
Abstract
Objectives:
The relationship between poverty and health has been well addressed in public health research. The health effects of social and economic inequalities on working groups have also drawn the attention of occupational health scholars. Research addressing workers in low-paying jobs showed increased risks for poor health. This research examined the psychosocial factors associated with poor mental health and self-rated health among low-income bakery workers performing demanding tasks.
Methods:
Face-to-face interviews in 504 randomly selected bakeries in Lebanon provided data on socio-demographics, perception of the workplace environment, job security, job satisfaction, general health, and mental health.
Results:
In total, 16.5% of bakery workers reported poor self-rated health, and 45% reported poor mental health. Workers with a chronic illness were almost three times more likely to report poor self-rated health (OR = 2.86; 95% CI = 1.44–5.67), and those with musculoskeletal pain reported poor self-rated health five times as often (OR = 5.34; 95% CI = 2.9–9.80). Those with a chronic illness and musculoskeletal pain were twice as likely to report poor mental health (OR = 1.94; 95% CI = 1.07–3.50 and OR = 2.07; 95% CI = 1.32–3.23, respectively); and those dissatisfied with their job reported poorer self-rated health (OR = 2.18; 95% CI = 1.12–4.23) and mental health (OR = 2.57; 95% CI = 1.54–4.26). In addition, workers reporting job insecurity had poor mental health twice as often (OR = 1.93; 95% CI = 1.24–2.99). Low socioeconomic indicators showed a gradient association with both poor self-rated health and mental health.
Conclusion:
Reporting job dissatisfaction and insecurity, musculoskeletal pain, and chronic illness were associated with poor mental and self-rated health among bakery workers. Interventions to improve the working conditions of bakery workers are timely and essential. This research provided evidence for policy to guide occupational health practice and safeguard the health of bakery workers.
Keywords
Introduction
Health research has become increasingly concerned with the relationship between poverty and health.1,2 Studying the health of workers in low-paying, highly demanding occupations offers empirical data to examine and understand the effects of social and economic inequalities on people. This study focused on the health of Lebanese bakery workers, most of whom are low-paid and experience job insecurity.
Bakeries are a ubiquitous feature of Lebanese street and food culture. They are integral to the local food economy, providing fresh pastries and bread that are a daily staple of Lebanese cuisine. 3 While bakeries have an important societal value, most owners and workers within small-scale bakeries are low-wage and at or near the poverty line. With limited resources, bakeries may have difficulty investing in the infrastructure and resources necessary to ensure a safe and healthy work environment. Furthermore, limited government capacity to engage in inspections and oversight of occupational health and safety conditions are impediments to industry-wide changes.
Most studies on the health of bakery workers have focused on industrial bakeries in developed countries, with a major emphasis on the respiratory effects of flour dust4–6 or the allergies and skin problems it produces. 7 This literature has not filled the gaps in knowledge about the occupational health of bakery workers in low-middle income countries like those found in Lebanon.
