
Abstract
The fat embolism syndrome is a well-known complication in trauma patients. We describe a rare case of traumatic fat embolism that leads to paraplegia. A 19-year-old male motorcycle accident victim was presented to our hospital. After stabilization and trauma survey, he was diagnosed with bilateral femur fractures, a spleen laceration and a tear in the inferior vena cava, for which damage control surgery was performed. Post-operatively, the patient became paraplegic and developed a fluctuating consciousness, respiratory distress and petechiae. Fat embolism syndrome was considered as the most plausible cause of the paraplegia. The fat embolism syndrome is seen in approximately 1% of trauma patients, mostly those with bilateral fractures of the femur. Prevention of the syndrome depends on early stabilization of fractures. However, even with optimal care, this syndrome can still occur and may have dramatic consequences, as we demonstrate in this case.
Introduction
The fat embolism syndrome (FES) is a well-known complication that could result from trauma and many diseases. The defining triad consists of respiratory distress, neurological deterioration and skin rash and could in severe cases lead to death. 1 We describe a case of trauma-induced FES leading to lasting paraplegia and provide an overview of the literature.
Case
A 19-year-old Dutch male sustained a high-speed motorcycle accident. The patient was stabilized on site, placed on a cervical protection device and due to a decreased Glasgow Coma Scale (GCS) score intubated. Before sedation, he had moved all four limbs. Initial assessment in our emergency room revealed normal breathing sounds bilaterally and a saturation of 100% with 10 L of O2. He had a pulse of 102 beats/min and a blood pressure of 85/50 mmHg (mean arterial pressure of 62 mmHg). Midshaft bilateral femur fractures were evident. Neurological examination was not performed because of sedation.
Chest, pelvic and cervical spine x-ray showed no fractures. Ultrasound assessment (FAST) showed a spleen laceration without intra-abdominal free fluid. A total body computed tomography (CT) scan with intravenous contrast showed contrast extravasation in the left iliac region, a retroperitoneal haematoma and a spleen laceration grade IV. No intracranial bleeding or fractures of the cranium or vertebrae were seen.
Laboratory results showed haemoglobin of 4.3 mmol/L, thrombocytes of 175 × 109/L and a prolonged activated partial thromboplastin time (APTT) of 45 s.
Emergency laparotomy followed and a splenectomy was performed. A tear in the inferior vena cava was identified and sutured. Both femur fractures were stabilized with external fixation. The total operation time was 3 h and 30 min. Post-operatively, our patient was transferred to the intensive care unit.
Over the entire course, a state of permissive hypotension was successfully maintained and the patient remained haemodynamically stable. To achieve this, a mass transfusion with 32 U of blood products and 12 U of solution was administered during assessment, surgery and recovery.
Twenty-four hours after surgery, sedation was ceased and neurological examination performed. The patient had a GCS of E4M6Vtube and paraplegia with complete loss of motor and sensory function from Th9 on the left side and Th10 on the right side of the body. A second CT scan did not reveal the cause for the paraplegia.
Several hours after neurological examination, the patient’s consciousness deteriorated and oxygenation levels declined. The GCS varied from E1M1Vtube to E3M3Vtube. Positive expiratory pressure had to be raised from 5 to 10 cm H2O. Diffuse swelling of the brain was seen on repeated CT scan.
The second day after trauma, conjunctival and skin petechiae were visible. Because of fluctuations in the GCS, respiratory deterioration and petechiae in a trauma patient with bilateral femur fractures, FES was suspected. A magnetic resonance imaging (MRI) scan of the brain revealed, besides diffuse swelling, multiple punctiform T2 hyperintense lesions diffusely spread in the brain in a pattern that is characteristic for FES (Figure 1). An MRI of the spinal cord showed an extensive ischaemic lesion from Th8 to the conus medullaris (Figure 2). The lesion was the result of embolism; however, the image itself cannot differentiate between causes of embolism. It does rule out hypotension as a cause for ischaemia. Supportive care was continued, and after 4 days, our patient had a maximal GCS and mechanical ventilation was ceased.

