
Abstract
Background:
Healthcare professionals in Taiwan are exposed to a myriad of occupational health and safety hazards, including physical, biological, chemical, ergonomic, and psychosocial hazards. Healthcare professionals working in hospitals and healthcare facilities are more likely to be subjected to these hazards than their counterparts working in other areas.
Objectives:
This review aims to assess current research literature regarding this situation with a view to informing policy makers and practitioners about the risks of exposure and offer evidence-based recommendations on how to eliminate or reduce such risks.
Methods:
Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses review strategy, we conducted a systematic review of studies related to occupational health and safety conducted between January 2000 and January 2019 using MEDLINE (Ovid), PubMed, PMC, TOXLINE, CINAHL, PLOS One, and Access Pharmacy databases.
Results:
The review detected 490 studies addressing the issue of occupational health and safety hazards; of these, 30 articles were included in this systematic review. These articles reported a variety of exposures faced by healthcare professionals. This review also revealed a number of strategies that can be adopted to control, eliminate, or reduce hazards to healthcare professionals in Taiwan.
Conclusion:
Hospitals and healthcare facilities have many unique occupational health and safety hazards that can potentially affect the health and performance of healthcare professionals. The impact of such hazards on healthcare professionals poses a serious public health issue in Taiwan; therefore, controlling, eliminating, or reducing exposure can contribute to a stronger healthcare workforce with great potential to improve patient care and the healthcare system in Taiwan. Eliminating or reducing hazards can best be achieved through engineering measures, administrative policy, and the use of personal protective equipment.
Implications:
This review has research, policy, and practice implications and provides future students and researchers with information on systematic review methodologies based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses strategy. It also identifies occupational health and safety risks and provides insights and strategies to address them.
Introduction
According to the World Health Organization (WHO), 1 an estimated 59 million people work in healthcare facilities globally, accounting for roughly 12% of the working population. The WHO 2 also reports that all healthcare workers, including healthcare professionals, are exposed to occupational hazards. The International Labour Organization (ILO) 3 reported that millions of healthcare workers suffer from work-related diseases and accidents, and many succumb to occupational hazards. Scholars and practitioners in the field of healthcare and occupational health and safety (OHS) are striving to raise awareness of the risk factors and importance of workplace health and safety among this population.1,3,4
Schulte et al. 5 defined an occupational hazard as the short-term and long-term dangers or risks associated with unhealthy workplace environments. Tullar et al. 6 and Joseph and Joseph 7 stated that the healthcare workers at greatest risk are doctors, healthcare professionals, nurses, laboratory technicians, and medical waste handlers.
Occupational hazards pose health and safety risks and have negative impact on the economy, which accounts for roughly a 4% loss in global annual gross domestic product (i.e. $2.8 trillion annually). 3 The WHO, 2 ILO, 3 and Nelson et al. 8 noted a lack of universally applicable data on the impact of occupational hazards.
OHS hazards, and their negative impacts on health and well-being among healthcare professionals, is an issue of growing concern in the Asia and Pacific region, particularly in Taiwan; however, research in this area has been somewhat limited. According to the Taiwanese Ministry of Health and Welfare (MOHW) 9 in Taiwan, 182,019 health and medical personnel are working at health care organizations in Taiwan, including 33,516 healthcare professionals and 15,016 pharmacist assistants. The healthcare professionals serve a Taiwanese population of 23,590,744 in 22,384 medical care institutions (490 hospitals and 21,894 clinics). 10 Of the 490 hospitals, 81 are public and 409 are privately owned; of the 21,894 clinics, 440 are public and 21,454 are privately owned. 10
Taiwanese healthcare professionals face a variety of OHS hazards, which increase the incidences of work-related disease, the country’s burden of disease, the total number of accidents, the incidences of job-related health problems, and the number of cases involving incapacitation or disablement. 9 This study reviewed previous works on OHS hazards, as well as their risk factors and control strategies, with a focus on healthcare professionals in Taiwan.
Methods
Search strategy
Cochrane 11 identified eight steps of a systematic review, which are adopted in this study.
Eligibility criteria
This study employed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol to organize the flow of information through the various steps of the review. We used the following key words in our literature search: occupational health and safety, risk factors, healthcare professionals, control strategies, and Taiwan. Studies conducted between January 2000 and December 2018 were included in the study.
The data sources for this systematic review included Cengage, PsycINFO, MEDLINE (Ovid), ProQuest, PubMed, PMC, TOXLINE, PLOS ONE, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Scopus, Access Pharmacy, Web of Science, ScienceDirect, NIOSHTIC-2, and National Health Insurance Research Database (NHIRD); unpublished government, academic, and agency articles, research or reports mainly WorldCat, AHRQ EPC, Google Scholar, and the WHO research database.
Inclusion and exclusion criteria
To ensure specificity and exclude irrelevant studies, we employed Boolean logic (AND, OR, NOT) in combining terms as search strings. 12 The operator AND was used to reduce the search yield for two key terms (e.g. “healthcare professionals (P) AND occupational health and safety”). The operator OR was used to increase the search yield (e.g. “healthcare professionals AND occupational health and safety OR risk factors”). Note that in this example, the two search terms are synonyms. The operator “NOT” was used to exclude specific terms or term combinations. 13
This research obtained a large number of initial articles (n initial = 490); however, the application of inclusion and exclusion criteria considerably reduced the number of articles for inclusion in the review (n = 30 articles). The 30 articles focused on OHS, occupational hazards, and healthcare professionals in Taiwan. Figure 1 presents a flow diagram depicting the application of eligibility criteria, the process of identification and screening, and the reasons for inclusion and exclusion.