Unlike comparable businesses in developed economies, small-scale Lebanese bakeries lack adequate ventilation and air conditioning, among other basic occupational safeguards. Workers in these bakeries spend long hours in cramped, hot work environments for shifts that can extend beyond 12 hours a day. These workers perform many tasks, such as dough handling, repetitive hand movements, heavy lifting, and working next to hot ovens, which may lead to health problems ranging from musculoskeletal pain to burns and heat-related illnesses. 8
The literature has described musculoskeletal pain as endemic in many low-wage occupational groups, including industrial workers, food and meat processors, clerks, data processors, and bakery workers.9,10 Occupational factors that are common among bakery work—a rapid work pace, heavy physical workload, repeated and forceful manual exertions, prolonged periods of awkward postures, and whole-body vibration—have been correlated with increased musculoskeletal pain.11,12 Our previous research has identified a positive correlation between somatization and reporting of upper musculoskeletal pain. 8 In addition, a study of bakery workers in Arak, Iran, found that this was the case among the study population, with over 40% of respondents engaging in harmful postures during their work tasks, and more than 60% had musculoskeletal pain. 13 Similarly, a study of a Nigerian bakery industry found that musculoskeletal problems were prevalent among 72% of bakery workers. 14 Furthermore, workers in traditional bakery industries may not receive the necessary occupational health and safety information to safeguard health, 15 while another study found that the use of personal protective equipment reduced symptoms of asthma and skin rashes. 16
In addition to being exposed to hard physical labour, bakery workers are regularly exposed to extreme heat. 17 Exposures to extreme heat conditions are linked to a range of illnesses and injuries – heat exhaustion, heatstroke, heart or lung disease, accidents, and injuries – and may even lead to death.18,19 Temperatures and humidity in indoor work environments may increase during hot and humid seasons, 20 especially in workplaces that lack effective ventilation or air conditioning – like in many Lebanese bakeries. These hot environments are related to chronic venous diseases among bakery workers. 21 Another aspect of high-paced food and service work, such as bakery work, is psychologically stressful working and employment conditions. Psychological distress has been linked to musculoskeletal pain, increasing severity of pain, and multi-site pain.12,22,23 Psychosocial factors such as job satisfaction, job content, organizational problems, decision latitude, and social support may also lead to increased musculoskeletal pain.12,22–25 In a study of data from a biannual US national survey, Waters et al. (2007) found that workers who were not satisfied with their jobs and who reported their work as always stressful were more likely to report back pains (OR = 7.65, 95% CI = 1.59–45.0 and OR = 2.89, 95% CI = 1.59–5.24, respectively). 26
Mental health and self-rated health (SRH) have been previously linked to poverty, low social status, and poor workplace conditions.22,27,28 Mental health has been linked with individual health ratings. Studies have found that workers reporting chronic illness were more likely to report poor SRH and mental health. 29 Other studies suggest that poor mental health among workers is an important risk factor for physical illness, 30 work-related injuries, 31 and absenteeism. 32 An Australian study found an 18% increase in absenteeism rates among manual workers reporting high psychological distress. 32 Psychological distress has economic implications for the bakery industry, affecting operational expenses and workers’ income and savings.
SRH has been widely used by public health professionals as a measure of health status, morbidity, and mortality.33,34 Researchers have observed associations between health ratings and a variety of individual indicators, including age, employment status, access to social support, and health history and status.35–37 Poor SRH among bakery workers may reflect poor health, life dissatisfaction or unhappiness, and psychological distress.
Although bakery workers in low-middle income countries are generally a vulnerable population facing hazardous occupational settings, a few studies assessed their health. In fact, this occupational group has not been studied in Lebanon and the Arab region. Our research aimed to address this gap by studying the health of low-wage bakery workers in Lebanon and exploring the links between SRH, mental health, and workplace psychosocial factors.
Methods
This study utilized a cross-sectional survey of a representative sample of bakery workers in Lebanon.
Study population and sampling strategy
A list of bakeries was obtained from a GIS company in Lebanon. This list included a total of 1960 bakeries distributed throughout 5 Lebanese governorates: North, Mount Lebanon, Beirut, South, and Nabatieh. A number of bakeries proportionate to the density of bakeries in each region were sampled, whereby the number of bakeries selected from each governorate was derived from the proportion of the total number of bakeries in that governorate as compared with the total number of bakeries in the country, yielding a final sample of 582 bakeries. Of these, 504 bakeries were successfully reached, with one worker interviewed from each bakery (87% response rate). Any worker male or female performing bakery tasks and who was identified at any of the 504 randomly selected bakeries was eligible for inclusion in the study, regardless of the age group. During data collection, 78 bakeries were not found, were closed, or refused to participate for reasons of lack of time or mistrust.