MRI of the patient 1 day after onset of neurological symptoms. On the left side, a T2-weighted image with multiple foci of high signal intensity bilaterally in the semioval centre (arrows) in keeping with the starfield pattern described for FES. On the right side, corresponding diffusion-weighted image showing diffusion restriction as a result of fat emboli.
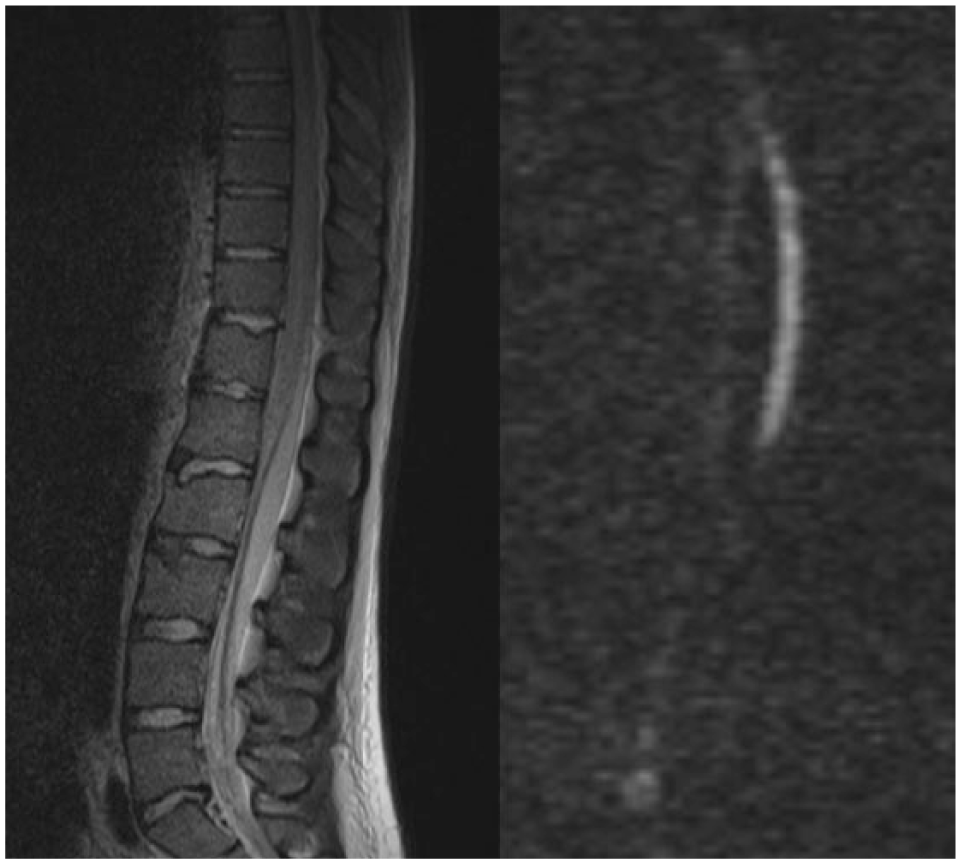
MRI of the thoracolumbar spine of the patient 1 day after onset of the paraplegia. On the left side, a sagittal STIR-weighted image showing a hyperintense signal in the distal part of the myelum which appears swollen. On the right side, a diffusion-weighted image with diffusion restriction of the corresponding myelum consistent with extensive ischaemia due to embolism. In this image, the cause of the embolism cannot be identified.
Both femur fractures were successfully treated with the external fixation, and no further complications occurred. Cognitive functions recovered fully, but the paraplegia with complete loss of motor and sensory function remains to this day.
Discussion
The FES was first described in 1862. 2 Today, the established triad of symptoms caused by diffuse embolism with fat globuli consists of respiratory distress, cerebral impairment and skin rash. 1
The exact pathophysiology of traumatic FES remains unknown, but two theories exist. The mechanical theory states that fat and bone marrow enter the bloodstream directly into the venous system at the site of the fracture. These particles then pass towards the pulmonary circulation and cause embolization and subsequently respiratory distress. Furthermore, small fat globules are believed to be able to pass through the pulmonary circulation or a persisting foramen ovale and enter the systemic circulation, causing embolism in the brain, skin and other parts of the body.
