
Abstract
Introduction:
Certification of out-of-hospital deaths is challenging as physicians are often unavailable at the scene. In these situations, emergency medical services will generally transport the decedent to the nearest hospital. In 2011, a remote death certification program was implemented in the province of Québec, Canada. The program was managed through an online medical control center and enabled death certification by a remote physician. We sought to evaluate the implementation and feasibility of the remote death certification program and to describe the challenges we experienced.
Methods:
We retrospectively reviewed all remote death certification requests received at the online medical control center between 2011 and 2019. Data were collected from the online medical control center database and records. Feasibility was determined by evaluating the remote death certification rate.
Results:
Overall, 84.1% of remote death certification requests were realized, producing a total of 9776 death certificates. Male decedents accounted for 61.5% of remote death certification requests and were more likely than females to undergo a coroner’s investigation for cause of death (36.3% vs 20.8%, p = 0.017). Urban/mixed regions had higher rates of achieved remote death certifications (mean 87.3% vs 76.9%, p = 0.033) and putrefied bodies (mean 3.8% vs 2.2%, p = 0.137) compared to rural regions. Among unrealized remote death certification requests, the most common reason was failure of relatives to designate a funeral home (36.8%).
Conclusion:
Our 8-year experience with the remote death certification program demonstrates that despite facing numerous challenges, this process is feasible and offers a valuable option to manage out-of-hospital deaths. The remote death certification program is spreading in the remaining regions of Québec. Future studies will aim to quantify how much time this process saves for emergency medical services in each region of the province.
Introduction
Medical death certification is an essential process that provides documentation for administrative and legal purposes, as well as vital statistics for health policy and epidemiologic purposes.1,2 It is time-consuming to perform this process thoroughly and accurately due to the need to travel to the scene of death and collect the required information, much of which is often missing.2–4 As such, completing a death certification can pose a daunting task for most physicians and healthcare practitioners. Following the coronavirus outbreak in 2020, the British Medical Association partnered with the Royal College of General Practitioners to produce a protocol for remote assistance in verifying death. 5 This protocol allowed for a competent adult at the scene of death to receive assistance and guidance via video link from a physician that would enable the physician to safely and quickly verify the death. The impact of this protocol is yet to be determined.
In the Canadian province of Québec, physicians are responsible for pronouncing and certifying out-of-hospital deaths, except in rare cases. 6 Historically, as family physicians became less and less available to certify out-of-hospital deaths, it became necessary for emergency medical services (EMS) to transport the deceased to the nearest emergency department (ED) for medical death certification. This reduced the availability of emergency medical technicians (EMTs) for urgent calls, led to interference with law enforcement at crime scenes, and put an additional burden on hospital resources. To mitigate these issues, a provincial remote death certification (RDC) pilot program was implemented in 2011 by the Unité de coordination clinique des services préhospitaliers d’urgence (UCCSPU) at the direction of prehospital emergency services in order to medically certify a death. The UCCSPU is an online medical control (OLMC) center that employs trained nurses to support EMTs via telephone using specific protocols and to make referrals to ED physicians as necessary. 7 This pilot program was based on a protocol approved by the Québec College of Physicians, the Québec Ministry of Health and Social Services, and the Coroner’s Office. It requires a high level of coordination between EMTs, UCCSPU staff, and ED physicians since EMS in Québec is almost entirely provided by basic life support EMTs (BLS-EMTs); physicians are not present at the scene or in the ambulances.
