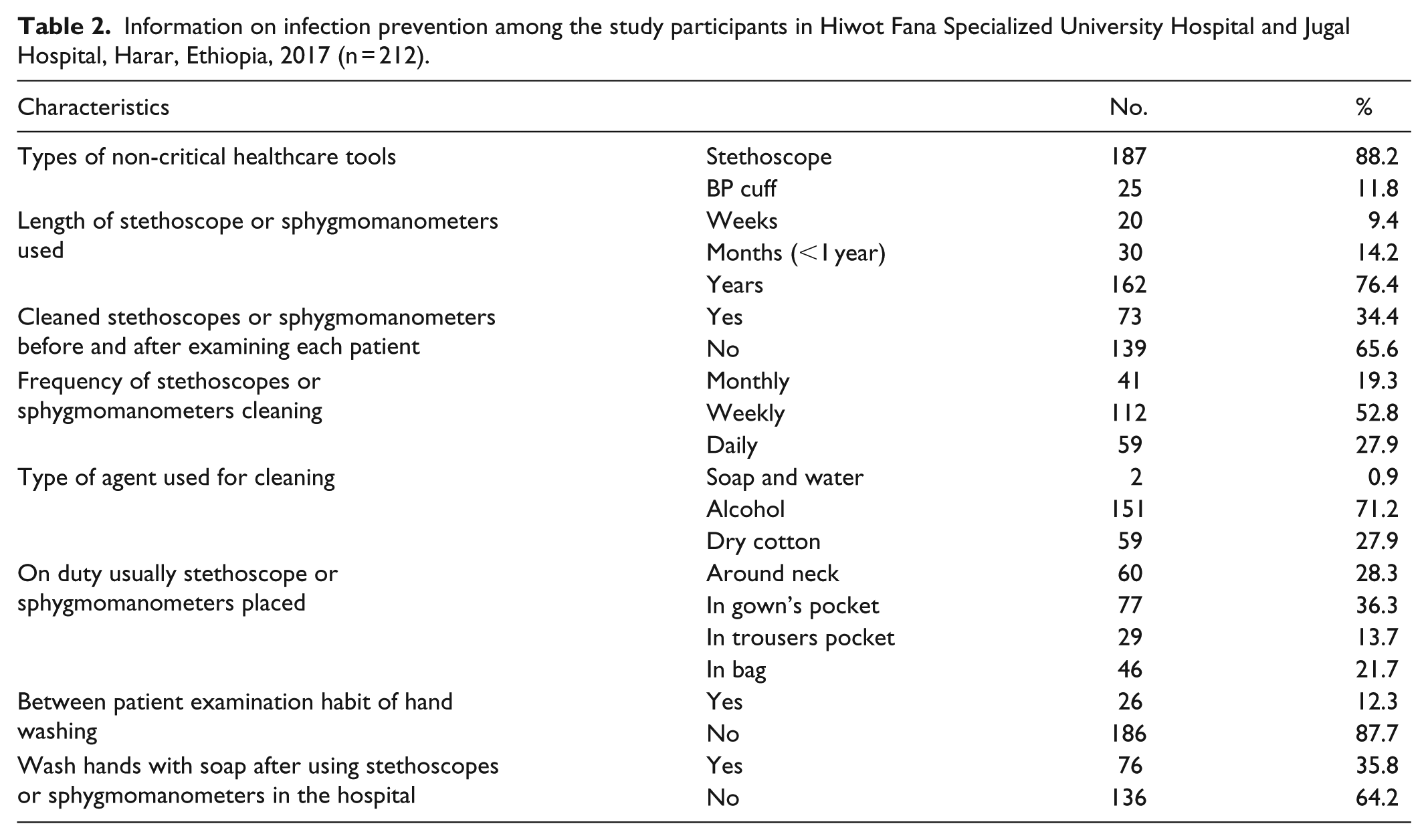
A total of 187 stethoscopes and 25 sphygmomanometers owned by different health professionals were examined for bacterial contamination. The majority (76.4%) of the stethoscope was used by the professionals for more than a year. About two-third of (65.6%) healthcare workers did not practice stethoscope and sphygmomanometers disinfection before and after examining each patient; 186 (87.7%) and 136 (64.2%) of the study participants have no habit of hand washing between patient examination and with soap after using stethoscope or sphygmomanometer, respectively (Table 2).