However, this mechanism does not explain the late onset of symptoms after trauma and not every patient with FES has a persisting foramen ovale. In this case, the patient had no persisting foramen ovale. In turn, the biochemical theory suggests that circulating bone marrow due to trauma causes an inflammatory response, which results in damage to capillary beds and leads to embolisms throughout the entire body. 3
FES usually develops 24 up to 72 h after trauma. 4 The most common feature is pulmonary distress which occurs in up to 96% of the cases, of which 44% require mechanical ventilation. 5 Second, cerebral embolism could occur and may result in a confusional state, a lowered mental status, seizures and in some severe cases coma. These symptoms usually resolve over time. 6 The incidence of cerebral involvement is reported in up to 59% of patients who suffer from FES. 7 Petechial rash, seen in up to 60% of the cases, usually occurs within the first 36 h and can affect any part of the skin, conjunctiva or mucous membrane. 8
Spinal cord ischaemia due to FES, as seen in our case, has only rarely been reported. One other reported case describes a 22-year-old male with a B-cell lymphoma which induces FES and subsequently a conus medullaris syndrome. 9 Neurologically, he recovered fully. A second case describes a 22-year-old male involved in a traffic accident with multiple fractures, including bilateral femur fractures. This patient develops spinal cord infarction at cervical level following fixation of the femur fractures with the use of retrograde reamed nailing. 10 In this case, the infarction is also transient and the patient recovers fully. Both cases describe the development of spinal cord infarction due to FES and full recovery from the infarction. This is in contrast to our case where the paraplegia remains. This gives rise to the question whether the spinal cord infarction is caused solely by FES. However, there was no direct trauma to the spinal cord and during first response resuscitation was swiftly started. A state of permission hypotension was successfully maintained during the prehospital and hospital phase. In general, permissive hypotension appears to result in fewer complications compared to a more aggressive resuscitation approach and yields no added risk for embolism or infarction of any kind. 11 Despite massive blood loss due to the spleen and vascular injury, the mean arterial pressure was above 60 mmHg during the entire course. This dismisses the likelihood of hypotension as a cause for the paraplegia in this case.
In 1974, Gurd and Wilson 1 developed a scoring system that describes major and minor diagnostic criteria (Table 1). It is still the main tool used to diagnose FES and relies mostly on clinical presentation and symptoms. In the decades following the Gurd et al. scoring system, new diagnostic instruments were developed that are useful in identifying FES and can potentially predict its severity and outcome.
Gurd and Wilson scoring system for the fat emboli syndrome.

The criteria are met when a patient has one major and four minor criteria.
Today, MRI is a very useful tool for diagnosing cerebral FES. 12 It can also differentiate between different stages and extend of the syndrome and differentiate between FES and diffuse axional injury.13,14
In addition to radiological findings, there is an increased interest in inflammatory markers in FES. Among others, interleukin-6 level at 12 h after trauma seems to have a predictive value for developing FES. 15
Following the Gurd et al. scoring system, our patient met all three major and two minor criteria. Moreover, the very characteristic so-called starfield pattern in the brain was seen on MRI T2-weighted images with corresponding diffusion restriction (Figure 1, left side). This occurs in 96% of the patients suffering from cerebral fat embolism.6,16
Although potentially fatal in severe cases, with a reported mortality of up to 7%, FES is usually self-limiting. 7 Optimization of the pre-hospital phase, timing of treatment during initial care and better post-operative supportive care have led to a decrease in incidence of the FES. Besides early fixation of long bone fractures, treatment options remain limited.17,18
Since the pathophysiology remains unclear and recent insights have not resulted in treatment options, we advocate more research and a new approach in diagnosing and classifying FES. Hopefully, this will result in a better understanding of this syndrome and the first effective therapeutic option.
Conclusion
The FES can have many different clinical courses and holds diagnostic difficulties. Incorporating current radiological and laboratory options in a scoring system could improve diagnosis and prediction of severity. Despite damage control surgery and rapid stabilization of long bone fractures, FES can still occur, and unfortunately, definitive treatment is not yet available. As our case demonstrates, spinal cord ischaemia with permanent paraplegia is a very rare, but possible and devastating outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.