Study protocol
A face-to-face interview, lasting between 40 and 50 min was carried out with each of the 504 bakery workers at the workplace after securing written consent from both employers and workers. The survey instrument (see Supplemental Material), which had been pilot-tested before conducting the interviews, included items on mental health, chronic illnesses, musculoskeletal symptoms, psychosocial aspects of work, as well as socio-demographic variables. The study was approved by the Institutional Review Board (IRB) at the American University of Beirut (no. FHS-RH1.03). This national umbrella project on bakery workers has also been described elsewhere. 8
Study variables
In this study, the independent socio-demographic variables included age, gender, and education. Age was split into two categories (⩽40 and >40 years) to test associations. Three levels of education were identified, being ‘secondary level or university’, ‘intermediate level’, and ‘primary level or below’.
In addition, psychosocial indicators were captured by measures of the socioeconomic status and the social environment at work. Workplace psychosocial indicators assessed whether workers were satisfied with their current job or not (dichotomized as satisfied or dissatisfied), whether they felt secure in their jobs, that is, whether their position would remain if they took a 3-month leave of absence due to illness (dichotomized as secure and insecure). Questions also addressed whether they worked under pressure, whether they get support from colleagues, the number of years working in their current job (⩾5 years or <5 years), their perception of their economic status, and their monthly income. Workers were also asked about their perceptions of the effect of workplace temperatures on their health.
The mental health and SRH of bakery workers were used as the primary health measures, as described in detail below. Mental health was measured using the Arabic version of the five-item Mental Health Inventory (MHI-5), a scale that was developed for use in the general population38,39 and which has been validated and applied in Arabic.40–43 The five items include questions about feelings of nervousness, tiredness, calmness, depression, and unhappiness in the 4 weeks prior to the interview. Scoring of MHI-5 ranges between 5 and 25. 44 For analysis, a cut-off point of less than 19, consistent with previous studies, was used as an indicator of poor mental health. 44
SRH was assessed by asking the respondent, ‘How do you perceive your current health status?’ The answer options were ‘very good’, ‘good’, ‘fair’, ‘bad’, or ‘very bad’ 33 which were then combined into two categories, ‘poor’ (including very poor, poor, and fair) and ‘good’ (including very good and good). Participants were also asked about having any chronic illnesses, which were self-reported and openly coded.
In addition, musculoskeletal pain was measured using a modified Nordic musculoskeletal questionnaire assessing pain prevalence during a 12-month period at six body regions (low back, neck, shoulders, elbows, wrists, and knees). 45 Workers were classified as having musculoskeletal pain at any of the six body sites or not having any musculoskeletal pain at all.
Statistical analysis
Descriptive analyses using frequencies and percentages were carried out for the study sample. Univariate and bivariate analyses were then done to examine the associations between SRH and mental health with the independent variables. Subsequently, two logistic regression models (one for SRH and another for mental health) were fitted with the independent variables that were significant at the bivariate level (p < 0.05). The same independent variables were used in both models. We explored analysing males and females in separate models (tables not shown); however, due to the small number of females in the sample (n = 70), there were no significant findings that could be inferred.
Adjusted odds ratio (OR), 95% confidence interval (CI), and p-values were reported. Data analysis was carried out using SPSS 20.0. The goodness of fit of the models was assessed using the Hosmer–Lemeshow test, indicating no lack of fit. We tested for first-term interactions, including the main effect, and no significant terms were found.
In addition, both SRH and mental health were grouped into three categories to test their association with the social environment at work, economic status, and physical health. The three categories were as follows: ‘none: for neither poor mental health nor poor self-rated health’, ‘1: for either poor mental health or poor self-rated health’, and ‘2: for both poor mental health and poor self-rated health’.