To date, even if there are some studies reporting death certification remotely, no studies have reported on physician certification of death from a remote location in real time. Indeed, in the neighboring province of Ontario, registered nurses holding an extended certificate of registration are permitted to certify out-of-hospital deaths; 8 however, deaths in Québec must be certified only by a physician. Also, the World Health Organization (WHO) 9 recommends the use of verbal autopsy (VA) for countries where most deaths would not be documented. The VA is a method for gathering information about circumstances and causes of death in cases where no official cause of death could be determined live by a physician. This method based on a post hoc written/verbal information (conversations and interviews) and computer algorithms to assign a cause of death category does not rely on medical records and a physician, even a distant one, to certify the death as suggested by Bauni et al. 10 The RDC program seems therefore unique in the way it enables in real time the verification and certification of death, and while there is some evidence the RDC program has increased EMS availability, 11 the feasibility of this program has not been assessed. The objectives of this study were to evaluate the feasibility of the RDC program over an 8-year period of practice and to describe the challenges experienced with implementing the program.
Methods
Study design and population
This was a retrospective review of all consecutive EMS calls to the UCCSPU for out-of-hospital death certification in all participating regions of Québec between April 2011 and March 2019. Ethical approval (No.: 2021-773) was obtained from the Research Ethics Committee of the Centre de Recherche du CISSS de Chaudière Appalaches, Lévis (CISSS-CA Research Center), Lévis, Québec, Canada.
Implementation of the RDC program
In April 2011, a pilot RDC project was launched in the Chaudière-Appalaches region of the province of Québec (population 420,000) with approval from the Québec College of Physicians. A multidisciplinary meeting was held with stakeholders including local and regional police, the Coroner’s Office, funeral homes, ambulance companies, first responders, fire departments, and health communication centers. Following this meeting, EMS supervisors were trained on the RDC protocol and tasked to train and coach all regional EMTs. All physicians in the region were informed of the new procedures regarding RDC.
In December 2011, 8 months after the implementation, the Québec College of Physicians reclassified the pilot project as a provincial program available to all regions of Québec. Any region requesting to join the program had to first hold a multidisciplinary meeting of key stakeholders, followed by protocol training of regional EMS supervisors and EMTs. A signed agreement by regional health agencies established obligations and responsibilities for participation in the program, along with a mechanism for registering complaints. By 2019, 9 of the 17 socio-sanitary regions of Québec had joined the program, representing a population of over 3 million individuals (35% of the province population). Among these nine socio-sanitary regions, two regions are exclusively urban (>350 persons/km2) and four regions are primarily rural (<10 persons/km2). The remaining three regions are mixed with both urban and rural areas (>60% rural, 28–41 persons/km2).
Protocol and procedures of RDC
The protocol is based on the fundamental rule that a funeral home or coroner must take charge of the corpse once RDC is complete. 12 If this is not possible, RDC is not pursued or is halted prematurely. The decision algorithm for RDC is outlined in Figure 1. Details of the RDC protocol and procedures are described in Supplemental Table 1. Briefly, the RDC protocol is possible only if it is preceded by one of five following protocols. The first two protocols concern conditions where resuscitation maneuvers are initiated and then stopped after asystole. The third protocol deals with impossible resuscitation maneuvers (i.e. rigor mortis body). The fourth protocol concerns obvious deaths that exclude all possible resuscitation maneuvers. The final one covers all terminally ill patients with a do-not-resuscitate order.
