
Abstract
Appendiceal neuroendocrine tumors are a rare subset of well-differentiated neuroendocrine tumors, comprising <1% of all malignancies. Appendiceal cancer is particularly rare, affecting approximately one to two individuals per one million annually in the United States. Appendiceal neuroendocrine tumors have an estimated incidence of 7/100,000 person-years in the United States. In this report, we present the case of a 19-year-old female who arrived to the emergency department with recurrent right lower quadrant pain, unresponsive to initial management for suspected acute appendicitis, and urinary tract infection. Advanced imaging revealed an appendiceal mucocele. The patient underwent appendectomy, and histopathology confirmed a well-differentiated appendiceal neuroendocrine tumor (grade 2) with lymphovascular invasion. A subsequent right hemicolectomy identified metastatic disease in 6 out of 27 lymph nodes. Unfortunately, the patient was lost to follow-up shortly after surgery. This case underscores the diagnostic complexities of appendiceal neuroendocrine tumors, which are often incidental findings during appendectomy and may present with nonspecific or atypical symptoms. It highlights the critical role of tumor size, grade, and histopathological evaluation in guiding management decisions, as well as the importance of a multidisciplinary approach to treatment. Moreover, it emphasizes the necessity of vigilant follow-up, particularly in young patients, to address the long-term implications of this rare malignancy and improve outcomes.
Introduction
Appendiceal tumors, a rare subtype of neuroendocrine tumors (NETs), account for <1% of all malignancies. 1 Approximately 60% of appendiceal NETs occur in the gastrointestinal tract, most commonly in the small intestine, followed by the rectum and appendix. 1 In the appendix, these tumors are identified in 1–2 cases/200–300 appendectomies annually, with an estimated incidence of 7/100,000 person-years in the United States.2,3
The precise pathogenesis of appendiceal NETs remains uncertain, though potential mechanisms include genetic predisposition and environmental factors. 4 Despite their rarity, these tumors present significant diagnostic and management challenges due to their variable clinical presentations and potential for metastasis. Optimal management depends on tumor size, histological grade, and metastatic involvement. Given their tendency for lymphovascular invasion and metastatic spread, a comprehensive evaluation and multidisciplinary management are crucial to optimize outcomes.
Here, we present the case of a 19-year-old female with persistent right lower quadrant (RLQ) pain, who was ultimately diagnosed with an appendiceal NET.
Case presentation
A 19-year-old female with asthma and morbid obesity presented to the emergency department (ED) with a 1-week history of right flank and RLQ pain, accompanied by increased urinary frequency. The pain, initially crampy, had intensified and radiated to the left lower quadrant. She denied fevers, nausea, vomiting, hematuria, vaginal bleeding, or changes in bowel habits. She had no prior surgeries. On arrival, her vital signs were stable, and physical examination revealed RLQ tenderness. Urinalysis suggested a urinary tract infection (UTI) caused by Proteus mirabilis, sensitive to cephalosporins. A computed tomography (CT) scan showed dilatation of the appendix tip, raising suspicion for acute tip appendicitis. Given the benign and uncomplicated nature of her symptoms, surgery was deferred, and she was discharged with a 5-day course of cefuroxime. However, the patient did not complete the prescribed antibiotic regimen.
One week later, the patient returned with worsening RLQ pain radiating to the back, nausea, dysuria, and bloody diarrhea. A repeat CT scan of the abdomen and pelvis revealed an appendiceal mucocele with luminal dilation up to 1.3 cm and mucosal hyperemia (Figure 1) but no evidence of peri-appendiceal fat, appendicolith, or peri-appendiceal fluid collection. In addition, the proximal appendix appeared normal. The small and large bowels were not dilated. A chest CT was also performed at the time and showed multiple sub-centimeter pulmonary nodules in the right and left lungs (Figure 2) without any evidence of consolidations or pulmonary edema. A laparoscopic appendectomy was performed, and the patient’s postoperative course was uneventful. Histopathological analysis confirmed a well-differentiated Grade 2 NET, with negative surgical margins (Figure 3(a)). The tumor involved the appendiceal wall and serosal surface, showing lymphovascular invasion. Immunohistochemical studies indicated neuroendocrine differentiation (Figures 3(b) and 4(a)), with a Ki-67 index of 11.2% and a mitotic rate of less than two mitoses per 2 mm2 (Figure 4(b)). Due to the tumor’s size exceeding 2 cm and the presence of lymphovascular invasion, a formal right hemicolectomy was recommended for complete lymph node dissection as per the National Comprehensive Cancer Network guidelines.