Results
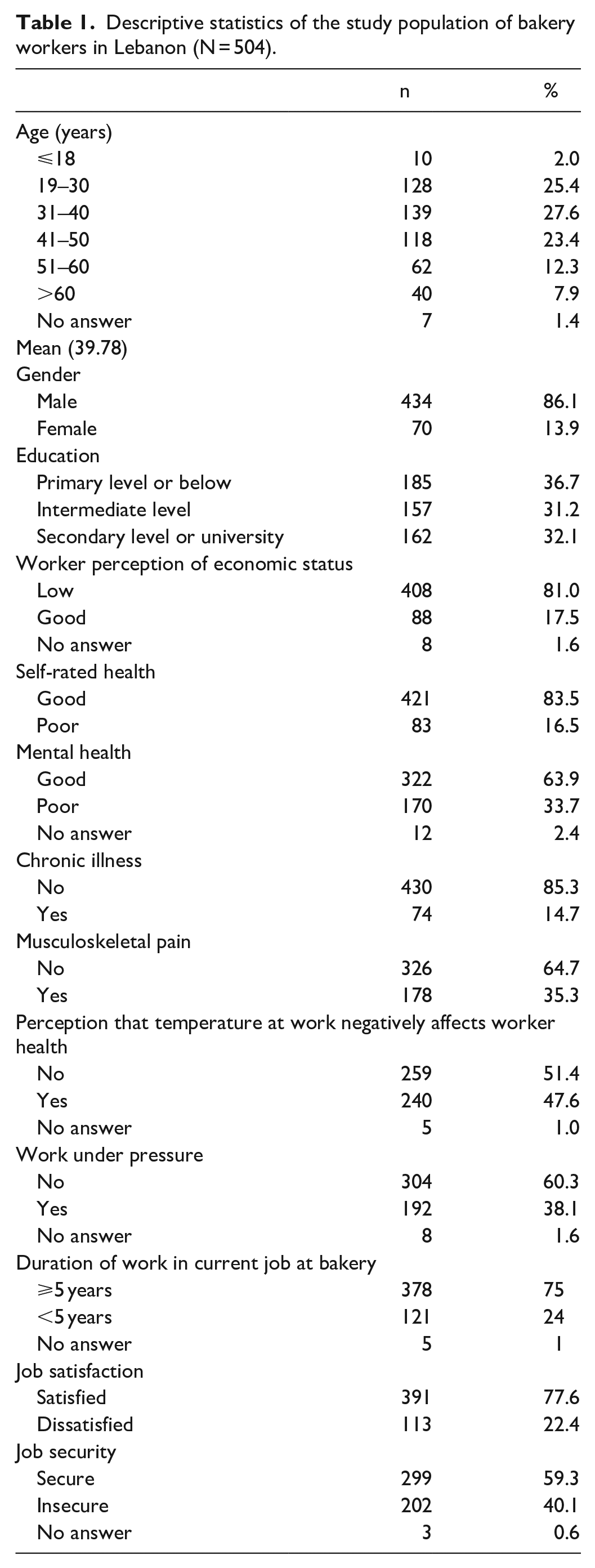
Out of 504 bakery workers, 16.5% self-reported poor health (Table 1), and 45% reported poor mental health. Socioeconomic information of the sample shows that the vast majority of workers were men (86%) and almost half were older than 40 (44%). Only 32% had remained in school beyond the intermediate level, while 81% viewed their economic status as bad. In terms of workers’ physical health, only 15% reported suffering from a chronic illness and 35% reported musculoskeletal pain. Forty percent of the workers described their employment as insecure, 38% worked under pressure, and 75% reported working at their current job for 5 or more years, averaging 66 h of work each week.
Descriptive statistics of the study population of bakery workers in Lebanon (N = 504).
Findings of the logistic regression models show that psychosocial factors were significantly associated with poor SRH and with poor mental health (Table 2).
Association of psychosocial workplace factors with poor self-rated health and poor mental health among bakery workers in Lebanon (N = 504).