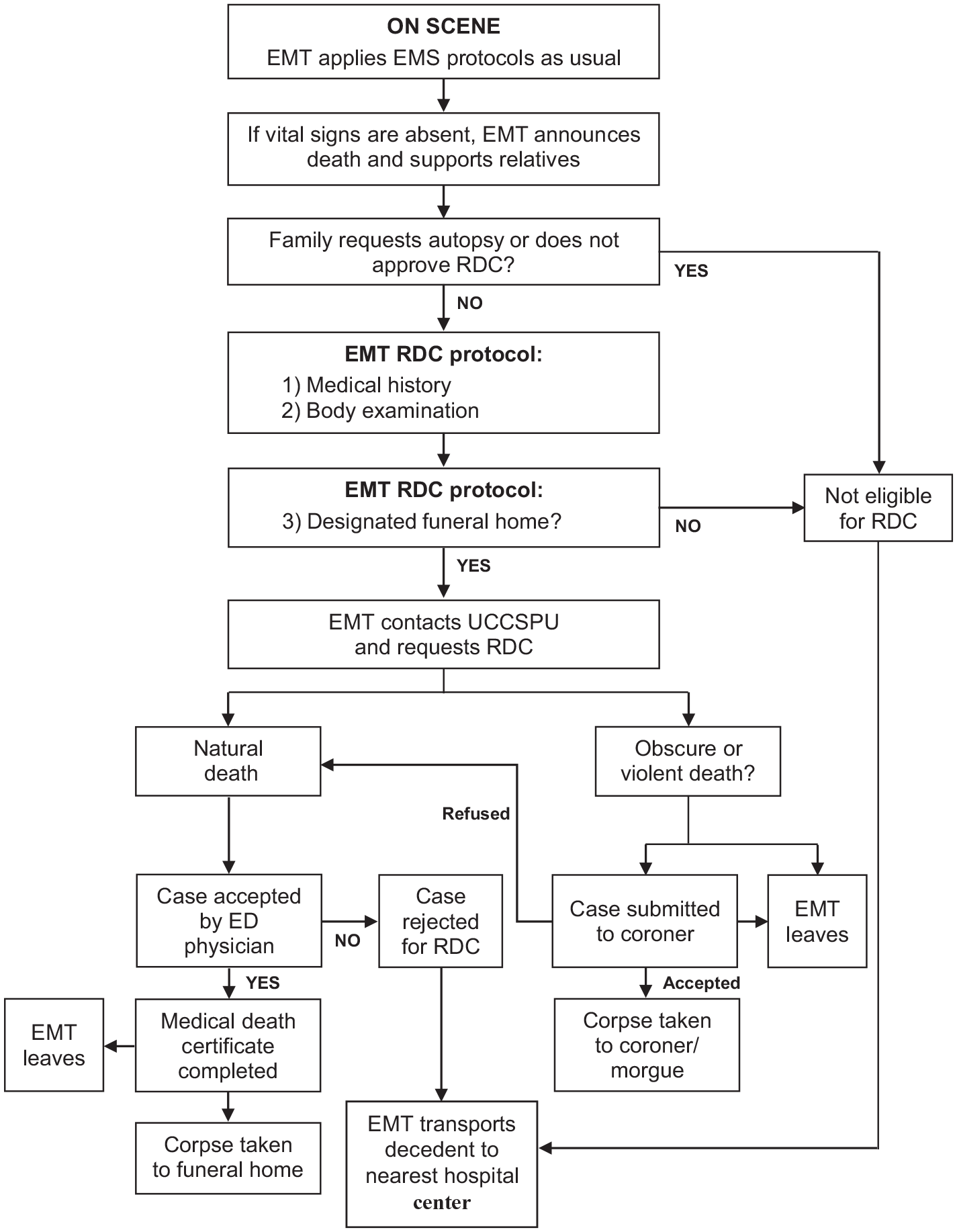
Decision algorithm for RDC.
Once RDC is completed, the UCCSPU nurse contacts Héma-Québec to provide the name and phone number of a relative in order to discuss potential tissue donation by the deceased. Héma-Québec is a non-profit organization that supplies blood and other biological human products to hospitals. The process of making referrals to Héma-Québec was revised in 2016; thus, we only report on referral data for the final 3 years of the study period.
Study definitions
In the province of Québec, a medical death certificate is an official document signed by a physician 6 who certifies the death, or a coroner, 12 with information regarding the deceased (name, gender, date, time and location) and the cause of death. The time and date of death are based on information gathered by EMTs on scene (family/witness) and from the examination of the body. The RDC protocol refers to the strict process that brings a physician to remotely medically certify a death. The RDC rate is the proportion of RDC requests that are realized. Finally, a putrefied body is characterized by a greenish and distended abdomen, swelling of the face and genitals, and fluid-filled blisters on the body. The percentage of putrefied bodies is defined as the proportion of RDC requests involving putrefied bodies since December 2014 (when data collection on putrefied bodies commenced). The rate per 100,000 population is based on the population in each region in 2019.
