
Abstract
Purpose:
There is an increasing focus on racial and social disparities in health care. There have been several studies that have documented disparities in outcome between racial groups in the adult literature. Not much is known about disparities in outcomes after surgical procedures in children. The purpose of this study was to investigate the effect of race on complications (outcomes) and costs after laparoscopic appendectomy.
Methods:
This study is a single-center retrospective chart review of 248 pediatric patients who underwent appendectomies for uncomplicated acute appendicitis from 2015 to 2017. Patients were divided into minority (Africa American or Hispanic) and non-minority groups, and length of stay, preoperative and postoperative factors, and total costs were compared.
Results:
Of 185 eligible patients, 45.9% (n = 85) were of Hispanic or African American ethnicity and 54.1% (n = 100) were Caucasian. About 11.8% of minority patients had comorbidities and 12% of majority patients had comorbidities (p = 1). Readmission rate for minority group patients was 3.5% (n = 3) and 2% (n = 2) for majority patients (p = 0.7). The average cost of hospital stay for minority patients was $30,900 and for majority patients was $31,111 (p = 0.59).
Conclusions:
Standardization of care protocols has reduced social/racial disparities in surgical outcomes. In the most common pediatric surgery emergency procedure, laparoscopic appendectomy, there were no differences in outcomes or costs between minority (Hispanic/Africa American) and Caucasian ethnic groups.
Level of evidence:
Level III
Type of study:
Clinical Study
Introduction
Appendicitis in children is a common surgical problem that adds to billions of dollars in health care costs every year. 1 There is literature to suggest that race and socioeconomic factors play a role in surgical management decisions. There is evidence that Caucasians are more likely to have their appendicitis treated by minimally invasive techniques as compared with African Americans.2,3 However, there is limited literature of race and length of hospital stay after surgery for pediatric appendicitis and associated costs.4–6 The purpose of this study was to investigate the effect of race on hospital costs and length of stay after laparoscopic appendectomy for non-complicated acute appendicitis, the most common emergent surgical procedure performed in children.
Patients and methods
IRB approval was obtained prior to performing single-center retrospective chart review of pediatric patients (<18 years old) who underwent appendectomies for acute appendicitis from January 2015 to April 2017. These patients were found under International Classification of Diseases (ICD)-9 and ICD-10 codes for acute appendicitis. All patients underwent a standardized emergency department (ED) evaluation, imaging protocol, and post-operative care plan when presenting to the facility with non-complicated acute appendicitis. Exclusion criteria included perforated appendicitis, non-operative management, interval appendectomies, or other diagnoses at surgery. Of the 248 total patients found through chart review, 63 were excluded. The remaining 185 patients were divided into two groups: minority (African-American or Hispanic) and non-minority groups.
We utilize a three-port technique for laparoscopic appendectomy, and the technique has been described elsewhere. 7 The patients were cared for in a nationally accredited children’s hospital. Patients were admitted and entered into a queue of patients waiting for emergency surgery, prioritization depending on physiological parameters and age.
Length of hospital stay, preoperative and postoperative factors, and total costs were compared and analyzed between the two groups. The findings represent a follow-up, focusing on racial disparities in health care delivery, to our previous publication on the topic of same-day discharge (SDD) after laparoscopic appendectomy. 8
Statistical calculations were performed using the Fisher exact test for categorical data and unpaired student t-test for continuous variables. A power calculation suggested that 200 patients would be needed in each arm to detect a 10% difference in outcomes accepting an Alpha error of p < 0.05 (Power = 0.8). A p-value of 0.05 or less was considered to be statistically significant.
Results
Of the 185 patients, 85 (45.9%) were of minority ethnicity (Africa American or Hispanic) and 100 (54.1%) were of majority ethnicity (Caucasian). Table 1 illustrates the demographic characteristics of the two groups.
Demographic characteristics of minority and majority group patients.

SDD: same-day discharge, BMI: body mass index, CI: confidence interval.