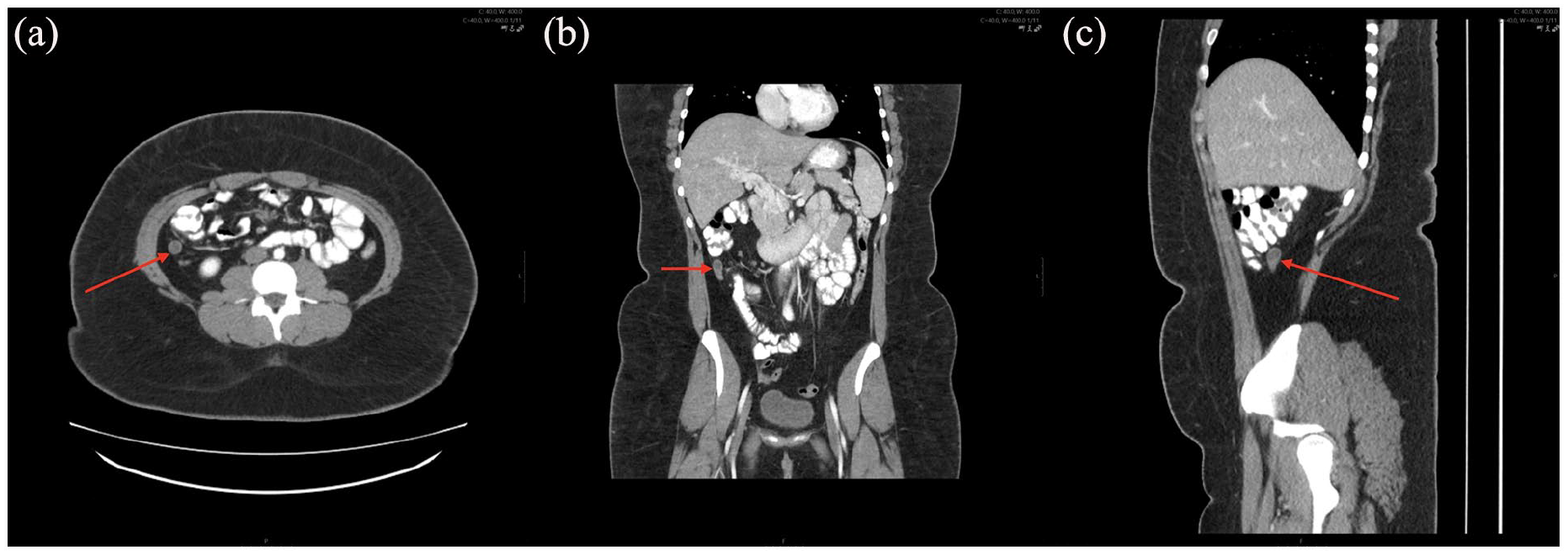
CT abdomen and pelvis showing luminal dilation of 1.3 cm of the appendix (red arrows) and mucosal hyperemia in (a) axial, (b) coronal, and (c) sagittal planes.

CT chest with red arrows showing (a) 2 mm right lower lobe nodules and (b) 4 mm nodule in the left lower lobe.

Histological characterization of biopsy. (a) Hematoxylin and eosin (20×) showing solid nests with an organoid pattern, round nuclei with salt-and-pepper chromatin, and rare nests containing small central necrosis. (b) Synaptophysin (10×) diffuse positivity of appendiceal tumor.