Data collection and statistical analysis
From the UCCSPU records and database, we extracted all variables of interest including the number of RDC requests, the number of requests realized, age, gender, reasons for unrealized RDCs, and findings from coroner cases. Feasibility was determined by evaluating the RDC rate. Descriptive statistics are presented as mean ± standard deviation (SD) and/or proportion (%). We used independent two-tailed t-tests (parametric test) to compare continuous variables and Pearson’s chi-square (χ2; non-parametric test) or Fisher’s exact test as appropriate to compare categorical variables. Cases were compared by gender (male vs female), by 10-year age groups, and by location (urban/mixed vs rural). Missing data were not included in the statistical analysis. A value of p < 0.05 was considered significant for all comparisons. All analyses were performed using SPSS 20.0 (Chicago, IL, USA).
Results
During the 8-year study period, there were a total of 11,622 EMT calls/requests for RDC (Table 1). The number of requests increased every year, from 244 requests at the start of the program in 2011/2012 to 2407 requests in 2018/2019. RDC rates ranged between 75.8% and 88.7% (mean 84.1% ± 4.5%) over the study period. It is important to note that for each new region that joined the program, it took around 2 years to adjust to the new protocol. Unexpectedly, we observed a high number of putrefied bodies over the study period, with requests for RDC involving putrefied bodies from natural deaths increasing from 17 in 2014/2015 to 98 in 2018/2019.
Rate of RDC and putrefied bodies between 2011 and 2019.

RDC: remote death certification.
Recording of putrefied bodies began in December 2014.
Table 2 shows the RDC rate and the number of putrefied bodies from natural causes of death per 100,000 population in each of the nine participating regions since they joined the program. Compared to rural regions, urban/mixed regions had higher rates of achieved RDCs (mean 87.3% ± 5.8% vs 76.9% ± 5.8%, p = 0.033) and putrefied bodies (mean 3.8% ± 1.7% vs 2.2% ± 0.9%, p = 0.137). Regional RDC rates varied from 70.9% to 93.0%. The three highest RDC rates were observed in predominantly urban/mixed regions (regions A, E, and F) with rates of 87.7%, 93.0%, and 92.8%, respectively, whereas the three lowest RDC rates were in rural regions (regions B, C, and G) with rates of 77.2%, 70.9%, and 74.9%, respectively. It should be noted that region I which is an urban region had been in the program for less than 4 months when this study began. The highest percentage of putrefied bodies was observed in region F (6.0%), a mixed region with 4.69 putrefied bodies per 100,000 population, followed by region E (5.1%), an urban region with 3.87 putrefied bodies per 100,000 population.
Regional RDC rates and putrefied bodies from natural causes of death.

RDC: remote death certification; U: urban region; R: rural region; M: mixed region with >60% rural population; km2: square kilometers; pop: population.
Data on number, %, and rate of putrefied bodies were available from December 2014 onward.
Table 3 shows the number of RDCs requested by EMTs and the RDC rate by gender, including the proportion of cases requiring investigation by a coroner. The majority of RDC requests involved males (61.5% vs 38.5%; p < 0.0001). Although the RDC rate was slightly higher among females (85.6% vs 82.7%), this difference was not significant (p = 0.232). A greater proportion of cases involving male patients were investigated by a coroner (36.3% vs 20.8%; p = 0.017). Regardless of the gender, the proportion of realized RDC cases investigated by a coroner was consistently around 30% throughout the study period.
RDC rate and coroner cases for deaths from natural causes, by gender.

RDC: remote death certification.
