
Abstract
Acute appendicitis is among the commonest surgical emergencies seen in an acute setting. Individuals living with the Human Immunodeficiency Virus (HIV) and/or the Acquired Immunodeficiency Syndrome (AIDS) have an increased risk of encountering complications with acute appendicitis. We conducted a literature search using the words appendicitis and HIV in google scholar, Medline, Scopus and PubMed. The search also extended to cover HIV presented with acute appendicitis, their outcome during and following the management of acute appendicitis. Several studies showed that HIV is associated with a higher rate of acute appendicitis than the general population. HIV can directly affect the appendix, through opportunistic infections, immune reconstitution inflammatory syndrome associated with start of antiretroviral medication. High index of suspicion is needed to exclude conditions that mimic acute appendicitis (abdominal tuberculosis, pyelonephritis, cytomegalovirus, cryptosporidium, pneumococcus, Amoebic appendicitis and pill impaction). The clinical presentation may not be typical of acute appendicitis and can be associated with low white cell count and variable fever. The Alvarado score for predicting acute appendicitis can be used and more research is needed to establish cut-off point value. Computed tomography scan and ultrasound are widely used in clinical diagnosis. Importantly, acute appendicitis with HIV/AIDS can be associated with high rate of post-surgical complications like infections, delay of healing, perforation, peritonitis, intra-abdominal abscess and longer hospital stay. HIV/AIDS with acute appendicitis is complex condition. Therefore, we conclude that patients with known HIV and acute appendicitis should also be managed in close liaison with HIV physicians during, before and after surgical treatment.
Keywords
Epidemiology
In the general population, the prevalence of acute appendicitis (AA) is 0.1%, while with HIV/AIDS, the prevalence ranging from 0.6% to 3.6%, and this is estimated to be 8% absolute increase in the risk. Thus, AA occurs at higher rates in people living with HIV (PLWHIV). 1 Therefore, the increase in the prevalence of HIV/AIDS in developing countries was also associated with an increase in the incidence of AA. It is worth mentioning that HIV/AIDS patients are associated with a 15-fold higher risk of acute perforated appendicitis than the general population. 2 Despite the fact that surgical treatment of AA was associated with decline in mortality from 26% to less than 0.2 per 100,000 population currently, 3 complications associated with surgery and presence of comorbidities can lead to an increase mortality up to 5%.
AA is one of the most common surgical emergencies in the world attributed to the inflammation of appendix. This inflammation was thought to occur in case of appendix obstruction (infection, calculi, fecaliths, lymphoid hyperplasia, infection and presence of tumours). The obstructed appendix can lead to bacterial overgrowth which in turn can lead to a disseminated sepsis. Early AA predominantly has aerobic organisms while mixed flora is more common in late appendicitis. 4 Escherichia Coli, Bacteroides Fragilis, Peptostreptococcus and Pseudomonas species are linked with gangrenous and perforated appendicitis. 5 This research project was conducted as a review article. The authors searched on the literature using the following databases: PubMed, Medline, Scopus and Google scholar. These databases were searched using the keywords HIV/AIDS, appendicitis, presentation of appendicitis and perioperative care in HIV individuals. The authors searched also using combination of the following terms ((HIV) AND (AIDS) AND (appendicitis)) OR ((perioperative) AND (emergency) AND (immunocompromised)). The search was based on studies published in English language from 1981 to 2020, the abstracts and the articles were then screened. Articles were scanned and read; further relevant references in the reference lists are also included. This is still a new area for research and exploration; therefore, we have also included experience gained from observations in case reports.