PRISMA flow diagram.
Data extraction: validity and reliability
In documenting and assessing individual publications, we collected key information from the relevant studies to populate an evidence table (see Appendix C) and conducted a critical appraisal of the included studies. 12 The study population included adult pharmacy workers (male and female). Data were extracted only from studies that included samples that were deemed significant given the justification of the authors of the studies. A critical appraisal of all studies was performed to assess their quality in terms of validity and reliability, as based on performance bias, information bias, selection bias, and detection bias. Cochrane 11 and Khan et al. 16 reported that biases tend to exaggerate or underestimate the “true” outcome of exposure to an occupational hazard. Our ultimate objective was to compare (without any form of bias) groups that were exposed to occupational hazards and those that were not exposed in terms of risk factors and outcomes. 16
For the sake of validity and reliability, all of the studies selected for inclusion were prospective in nature and included data pertaining to exposure and outcomes, while controlling confounding factors. We also looked for studies with high internal reliability (consistency across items within a test) and high external reliability (consistency in agreeability between uses/rates). 12 In our final analysis, we considered whether the research had been conducted in an appropriate manner (internal validity). 13 We also considered the generalizability of the results, that is, whether the results were pertinent to other situations (external validity).
Data synthesis
The final step involved the synthesis of evidence from the included studies; that is, organized into homogeneous categories, under which the results were to be summarized. The evidence was also graded (i.e. assessed in terms of quality) and integrated (i.e. weighted across categories to address the multidisciplinary nature of OHS research). 12 In this review, the synthesis, grading, integration, interpretation, and summary of the evidence were presented in narrative form, due to difficulties in textual and statistical pooling. After completing our systematic review, we employed the PRISMA reporting scheme, which is endorsed for OHS studies by Hempel et al. 12 Briefly, the PRISMA structure is laid out in the following format: topic, summary/abstract, introduction, methods, results, conclusion, and recommendations. 12 A meta-analysis was not conducted.
Results
The ILO categorizes OHS hazards that affect healthcare professionals as biological, chemical, physical, ergonomics, and psychosocial. 17 From the 30 studies in this review, this study identified the OHS hazards, injuries, and diseases affecting healthcare professionals working in hospitals and healthcare facilities.
Biological hazards
This section provides the biological hazards, as identified in the review, as the most commonly encountered in hospitals and healthcare facilities in Taiwan. According to WHO, the managers and administrators of hospital and healthcare facilities, in our case those in Taiwan, should carefully assess the potential for exposure to biohazards and put effective biohazard control plans in place. The following chart provides a summary of the identified biological hazards, their risk factors, and control strategies (Table 1).
Biological hazards.

Chemical hazards
The review established some of the most commonly faced chemical hazards present in hospitals and healthcare facilities, as well as the documented control strategies, which are summarized in Table 2.
Chemical hazards.

PPE: personal protective equipment; API: active pharmaceutical ingredient.
Physical hazards
Physical hazards, which are defined as environmental risk factors that can harm the body without contact, were found to account for a substantial proportion of risks among healthcare professionals in Taiwan.4,42–44 The physical hazards, risk factors, and control strategies are summarized in Table 3.
Physical hazards.

Ergonomic hazards
The review established that healthcare professionals are exposed to musculoskeletal disorders and injuries, such as low back pain due to the nature of their work, such as lifting patients. 44 Table 4 summarizes the risk factors and control strategies for this hazard.
Ergonomic hazards.