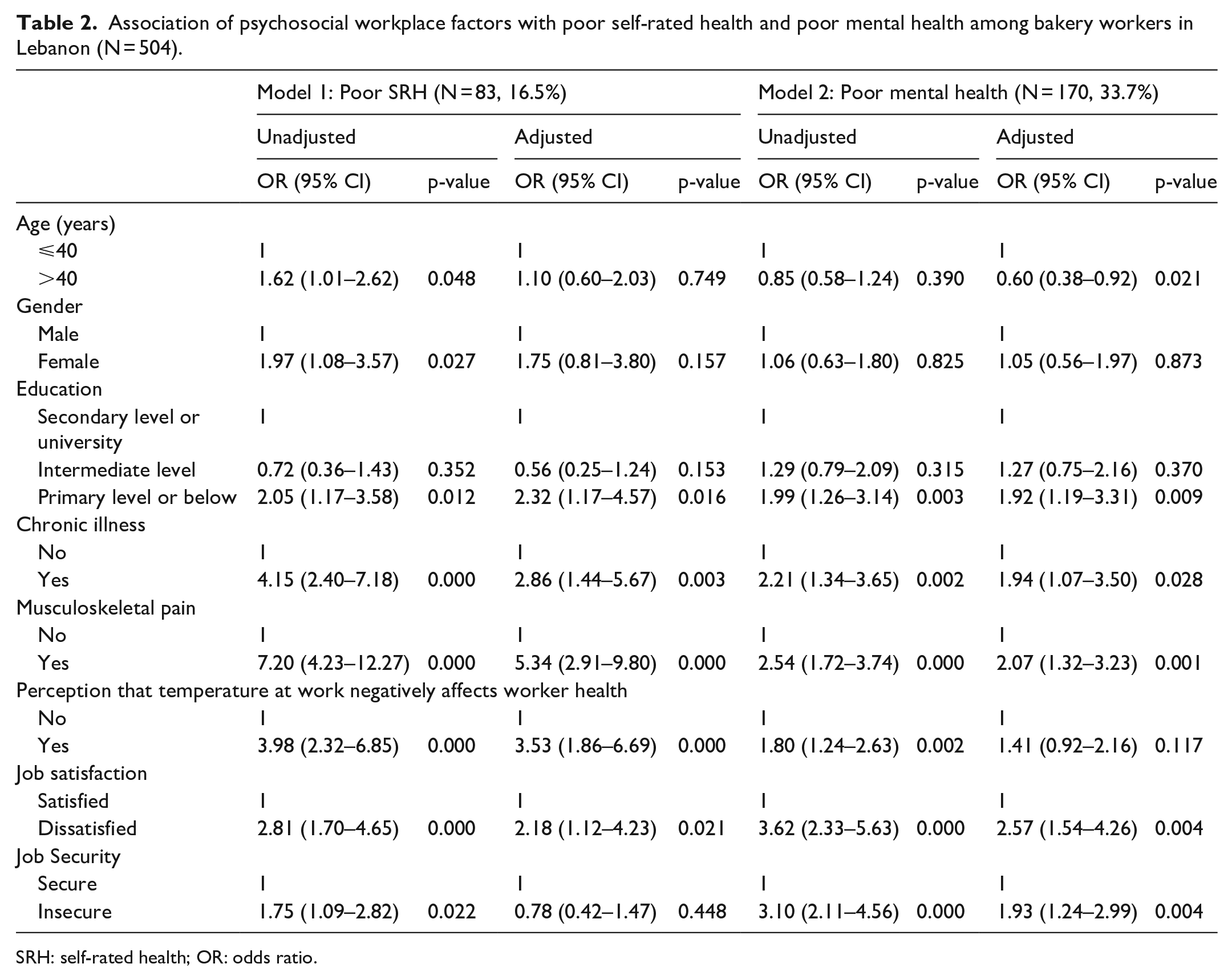
SRH: self-rated health; OR: odds ratio.
SRH
Education did not show a significant relationship with health ratings, except for workers with primary level or below reporting poor health (OR = 2.32; 95% CI = 1.17–4.57). Workers who were dissatisfied with their job were twice as likely to report poor health (OR = 2.18; 95% CI = 1.12–4.23). The physical health of the worker was an important mediating factor, as those suffering from a chronic illness were almost three times as likely to report poor SRH (OR = 2.86; 95% CI = 1.44–5.67) and those who reported musculoskeletal pain were five times as likely to report poor SRH (OR = 5.34; 95% CI = 2.91–9.80). Moreover, workers who perceived workplace temperature as negatively affecting their health were also significantly more likely to report poor SRH (OR = 3.53; 95% CI = 1.86–6.69).