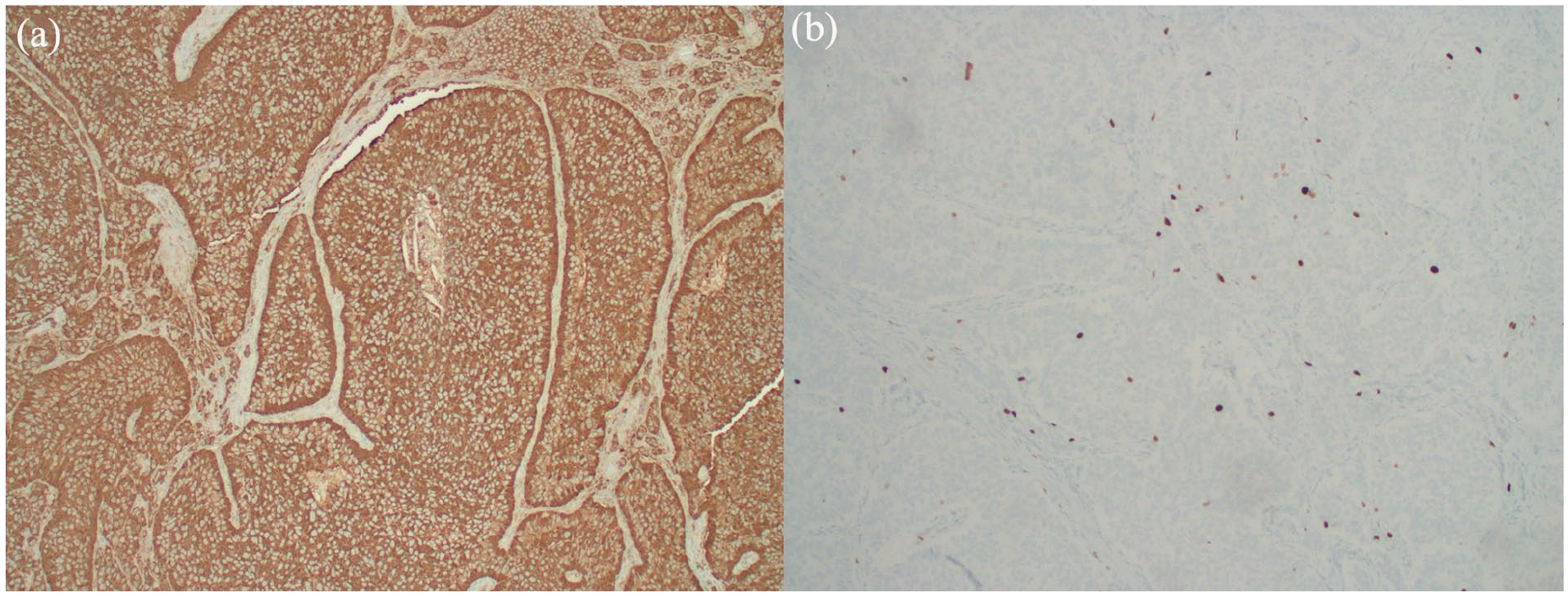
Immunohistochemical profiling of tumor. (a) Positive Chromogranin stain (20×) of appendiceal tumor. (b) Ki-67 positivity 11.2% (10×) with mitotic rate less than two mitoses per 2 mm2.
A right hemicolectomy was performed laparoscopically without any periprocedural complications 8 weeks later. The recovery was uneventful, and she was discharged on the sixth postoperative day. The final surgical pathology report of the segmental resection of the right colon revealed findings consistent with malignancy. Specifically, 6 out of 27 examined pericolonic lymph nodes were positive, consistent with a regional node metastatic well-differentiated NET. Notably, the right colon itself, including the appendectomy stump site, showed no evidence of a tumor. The proximal, distal, and radial margins were negative for tumor involvement. Additionally, the omentum was examined and found to be free of tumors. These findings suggest a case of lymph node metastasis from a primary NET, originating from the appendix.
A medical oncology consultation was scheduled as an outpatient, and the patient was recommended to undergo a follow-up CT scan in 3 months. Additionally, a NETSPOT PET scan was ordered to assess for distant metastatic disease using somatostatin receptor targeting, given the positive lymph nodes on pathology and the presence of subcentimeter, potentially metastatic, pulmonary nodules on previous CT scans. The patient was also referred to genetic counseling due to her age. Unfortunately, the patient was lost to follow-up before this could be completed.
Discussion
Appendiceal cancer is rare, affecting approximately one to two people per one million annually in the United States. 5 However, recent studies suggest an increasing prevalence, particularly among individuals between the ages of 50 and 80 years. 5 NETs are the predominant tumor type arising in the appendix, accounting for ~50% of all appendiceal cancers. 6 While NETs are most found in the small intestine, their presence in the appendix remains clinically significant, particularly when they deviate from the typical incidental discovery.2,7
In most cases, appendiceal NETs are located at the tip and are asymptomatic, often detected incidentally during appendectomies.8,9 In contrast, tumors located at the base, which occur in ~10% of cases, are more likely to present with symptoms similar to acute appendicitis. Our patient, despite the tumor’s location at the tip, presented to the ED twice with worsening RLQ abdominal pain, prompting initial consideration of both appendicitis and pyelonephritis associated with a UTI. Therefore, the symptomatic presentation despite the tumor location at the appendiceal tip caused diagnostic challenges. The most common age group affected is between 50 and 55 years with a history of smoking being a common risk factor.1,3 –5 Therefore, in a 19-year-old female with no history of smoking, this presentation is even more unusual and uncommon.