HIV and appendicitis
HIV can increase the risk of AA in different ways. For instance, the HIV virus can directly target the appendix. 6 In other situations, the AA can be associated with opportunistic infections like Kaposi’s sarcoma, cytomegalovirus, Mycobacterium sp, Cryptosporidiosis and Salmonella typhi infection. 7 Importantly, the association of AA with HIV/AIDS is likely to occur on average older individuals than the general population. This likely attributed to the fact that PLWHIV are living longer with administration of antiretroviral medication. Therefore, surgeons are recommended to have high index of suspicion, as some patients may present with features not consistent with typical diagnosis of AA (less frequency of fever and a leucocytosis). For example, Duhamel et al. 8 showed that AA in an HIV-infected subject can mimic acute pyelonephritis secondary to obstruction. Perioperative care is essential and attention should be paid to the fact that these patients are at risk of developing complications like infection, delay in wound healing, perforation, intra-abdominal abscess, peritonitis and prolonged hospital stay, and ultimately all these complication may lead to an increase in mortality. 9 – 11
Another factor that can be associated with AA is immune reconstitution inflammatory syndrome (IRIS). This syndrome is associated with initiation of combined antiretroviral therapy (cART), which initiates a pathological inflammatory response to a previous infection resulting in appendicitis.10,11 Different mechanisms were also suggested to have role in the AA such as strong interferon response in the appendix may in part endorse a viral aetiology for the inflammation. Such observation can be also endorsed by the fact that the appendix is also part of the gut lymphoid tissues and this may further explain the involvement of the mucosal B and T cells and the replication of the HIV virus in the appendix.10,11 The role of immune status and CD4 count is also linked with AA. For example, Bedada et al. 11 showed that high postoperative complications and mortality in HIV patients with AA can be associated with a CD4 count <200. León-Ballesteros et al. showed that AA in PLWHIV can be associated with low prevalence of leukocytosis; however, their study showed that presence of both diabetes and HIV can be associated with high rate of surgical complications and an increase in hospital stay. 12 Therefore, early involvement of HIV physician in the management of these patients is highly recommended.
Importantly, it was shown that in a retrospective study in South Africa, 10 a perforated appendicitis was more reported in HIV-positive patients and this explains the need for more laparotomy in this group. In this study, it was shown that only in HIV patients, granulomatous inflammation was found. 10 In other studies, no difference was seen in the complication rate, length of hospital stays, and mortality between HIV-positive and HIV-negative patients.11,13 In one case study, pill impaction was found in appendiceal orifice with HIV patient. 14 In summary, it is possible that HIV can influence the appendix in different ways: (1) HIV virus directly affects the appendix, (2) opportunistic infections, (3) IRIS and (4) high levels of perioperative complications.
In addition to usual organisms, some unusual pathogens can precipitate appendicitis in HIV-infected patients. The causative agents including mycobacterium, cytomegalovirus, cryptosporidium, pneumococcus, Amoebic appendicitis, Pill Impaction and IRIS have been reported as AA in HIV patients.6,13 –15 There are different conditions in HIV patients which can present as abdominal pain or right iliac fossa pain. For instance, disseminated histoplasmosis and Kaposi’s Sarcoma can present as AA.16 –20
Clinical presentation
Clinical presentation can be variable but abdominal pain is the most common symptom with appendicitis.21,22 Other common clinical symptoms were right lower quadrant abdominal pain, nausea and vomiting. Some have atypical/nonspecific symptoms including indigestion, flatulence, diarrhoea and generalized malaise, and symptoms are mainly dependant on location of the appendix.
Investigations
Diagnosis of AA is based on clinical assessment, laboratory findings (C-reactive protein (CRP), white blood cell (WBC), but WBC is not always a reliable indicator such as in pregnancy) and imaging modalities like ultrasound and computed tomography (CT). Magnetic resonance imaging (MRI) is not widely used in the diagnosis of AA but can be used in further assessment of acute abdomen and pelvic pain.21,22
Role of the scoring system
The Alvarado score was widely used in establishing the diagnosis of the AA. The clinical score system has six clinical items and two laboratory measurements with a total 10 points (temperature, rebound tenderness, anorexia, nausea and vomiting, migration of pain to the right quadrant, and tow lab measurements are Leukocytosis > 10,000 and Leukocyte Left Shift). 23 In systematic review by Ohle, the cut-point of Alvarado score of 5 in general population without HIV was a good score to determine patients in need to be admitted to the hospital. Importantly, the score performed poorly when using the cut-point of 7 as point for progression to surgery. 23 Sobnach et al. 24 showed that cut-point of 8 can be used accurately to predict the diagnosis of appendicitis in HIV patients. However, further research is needed to assess the role of Alvarado score in the diagnosis of AA in HIV.