Information on infection prevention among the study participants in Hiwot Fana Specialized University Hospital and Jugal Hospital, Harar, Ethiopia, 2017 (n = 212).
The frequency of bacterial isolates
The overall prevalence of non-critical healthcare tool contamination was 53.8% (114/212). Of these, 101 (54.0%) and 13 (52%) were stethoscopes and sphygmomanometers, respectively. A total of 137 bacterial strains were isolated. S. aureus was the most frequent isolate (35%) among Gram-positive bacteria followed by coagulase-negative staphylococcus (CoNS; 16.8%) and Bacillus species (8.8%). Regarding Gram-negative bacteria, Klebsiella pneumonia (12.4%) were the most common isolates followed by P. aeruginosa (7.3%), E. coli (7.3%), Proteus spp. (6.6%) and Salmonella spp. (5.8%).
Factors associated with the contamination of non-critical healthcare tools
The proportion of stethoscopes or sphygmomanometers contamination used by health professionals who were not cleaned regularly their stethoscopes or sphygmomanometers before and after examining each patient was high (77%). The contamination of stethoscopes or sphygmomanometer used by health professionals working in the intensive care unit (75%) and medical ward (73.5%) was high compared with other wards. In multivariate analysis, gender, occupation, professional working department, cleaning of stethoscopes or sphygmomanometers before and after examining each patient and the frequency of stethoscopes or sphygmomanometers cleaning were found to be statistically significant (p < 0.05). Stethoscopes or sphygmomanometers used by males were 1.5 times more likely contaminated compared to females (adjusted odds ratio (AOR): 1.51, 95% CI: 1.81–12.14). Stethoscopes or sphygmomanometers which were not disinfected before and after the use for examining patient was six times more likely contaminated compared to those cleaned regularly (AOR: 5.95, 95% CI: 3.09–19.04). Stethoscopes or sphygmomanometers used in the intensive care unit (AOR: 1.97, 95% CI: 1.02, 9.63) and medical ward (AOR: 1.89, 95% CI: 1.06, 8.52) were two times more likely contaminated compared to their counterparts. Stethoscopes or sphygmomanometers used by medical students were about 1.5 times more likely contaminated compared with those used by the staffs (AOR: 1.49, 95% CI: 1.42, 8.02). Stethoscopes or sphygmomanometers disinfected monthly and weekly were four times (AOR: 4.01, 95% CI: 2.00, 11.58) and two times (AOR: 2.02, 95% CI: 1.81, 8.1) more likely to be contaminated with bacteria compared to those cleaned daily, respectively (Table 3).
Factors associated with stethoscopes or sphygmomanometers bacterial contamination among the study participants in Hiwot Fana Specialized University Hospital and Jugal Hospital, Harar, Ethiopia, 2017 (n = 212).

CI: confidence interval; BP: blood pressure.
Antimicrobial susceptibility pattern of the isolates
Overall, 137 bacterial isolates were tested against nine different commonly used antimicrobial for the treatment of bacterial infections. All P. aeruginosa isolates were 100% resistant to Amoxicillin and Cefotaxime. All P. aeruginosa and E. coli isolates were 100% sensitive to Norfloxacin; 25 (25%) of the Salmonella spp. showed resistance to Tetracycline and Vancomycin. All Salmonella isolates were susceptible to Ciprofloxacin.