Tumor size remains the most reliable indicator for assessing both malignant potential and the likelihood of metastasis. Previous reports indicate that appendiceal NETs are typically <1 cm in size, which accounts for ~95% of cases, and are generally managed with appendectomy alone.10,11 Tumors measuring 1–2 cm require further histopathological evaluation, including assessment of mesoappendiceal involvement, to guide surgical decisions. 12 In our case, the patient’s tumor was notably large (>2 cm) and exhibited lymphovascular invasion, necessitating a right hemicolectomy. The presence of such an aggressive pathological profile in a young female, is highly unusual and warrants further discussion regarding potential genetic predispositions and tumor biology.9,13 –15 A more complete summary of prognostic factors in appendiceal NETs are found in Table 1.
Prognosis of appendiceal neuroendocrine tumors.

While the majority of appendiceal NETs are sporadic, emerging evidence suggests that genetic syndromes such as multiple endocrine neoplasia type 1, von Hippel–Lindau or neurofibromatosis type 1 may contribute to NET development.3,4 Although our patient had no known family history of endocrine or neuroendocrine malignancies, future studies should explore whether young patients with large, invasive appendiceal NETs warrant genetic screening. Additionally, recent research has identified specific molecular markers, including alterations in chromatin remodeling genes (e.g. ATRX, DAXX) and mTOR pathway dysregulation, which may influence tumor behavior and prognosis. 4 Further investigation into these associations could provide insights into risk stratification and personalized management approaches.
Such genetic and biomarker testing could have been a valuable addition in understanding the atypical presentation in this patient. Unfortunately, the patient was lost to follow-up. Even so, there does exist some prior literature on the prevalence of NETs in the pediatric population. A retrospective study by Boston et al. of 33 patients shows that appendiceal NETs were found more in female pediatric patients, generally described as low-grade, well-differentiated tumors without metastasis. 19 A 100% 5-year relapse-free survival rate was observed for patients treated for appendiceal NET in the study, further underscoring the need for intervention. 19 Another study by Wu et al. underscores the clinical significance of our patient. They report that fewer than 6% of appendiceal NETs are larger than 2 cm. Patients also present with nonspecific symptoms such as diarrhea and flushing, as in this case. 20 Therefore, our patient exhibited a larger tumor than usual coupled with lymphovascular metastasis that prompted more aggressive intervention in the form of hemicolectomy.
Follow-up recommendations also vary based on tumor size. For tumors smaller than 2 cm, excision is often sufficient without further intervention. 12 However, in cases with lymphatic metastasis, even with complete resection, long-term surveillance is advised. 4 Appendiceal NETs generally have a favorable prognosis, with an 80% 5-year survival rate, but aggressive features such as lymphovascular invasion or mesoappendiceal extension warrant closer monitoring. This case underscores the importance of conducting a thorough and patient-centered evaluation to guide clinical management.
Conclusion
This case highlights the importance of vigilant intraoperative assessment and detailed pathological evaluation in managing appendiceal NETs. Incidental findings during surgery may warrant further surgical intervention based on tumor characteristics. Given the potential for nonspecific presentations, particularly in younger patients, careful consideration of the risks and benefits of additional intervention is essential to minimize morbidity and improve patient outcomes.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Consent to participate was obtained from the patient.
Consent for Publication
Informed written consent was obtained from the patient for their anonymized information to be published in this article.
Author Contributions
Fariha Hasan: conceptualization; writing – review and editing. Amir Davoodi: investigation; writing – original draft; writing – review and editing. Amy Bordogna: investigation; writing – review and editing. Shrey Dalwadi: investigation; writing – review and editing. Yumna Timsaal: investigation; writing – review and editing. Avneet Singh: conceptualization; writing – review and editing. Alexander Garcia: investigation; writing – review and editing. Kim HooKim: investigation; supervision; writing – review and editing. Satyajeet Roy: investigation; writing – review and editing; supervision.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.