Pre-operative factors
The average age was 10.8 years for the minority group 1 and 11.9 years for the Caucasian group (p = 0.04). Patients tended to be male in both ethnic groups; 58.8% (n = 50) of minority group patients and 57% (n = 57) of majority group. The percentages of obese patients (body mass index greater or equal to 30) within the minority and majority groups were 5.9% and 6%, respectively (p = 1). All patients were covered by some form of health insurance, either Medicaid or private insurance. About 68.2% (n = 58) of minority patients had Medicaid health insurance while 31.8% (n = 27) had private insurance. About 8% (n = 8) of majority patients were covered by Medicaid health insurance and 92% (n = 92) were covered by private insurance (p < 0.001) (Table 1).
Table 1 illustrates the preoperative history, clinical presentation, comorbidities, and laboratory values in the two groups. An imaging study (either ultrasound or computed tomography scan) was performed in 74.1% of patients in minority group as compared with 77% of patients in Caucasian group (p = 0.86). In the minority group of patients who had one study performed, 60.3% (n = 38) had an ultrasound and 39.7% (n = 25) had a CT scan. By comparison, 87% (n = 67) of the patients in the Caucasian group with one study had an ultrasound and only 13% (n = 13) had a CT scan (p < 0.001) (Table 2).
Clinical features of patients in the majority and minority groups.

ADHD: attention deficit hyperactivity disorder; DM1: diabetes mellitus type 1; GERD: gastroesophageal reflux disease; IBS: inflammatory bowel syndrome; Family History: family history of appendicitis; LOS: length of stay; ED: emergency department arrival; CS: surgical consult; OR: operating room. CI: confidence interval; SDD = same-day discharge.
Fever: T > 100.4°F.
Hospital admission and length of stay (LOS)
The difference in average amount of time from presentation to the ED and time of surgical consult for minority and Caucasian groups was 5.1 and 5.5 hours, respectively (p = 0.49). The time to surgery after initial evaluation in the two groups is depicted in Figure 1(a) and (b). In the minority group, 48.2% (n = 41) were SDD, whereas in the Caucasian group 69% (n = 69) were SDD (p = 0.005). The average LOS was 26.5 hours for minority group and 23 hours in the Caucasian group (p < 0.001). Average postoperative LOS in the minority and Caucasian groups were 17.5 hours (median = 16.6; range = 0.8–124 hours) and 16.6 hours (median = 14.5; range = 0.7–97 hours), respectively (p = 0.7).
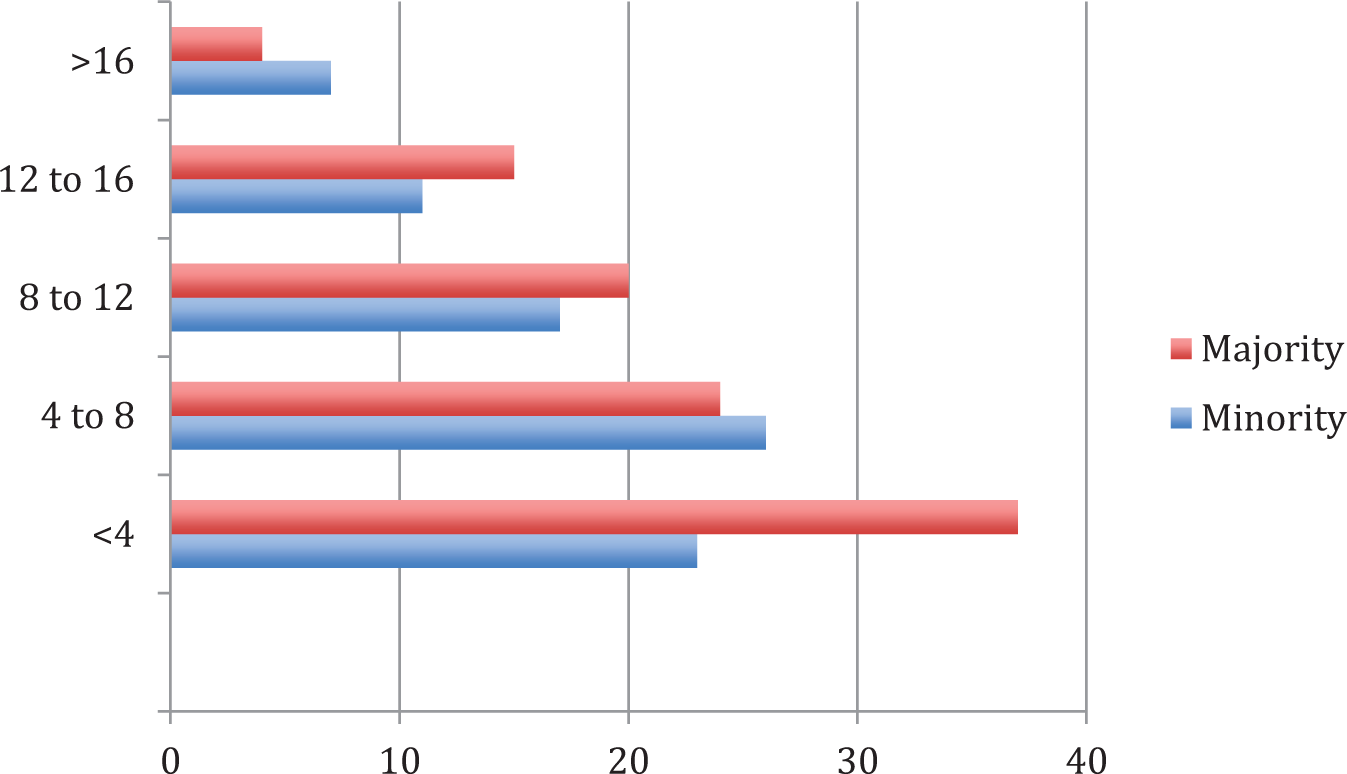
Time in hours to consultation in the majority and minority groups.
Postoperative factors