More than 78% of K. pneumoniae and coagulase-negative Staphylococcus isolates were susceptible to Cefoxitin and Ciprofloxacin. Majority of Proteus species, Bacillus species and S. aureus isolates were susceptible to Norfloxacin. Relatively, S. aureus (8.3%) showed the least resistance against Norfloxacin (Table 4).
Antimicrobial susceptibility pattern of bacteria isolates from stethoscope or sphygmomanometers to commonly used antibiotic disks in Hiwot Fana Specialized University Hospital and Jugal Hospital, Harar, Ethiopia, 2017 (n = 212).
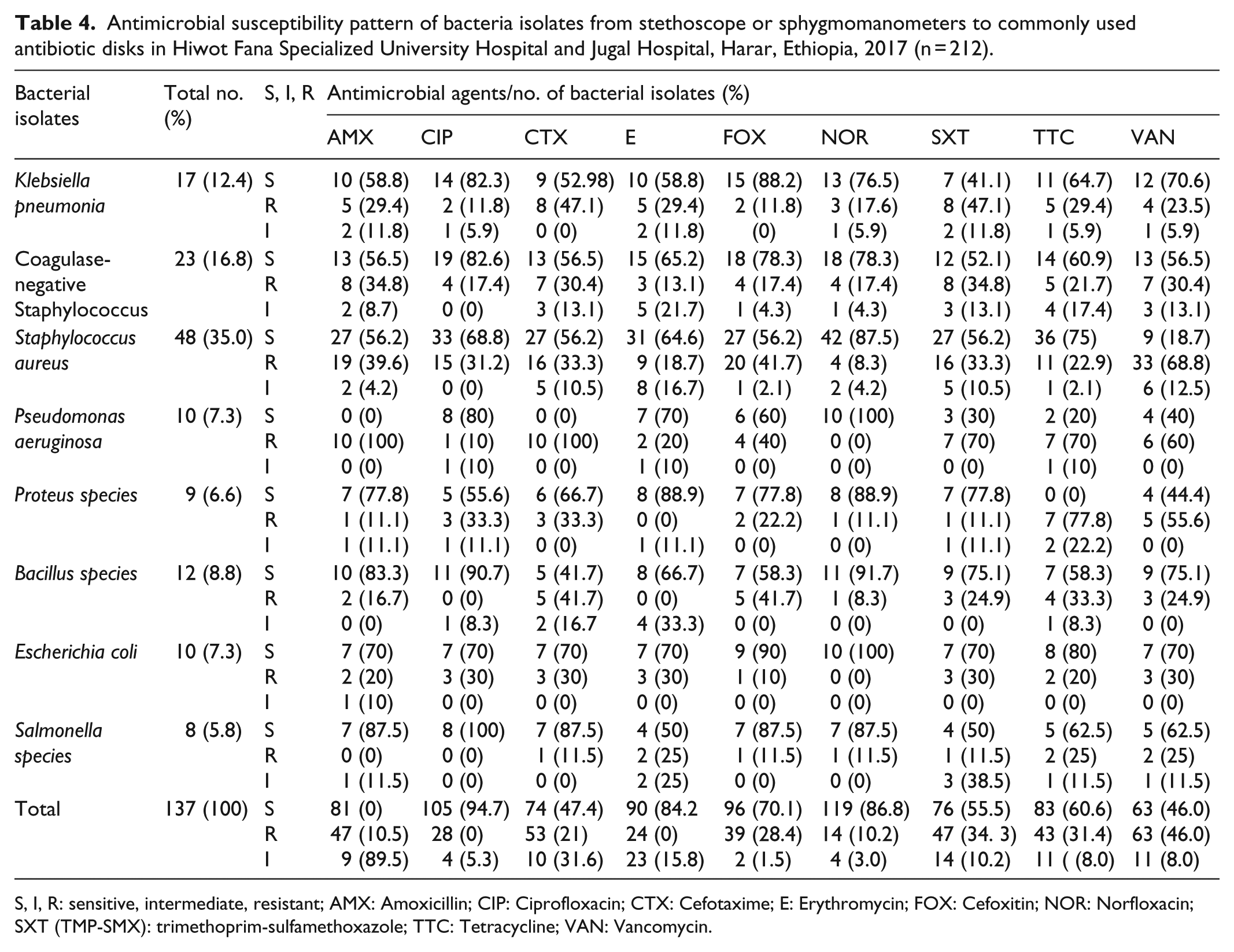
S, I, R: sensitive, intermediate, resistant; AMX: Amoxicillin; CIP: Ciprofloxacin; CTX: Cefotaxime; E: Erythromycin; FOX: Cefoxitin; NOR: Norfloxacin; SXT (TMP-SMX): trimethoprim-sulfamethoxazole; TTC: Tetracycline; VAN: Vancomycin.