Mental health
Workers who were dissatisfied with their job and those who believed that their jobs were insecure were more likely to report poor health (OR = 2.57; 95% CI = 1.54–4.26 and OR = 1.93; 95% CI = 1.24–2.99, respectively). The physical health of the worker was also associated with mental health. Workers who suffered from a chronic illness and those who reported musculoskeletal pain were twice more likely to report poor mental health (OR = 1.94; 95% CI = 1.07–3.50 and OR = 2.07; 95% CI = 1.32–3.23, respectively). Perception of the work environment temperature was not significantly correlated to mental health, while education level was only significant for workers with primary level or below (OR = 1.92; 95% CI = 1.19–3.31). Age was also significantly related to mental health, with older workers less likely to report poor mental health (OR = 0.60; 95% CI = 0.38–0.92).
Mental health, SRH, and the social environment at work
The findings of the bivariate analyses showed a gradient association between social and economic indicators and both self-rated and mental health ratings (Figures 1 and 2). Ninety-three percent of workers with both poor mental health and poor SRH reported low perceived economic status, while 52% reported job dissatisfaction, 63% reported job insecurity, and 46% reported earning less than 1,000,000 Lebanese Pounds (LBP) (around US$667) monthly. Alternately, workers who had neither poor mental health nor poor SRH reported less prevalence of perceived low economic status (79%), job dissatisfaction (14%), job insecurity (31%), and earning less than 1,000,000 LBP each month (26%). Furthermore, 43.5% of workers with both poor mental health and SRH reported rarely getting help from colleagues, compared with 23.2% who had neither SRH nor mental health rated as poor.

Relationship between social environment at work and workers’ mental and self-rated health.

Relationship between workers’ economic status and their mental and self-rated health.
There were similar trends found between mental health, SRH, and physical health indicators (Figure 3). Thirty-five percent of workers with both poor mental health and poor SRH reported having a chronic illness, and 78% reported musculoskeletal pain, compared with 9% of workers with a chronic illness and 23% with musculoskeletal pain among those who had none rated as poor. Among workers who reported neither health ratings as poor, 40% perceived the temperature at work as negatively affecting their health, compared with 82% of those reporting both poor mental and SRH.

Relationship between workers’ physical health and their mental and self-rated health.
Discussion
Despite bakery workers’ concern over the impact of high temperatures on their health (47.6%), the majority of workers were satisfied (77.6%) and were secure (59.3%) in their job. These findings reflect the pride that bakery workers’ take in their work. However, workers who were dissatisfied with their job (22.4%) and those who reported insecure employment (40.1%) were more likely to report poor mental and SRH. The strained economic conditions and the rising cost of living in the country are expected to exacerbate the poor work conditions for bakery workers.
The results also indicated that those who identify themselves as having poor mental and SRH were more likely to experience chronic health conditions. A similar gradient relationship between indicators of economic security and markers of health was found among a population of Palestinian refugees in Lebanon, most of whom work in low-wage jobs in the service and food sectors. 42
Consistent with findings in other studies, these results indicate associations between poor mental and SRH and worse physical health.30,46 Previous studies found that poor mental health was correlated with higher rates of musculoskeletal pain, often attributing the relationship to stress response.12,22,24,47 In a study on Spanish workers, the findings showed that workers with poor mental health were 50% more likely to report lower back pain. 48 Research has also linked chronic illness to poor mental health.49–51 Meanwhile, the relationship between poor SRH and physical health (chronic illness and musculoskeletal pain) is fairly self-evident, as people suffering from health problems are more likely to view their health as poorer. 36 Interestingly enough, rates of musculoskeletal pain were lower than in several of the other studies of traditional bakery industries.13,14 Future research might explore the social or structural factors contributing to these differences in reporting.