There was no significant difference in perioperative complication rate in between the two groups with one patient in the Caucasian group developing rhabdomyolyis (0% vs 1%; p = 1). In the minority group, three patients (3.5%) presented to the ED after their surgery without needing readmission, while 1 patient in the Caucasian group (1%) had an ED revisit (p = 0.34). Readmission rate in the minority group was 3.5% (n = 3) and 2% (n = 2) among Caucasian patients (p = 0.7) (Table 2). The three readmissions in the minority group were for antibiotic induced colitis, abdominal pain, and right lower quadrant abscess, respectively. In the Caucasian group, two patients needed readmission for intra-abdominal abscess.
Costs
The average cost of hospital stay is illustrated in Table 2. In the minority group, average cost for admission and treatment was $30,900 and for Caucasian group was $31,111 (p = 0.59). Within the minority group, SDD had average cost of $28,100 and non-SDD had average cost of $33,500 (p < 0.01). In the Caucasian group, average costs in the two categories were $29,800 and $34,000, respectively (p = 0.07) (Table 2).
Discussion
Children in minority groups have been observed to have worse outcomes and prognosis across various medical specialties, including surgery. 9 Other reports have found that African-American and Hispanic present with perforated appendicitis more often than their Caucasian counterparts and were more likely to have complications and increased hospital stay. 10 We have tried to remove any disparity in the comparison groups in our simple study to truly study the effect of race on outcome by only including non-complicated appendicitis managed by laparoscopic appendectomy. In our study, neither the outcomes nor the charges (costs) were different between majority and minority groups. Furthermore, both minority and majority group patients present similarly with little difference in their disease process. This is important, as pediatric appendicitis is the most common emergency operation performed in children. Our results show that racial disparities do not extend to outcomes in pediatric appendicitis, a commonly performed pediatric emergency procedure. The reasons for the study results could be attributed to the urban setting; tertiary care hospital services in a National Association of Children’s Hospitals and Related Institutions (NACHRI) approved children’s facility, standardization of care protocols, teaching facility, and board certification in pediatric surgery among operating surgeons. It will be important to further validate the findings of this study using larger national inpatient databases.