The number of RDCs that were realized, unrealized, or investigated by the coroner are shown by gender and age group in Figure 2. Regardless of the gender, the number of achieved RDCs (realized + coroner) was significantly greater with increasing age (0–89 years, p = 0.001 for women; 0–79 years, p = 0.006 for men). There was, however, a greater number of males in each 10-year age group between 0 and 79 years (p < 0.05). With respect to unrealized RDCs, the number of cases increased with age until peaking in the 60- to 69-year age group for men (p = 0.019) and in the 80- to 89-year age group for women (p = 0.012). For all age groups under 80 years of age, we observed a greater proportion of unrealized cases in patients who were male.

Cases of RDCs that were realized, unrealized, or sent to the coroner, by gender and age group.
The reasons for unrealized RDCs are described in Table 4. Since the start of the RDC program, approximately 16% of EMT requests were not realized. The most common cause was the absence of a designated funeral home (36.8% of cases), followed by the inability of the physician to identify the cause of death (20.0% of cases). A further 5.8% of cases had no funeral home designated and no cause of death identified. The challenges experienced over 8 years of the RDC program are described in detail in Supplemental Table 2.
Reasons for unrealized RDCs.

Other reasons included family refusal, UCCSPU overcharges, humanitarian reasons, peace officer or coroner orders, and paramedic or UCCSPU mistakes.
RDC: remote death certification; UCCSPU: Unité de coordination clinique des services préhospitaliers d’urgence.
Finally, Table 5 shows referrals to Héma-Québec for tissue donation from all regional hospitals of the nine participating regions and from the UCCSPU during the final 3 years of the study. Referrals to Héma-Québec increased by 85% (from 370 to 684 referrals) over this 3-year period and accounted for 26.3% of all referrals during this period. Although regional hospitals collectively made 73.7% of all referrals, the single hospital with the most referrals accounted for 9.4% of all referrals (results not shown). The large proportion of referrals from the UCCSPU can be attributed to nurses who systematically question each RDC request for possible tissue donation and subsequently contact Héma-Québec if eligible criteria are met.
Referrals for tissue donation to Héma-Québec by regional hospitals and the UCCSPU.

UCCSPU: Unité de coordination Clinique des services préhospitaliers d’urgence (online medical control center).
Discussion
To our knowledge, although some similarities exist with other processes8,9 collecting information to issue a medical death certification, this is the first study to report on the feasibility of a system where physicians in a real time remotely certify out-of-hospital deaths. In this 8-year retrospective review of the RDC program, we observed a mean annual RDC rate of 84.1%. Male decedents accounted for 61.5% of certifications, and 2.9% of cases involved putrefied bodies. The most common reason for an unrealized RDC was the lack of a designated funeral home (36.8%). Implementation and management of the RDC program required collaboration among a multidisciplinary team of stakeholders. We observed very few physician refusals for RDC during the study period, suggesting a high level of trust between EMTs and physicians. Indeed, the RDC protocol (mostly unchanged since implementation) precludes physician reluctance to pronounce death. Moreover, the high RDC rate and the fact that no “false decedents” were reported suggest the RDC protocol is appropriate, feasible, and applicable to new socio-sanitary regions of the province of Québec regardless of the population (urban, rural, mixed). Finally, tissue donation referrals made by the UCCSPU increased by 85% since this process was revised in 2016 and account for a significant proportion of all tissue donation referrals to Héma-Québec.
One of the main objectives of the RDC program was to increase the availability of EMS for urgent calls. 13 Previously, we analyzed a sample of 185 out-of-hospital deaths and demonstrated that a realized RDC in region A (mixed region) saved approximately 71 min for EMS, while a realized RDC in region C (rural region) resulted in a 28-min gain. 11 Regardless of the region, when a RDC is realized, the prehospital time gain includes transport time to the nearest ED, time spent in the ED, and time required for the EMT to return to their service area. 11 This overall reduction in EMS intervention time increases the availability of EMS to attend to other urgent calls. Moreover, by precluding transport of the corpse to the nearest hospital, 12 the RDC program decreases utilization of hospital resources. At the administrative level, this reduces the need to register the corpse by a clerk, to issue death certification forms, to contact a funeral home and/or coroner, and to occupy space within the hospital. From a clinical standpoint, the benefits include reduced need to involve hospital staff (i.e. no triage, no physician examination, and no meetings with family members). In addition, it avoids possible contamination of hospital staff who come in contact with the corpse. With the outbreak of the coronavirus pandemic in 2020, it became even more important to ensure the safety of hospital staff and to maximize the use of hospital resources in critical areas. Additional benefits of the RDC program include fewer administrative issues for relatives of the deceased and a reduced need for them to travel, as well as increased tissue donation referrals compared to when the deceased were transported to the nearest ED.