Resistance to two or more different classes of antimicrobial groups
The overall prevalence of resistance to two or more antimicrobial was 16.8%. S. aureus (66.3%) was most predominantly showed resistance to two or more antimicrobial followed by coagulase-negative staphylococcus (39.1%) and P. aeruginosa (30%) (Table 5).
Multiple antimicrobial resistance of bacterial isolates from Stethoscope or Sphygmomanometers of health professionals to commonly used antibiotic disks in HFSUH and Jugal Hospital, Harar, Ethiopia, 2017 (n = 137).

Discussion
The introduction of medical devices for the management and treatment of diseases has contributed to the emergence of HCAIs with the consequence that put the patient into poor prognosis. The introduction of such devices is not wrong by itself, instead facilitates the medical procedures, but lack of commitment by the medical personnel to the infection prevention protocols was significant. 18 The implication of the findings is that the stethoscope and sphygmomanometers might be a vector playing an important role in the transmission of potentially pathogenic bacteria, as well as in the spread of antimicrobial-resistant strains in the hospital environment.
In this study, 55.6% of the stethoscopes and 60% of sphygmomanometers were contaminated with various types of bacteria which is almost similar with previous studies conducted by Kuhu Pal et al. 20 in Tertiary Care Hospital of Rural Bengal (52%) and Africa-Purino and his colleagues 26 in the Santo Tomas University Hospital (57%). The incidence of stethoscopes contamination was also in line with other observations.19,20,27–29 But lower compared to the previous studies reported by Marinella et al. 30 (100%), Wood et al. 31 (100%), Zuliani-Maluf et al. 32 (87%), Youngster et al. 33 (85.7%) and Uneke et al. 28 (80.1%). The variation could be due to the differences in the time of exposure, a number of patients contacted and adherence level of infection prevention protocol implementation.
In this study, the contamination of stethoscopes or sphygmomanometers used by health professionals who were not cleaned regularly before and after examining each patient was high (77%). The higher contamination was recorded among non-critical healthcare tools used by health professionals working in the intensive care unit (75%) and medical wards (73.5%). This finding was in line with Jimma University Specialized Hospital report 18 and other previous studies.21,28,30,34,35 In addition, male health professionals did not disinfect (cleaned) before and after examination, being student and monthly or weekly disinfection (cleaning) was found to be among the contributing factors to the contamination of non-critical healthcare tools.