There were some differences in care that were noted, and it is important that quality metrics and studies on disparity address all aspects of the care process. Patients who received only one imaging study were more likely to receive a CT scan if they were in the minority group and an ultrasound if they were in the Caucasian group. With an active discussion among stakeholders to reduce exposure to ionizing radiation, it is troubling that children still are exposed to a greater amount of CT scan imaging without a prior ultrasound despite having an active protocol. Potential reasons for this finding include communication barriers, diagnostic difficulty, and examination findings more suggestive of complicated appendicitis or other abdominal pathology. Greater awareness among the Caucasian group parents may also have led to them declining CT scans in their wards due to the perceived harm of ionizing radiation.
All patients were covered by health insurance, either through Medicaid or private insurance. There were significantly more patients with government Medicaid than private insurance in the minority group as compared with the Caucasian group. Patients in both minority and majority groups did not have significant differences in postoperative complications or ED revisits and readmissions. Having standardized protocols reduces variability in care delivery. Setting expectations in the peri-operative setting is imperative in achieving these outcomes. Even for non-perforated appendicitis, a few studies have found that minorities are more likely to be non-SDD compared with majority population groups. 11 We also noted a higher rate of non-SDD in minority patients; however, this did not impact cost or quality. The differences noted in the rate of SDD suggest that we still have some work to do but most importantly neither the costs nor the results are impacted by the slight increase in length of stay.
From the hospital’s perspective, taking care of a large proportion of Medicaid children impacts the bottom line. In this study, there were a higher proportion of minority (predominantly Medicaid) patients who did not have SDD. While the costs averaged out across the minority group, and there was no significant difference between groups, it is possible that larger studies may find this to significantly impact the bottom line of institutions that predominantly care for minority/Medicaid patients. While the costs to the hospital system are the same irrespective of the insurance status of the infant, the profit margins are better with commercial insurances. Designated children’s hospitals often see transfers of patients who are in their late teen years and many of these transferees are Medicaid recipients. It is important for the State and Federal agencies to acknowledge these financial implications and consider different level of reimbursement for designated children’s facilities to ensure their profitability.
Care for appendicitis is driven by standardized protocols in our institution and reflects the reduction in variability in health care overall. The lack of a significant difference in hospital charges and minimal difference in length of stay between Caucasian and minority groups is a testament to this standardization process of health care. This study has inherent limitations, as it is a retrospective study at a single-center and lacks statistical power. Thus, the findings may be limited in application to a larger population. A number of patients were admitted after being transferred from outside hospitals, which may have delayed diagnosis or surgery and affected presenting symptoms and laboratory findings. Further study with greater attention to patient social, educational, and economic factors in larger databases might improve our understanding of racial differences in surgical outcomes.
Conclusion
The lack of disparity in outcomes and costs among ethnic groups in pediatric appendicitis, one of the most common pediatric pathologies, suggests that the health care system is doing its job in providing equitable health care to all stakeholders. It is important for Medicaid reimbursements to keep pace with costs of inflation and new technology so that these gains in equitable patient care are not lost.
Footnotes
Acknowledgements
Dr. Olivia Cheng, MD, helped with data collection and analysis.
Author contribution
Dr. Burjonrappa: data curation; formal analysis; conceptualization; methodology; writing—draft, review, & editing.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from NYU Winthrop University Hospital Institutional Review Board (#17424 approved on 4/28/2017).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Institution Review Board approval was obtained from NYU Winthrop IRB. Informed consent was not sought for the present study because IRB Winthrop retrospective study with HIPAA protection/ no risk to human subjects/ no direct patient contact and thus meeting informed consent EXEMPT criteria.