Over the 8-year study period, there were some expansions and several important improvements in technology and the methodology of the program. A custom software application was designed to enable faster and easier data collection at the scene by EMTs, and we implemented a system to automate data recording in the UCCSPU registry by nurses. These advances decreased the time required to process an RDC request by 30%. In 2013, the RDC program was expanded to include home care nurses for terminally ill patients. Rather than calling EMS when the patient passed away, the family calls their home care nurse who visits the home and calls UCCSPU to go through the RDC process. As a result of this change, EMTs were more readily available to respond to urgent calls. Physicians and nurses in Québec are working together to progressively implement the RDC program (using the same protocol and procedures) at nursing homes across the entire province. With all these improvements and new inclusions since its implementation, the RDC program draws attention of other socio-sanitary regions of the province of Québec which are planning to join the program.
Limitations
This study is subject to the known limitations of a retrospective analysis on an existing dataset and cannot be used to imply causality. As it was an observational study of all consecutive EMS calls to the UCCSPU requesting out-of-hospital death certification, sample size calculation/power analysis was not performed. Some cases were missing data and could not be included in the analysis. Although the RDC program was successfully implemented in nine regions of Québec (each with their local EMS system), our results may not be generalizable to other populations, jurisdictions or EMS systems.
Conclusion
Our 8-year experience with the RDC program demonstrates that this practice is feasible and offers a valuable option for remote out-of-hospital death certification despite numerous challenges. With regard to its feasibility, improvements and benefits, the RDC program is gaining more interest and is spreading to the remaining regions of Québec. Future studies are planned to quantify the amount of time that the RDC program saves for EMTs in the in-hospital and out-of-hospital settings.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211001145 – Supplemental material for Remote certification of out-of-hospital deaths in a Canadian Province: An 8-year experience of a novel practice
Supplemental material, sj-pdf-1-smo-10.1177_20503121211001145 for Remote certification of out-of-hospital deaths in a Canadian Province: An 8-year experience of a novel practice by Alain Tanguay, Johann Lebon and Denise Hébert in SAGE Open Medicine
Footnotes
Acknowledgements
The authors sincerely thank all members of the UCCSPU and Hôtel-Dieu de Lévis who assisted the research team in accessing records and data, as well as Percipient Research & Consulting for providing assistance with language editing.
Author contributions
All authors have participated in the work and have reviewed and agree with the content of the article. Dr Alain Tanguay is the guarantor of this work. He had full access to all the data and takes full responsibility for the integrity of the data and the accuracy of the analyses. Alain Tanguay and Johann Lebon performed the literature review, prepared and wrote the manuscript, and contributed to the discussion. Johann Lebon collected and analyzed the data. Denise Hebert and Alain Tanguay participated in data collection, reviewed the manuscript, and approved the final version submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Research Ethics Committee of the Centre de Recherche du CISSS de Chaudière Appalaches, Lévis (CISSS-CA Research Center), Lévis, Québec, Canada. The Approval No. is 2021-773.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fondation Hôtel-Dieu de Lévis, Lévis, Québec, Canada.
Informed consent
Written or verbal Informed consent from all subjects prior to study initiation was waived by the Research Ethics Committee of the Centre de Recherche du CISSS de Chaudière Appalaches, Lévis (CISSS-CA Research Center), Lévis, Québec, Canada, because of the retrospective nature of the study and it was study from UCCSPU records.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.