Consistent with other studies, poor SRH and mental health were associated with lower levels of education.52,53 Bakery workers with lower levels of educational attainment may experience higher levels of disadvantage and may be more likely to report poor SRH.
A sizable proportion of workers (47.6%) perceived that the temperature at work negatively affects their health. This finding underlines bakery workers’ concerns over the prevailing hot temperatures in the work environment. Baking in front of open fire is a workplace feature in most Lebanese bakeries. The study showed that workers who perceived workplace temperatures to negatively affect their health were more likely to report poor SRH and mental health. These findings were echoed by Chau et al., 31 who reported a positive association between workplace exposures and poor mental health.
The same relationship between job insecurity and poor mental health identified in this research was reported in Tsumtsumi et al. 54 However, this study did not find a significant association between job insecurity and SRH, as found by other research. 35 Unlike Chau et al., 31 this study did not find workplace pressure as significantly related to poor health outcomes. This result may suggest that the other variables in our analysis are confounding this relationship or that the questionnaire item does not adequately capture the pressures of bakery work. Alternately, work within bakeries with a small clientele may not result in intense psychological pressures.
This study recruited a majority of male participants (86%), limiting the possibility of stratifying the analysis by gender. The demographics of the bakery industry proved to be an obstacle to recruiting greater female participation, as bakery workers in Lebanon are predominantly males. The study also adopted a cross-sectional design restricting the ability to establish causality, which does not provide insight into how health status shifts as workers’ workplace, economic, and physical health variables shift over the life course. No power analysis was done due to the multiple hypotheses that were tested in the national bakery workers’ project in which this study was nested. Finally, the survey instrument relied on self-reported information, which may lead to underreporting and misreporting. For example, workers may only report major or chronic incidents of musculoskeletal pain in a 12-month period leading to underreporting. The sample may also be affected by the healthy worker effect, with lower levels of study participation among workers experiencing severe health challenges.
Implications for occupational health practice
This study evidenced the association between job dissatisfaction and job insecurity and poor indicators of health among bakery workers in Lebanon. This workforce lacks health insurance and basic social security that are not provided to the informal sector in Lebanon. This adds to the psychosocial burdens that bakery workers potentially face. Health protection and job security of bakery workers are, respectively, under the mandate of the Ministry of Public Health and the Ministry of Labour that may jointly revisit related policies to safeguard the health and safety and the job security of bakery workers whose work is a necessity for the country’s food security.
Compliance with occupational safety standards and the Lebanese Labour law, which depicts the maximum load of work hours allowed per week (48 h per week), 55 must be enforced through routine workplace inspections by the Ministry of Labour. Moreover, promoting a culture of safe work practices in bakeries will help in improving bakery workers’ health.
Conclusion
Bakery workers in Lebanon are at the intersections of multiple marginalities: the workforce is almost entirely poor and with limited educational capital and many are older and aging. Given the economic, social, and political realities, workers in the food sector are likely to become more vulnerable as an exploding labour force threatens their job security, which has been reported by a sizable proportion of our study participants (41%). Studying the health of low-wage workers makes visible the less obvious societal impacts of poverty. This study showed that job dissatisfaction, job insecurity, musculoskeletal pain, chronic illness, and lower levels of education were all associated with poor mental health and SRH among low-income bakery workers in Lebanon.
This research provided evidence for the need to intervene to improve the conditions, and specifically the job security, of bakery workers in Lebanon’s informal sector.
Supplemental Material
Questionnaire-8May20 – Supplemental material for Mental and self-rated health of bakery workers in Lebanon: A national study
Supplemental material, Questionnaire-8May20 for Mental and self-rated health of bakery workers in Lebanon: A national study by Rima R Habib, Nataly W El-Haddad, Kareem Elzein and Safa Hojeij in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Ms. Hind Farah for coordinating the data collection activities and GeoVision S.A.L for providing the GIS maps to identify bakeries in Lebanon.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University Research Board at the American University of Beirut.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board (IRB) at the American University of Beirut (no. FHS-RH1.03).
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.