The diagnosis can be established from the history, clinical examination and simple blood investigations like CRP and WBCs. In case of doubt about the diagnosis, it is advisable to perform imaging studies such as abdominal ultrasound or CT. 25 The accuracy of ultrasound is estimated to be between 71% and 97%, while the accuracy rate of CT scanning is between 93% and 98%. 26 These image modalities were also used in HIV patients for the diagnosis of appendicitis (Figure 1).
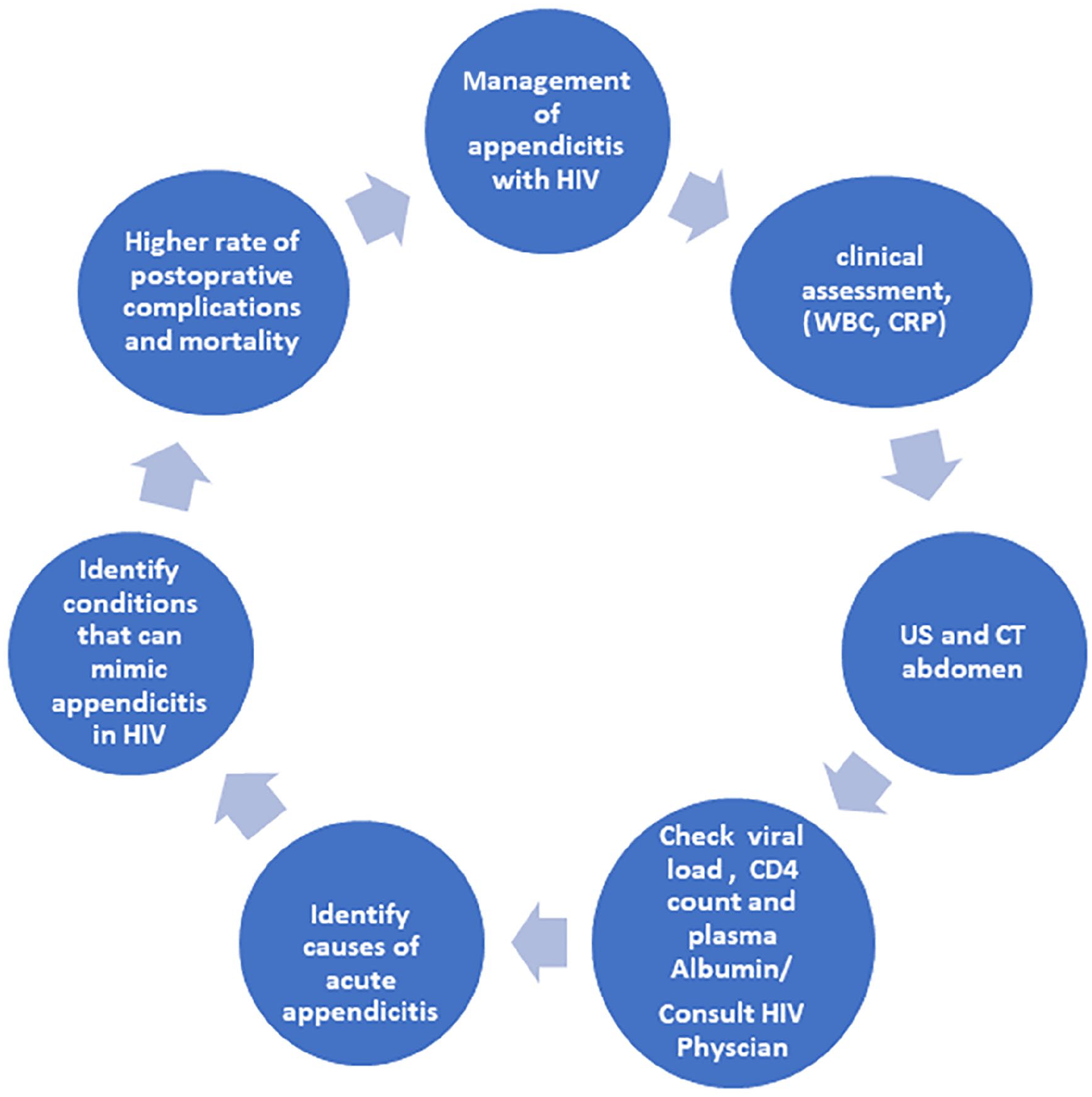
The steps in the management of acute appendicitis in individuals living with HIV.