A total of 137 pathogenic bacterial strains were isolated. Of them, 39.4% were Gram-negative bacteria which were almost similar to a study conducted at Jimma University Specialized Hospital. 18 But higher than other previous studies.15,28,36,37 S. aureus was the most common isolate over other potential pathogens such as coagulase-negative staphylococcus, Bacillus spp, K. pneumonia, P. aeruginosa, E. coli, Proteus spp and Salmonella spp. Most of the identified bacterial species were among the common isolates reported in the previous studies of medical equipment.15,28,36,37
Most of the bacteria isolated were resistant to different antimicrobials in the testing panel. The development of antibiotic resistance is worrisome and has been described as a serious public health concern. This is particularly the common case in developing countries where there is limited healthcare services, inadequate drug supplies, non-adherence to treatment strategies, self-medication and dubious drug quality that favor the emergence and persistence of antibiotic resistance. 38
All the P. aeruginosa isolates were resistant to two most commonly used antimicrobials (i.e. Amoxicillin and Cefotaxime). All P. aeruginosa and E. coli isolates were susceptible to norfloxacin; 25% of the Salmonella spp. showed resistance to tetracycline and vancomycin. However, all Salmonella spp. were susceptible to Ciprofloxacin, which was similar to the previous studies conducted at Jimma University Specialized Hospital, 18 Nigeria 28 and southwestern Ethiopia. 39
Sufficient emphasis on disinfection practices of non-critical medical equipment for patient care is mandatory. Lack of focus on the implementation of infection prevention and patient safety and the emphasis given to the topic in the medical education curriculum might be the possible reason for the lack of attention toward the issue and a high degree of contamination. This was also supported and indicated by several other studies.15,18,28,36,37 Similarly, our study indicated a high contamination rate of stethoscopes and sphygmomanometers with potential pathogens that may cause a variety of diseases. These bacterial strains were also resistant to commonly used antimicrobial agents.
This study has several limitations. The sample size of sphygmomanometers was too small. This might reduce the power of analysis to show whether there is a difference in the sphygmomanometers utilized and contamination. Only nine antimicrobial disks were used to determine antimicrobial susceptibility of the isolates that may affect the generalizability of the finding. The antimicrobial susceptibility testing was performed in vitro, which might not indicate in vivo sensitivity. In addition, the cross-sectional nature of the study limits the investigation to the level of the association between determinants and outcomes of interest. Hence, it was impossible to get information about a causal relationship with the majority of associated factors.
Conclusion
This study confirmed that the majority of the stethoscopes and sphygmomanometers were contaminated with pathogenic bacteria known to be associated with HCAIs. Furthermore, a large proportion of isolates are resistant to multiple classes of antimicrobial agents commonly prescribed in the hospital. Being male, failure to disinfect (clean) before and after examining each patient, working in the intensive care unit and medical ward, being a student, disinfecting (cleaning) monthly or weekly were factors contributed to the contamination of non-critical healthcare tools. An intervention on the actual factors contributed to the contamination of non-critical healthcare tool should be implemented to reduce the bacterial load and HCAIs. Most of the healthcare workers did not practice about stethoscope and sphygmomanometers disinfection before and after examining each patient. Providing continuous on-the-job training for healthcare workers on infection prevention, patient safety and regular disinfection of non-critical healthcare tools contributes for minimizing contamination. Strict adherence to the stethoscope and sphygmomanometers’ disinfection can minimize contamination and ensure improved patient safety in the hospital environment.
Footnotes
Acknowledgements
We would like to thank Haramaya University for financing this research work. Our thanks also go the study participants, individuals and organization that supports us in conducting this study.
Author’s Note
F.W. designed the study; participated in data collection, analysis, interpretation and write-up; drafted the manuscript and critically revised the manuscript. D.A. designed the study; participated in data collection, analysis, interpretation and write-up; drafted the manuscript and critically revised the manuscript. D.M. designed the study; participated in data collection, analysis, interpretation and write-up; drafted the manuscript and critically revised the manuscript. M.A. designed the study; participated in data collection, analysis, interpretation and write-up; drafted the manuscript and critically revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Haramaya University Colleges of Health and Medical Sciences Institutional Research and Ethical Review Committee (IHRERC23/2016). Based on the objective of the study, an official letter was sent to Hiwot Fana Specialized University Hospital and Jugal Hospitals. Confidentiality was maintained and all respondents’ questionnaire anonymously prepared.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was funded by Haramaya University.
Informed consent
The objective of the study was explained to each study participants. Those volunteered and signed the consent form were involved in the study. Written informed consent was obtained from all subjects before the study.