Surgical management
HIV is a condition associated with low immunity; therefore, we have provided full summary of information about preoperative and postoperative care for PLWHIV in Table 1.
Summary of necessary information about preoperative and postoperative care for individuals with HIV.

ART: antiretroviral therapy. Further information can be obtained from Masoomi et al. 28
Laparoscopic appendicectomy is a preferred approach in HIV patients. 28 There is significantly higher laparotomy rate in HIV-positive patients as perforated appendicitis is more frequent in this cohort. 6 Delayed presentation in HIV-positive patients and surgery were associated with significant higher postoperative morbidity and longer hospital stays.15,28,29 Overall, HIV-positive patients have significantly higher mortality rates. 28 Patients with low CD4 count (<200) are not only likely to have complicated appendicitis but also have a significantly higher mortality rate and a trend towards a higher total postoperative complication rate.12,13,25 PLWHIV presenting with acute abdominal pain should be treated with high index of suspicion of AA.
Outcomes
The outcome of few studies demonstrates that the lack of cART may be a risk factor for AA among HIV-infected patients.9,12 Low CD4 count <200 is not a risk factor for having appendicitis, 17 in contrast to other studies. 12 PLWHIV with a history suggestive of AA should be treated differently from the general population in terms of a more cautious approach. Moreover, as morbidity and mortality can be minimized by prompt surgical intervention, 30 there is a possibility of treating conservatively in the cases with appendicitis with HIV having low CD4 counts.9,12 One important challenge for surgeons is establishing the correct diagnosis of AA and excluding conditions that mimic appendicitis. It is worth mentioning, in two case reports, abdominal mycobacterial infection can mimic AA in HIV.31,32
Limitations
One limitation of this review is that we have only included manuscripts published in English, and we have not included manuscripts written in other languages. Due to limited publications in this field, we are not able to do systematic review.
Conclusion
The prevalence of appendicitis is higher with HIV (8%) in comparison with normal population (0.1%). The HIV can be associated with different precipitating factors that can lead to appendicitis. Among these factors mentioned are the appendix is target for the virus, the chronic state of inflammation of the body, the chance for opportunistic infection to settle in the appendix and high risk associated with surgery in comparison with normal population. Further investigations and research at molecular, cellular, histological, immunological and epidemiological level are needed to understand the exact role of these factors. This will require collaborative research works among different centres in order to recruit adequate numbers of patients and this may take years to achieve. The clinical presentations are similar to normal population, but high suspicion of index is needed to diagnose appendicitis in HIV individuals. Further research is also needed to assess the benefit of using the Alvarado score in establishing the diagnosis of the AA in PLWHIV. Early diagnosis and treatment can significantly help in decreasing the complications. Figure 1 provides step-by-step guide in the management of appendicitis with HIV, and Table 1 provides summary of perioperative care. It is crucial that HIV physicians should be consulted before, during and after surgical treatment of HIV patients with appendicitis.
Footnotes
Author contributions
A.M., S.H.R., E.E., D.M. and M.H.A., all contributed equally in writing, drafting and finalizing the manuscript. A.M. and M.H.A. conceptualized the structure of the analysis paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.