Psychosocial hazards
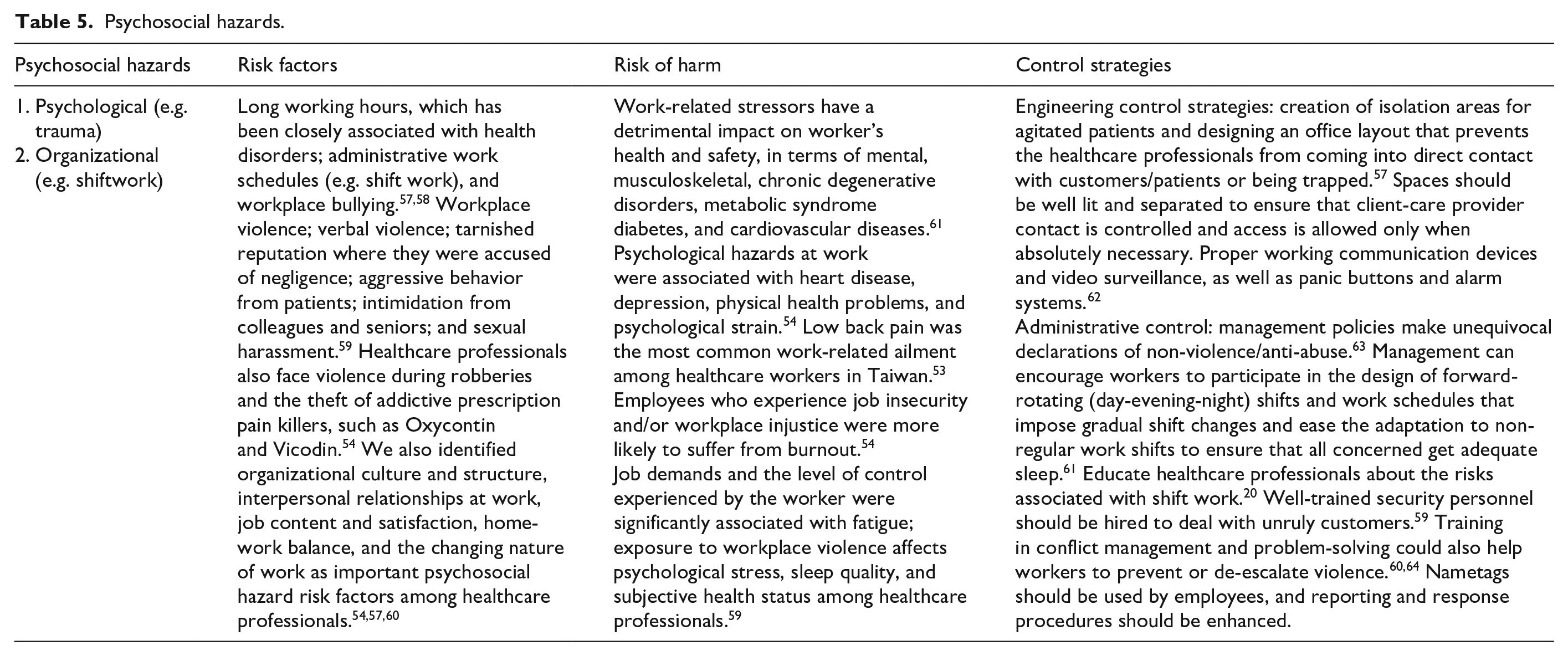
Psychosocial hazards have attracted considerable attention in the research community, as well as among policy makers and practitioners in healthcare.53–55 This study found that in Taiwan, psychosocial hazards have prompted a larger number of studies combining physical, chemical, and biological hazards. The WHO 56 reported that psychosocial hazards are closely linked to work-related stress, workplace violence (e.g. violent patients), and other workplace stressors. Table 5 provides a summary of the risk factors and control strategies of psychosocial hazards.
Psychosocial hazards.
Discussion
This review provides detailed information regarding the OHS hazards that affect healthcare professionals working in hospitals and healthcare facilities in Taiwan. The review summarizes the risk factors for hazards, as well as the control strategies to control, eliminate, or reduce them. From the reviewed studies, it was clear that OHS hazards can potentially result in a number of injuries, sickness, and harm. A wide range of OHS hazards were identified, including biological hazards 14 chemical hazards, 65 ergonomic hazards, psychosocial hazards, and physical hazards.59,62
The review has shown that healthcare professionals are at a significantly high risk of occupational related hazards. 56 Injuries and sickness prevent healthcare workers from discharging their duties effectively, which can have negative impact on the overall healthcare system in Taiwan. Physical hazards, such as falls, noise, and mechanical hazards, could have long-term physiological effects, such as hearing impairments; therefore, there is need to introduce various control strategies, such as engineering noise control measures. There should be the provision of good PPE for healthcare professionals to protect themselves from physical harms in the workplace.
According to our findings, it is evident that healthcare professionals are exposed to chemical hazards, some of which can be carcinogenic. There is also the risk of exposure to occupational dermatitis. It is therefore important that healthcare professionals are screened for cancer on a regular basis. The workers can also be trained about skin care and be provided with safety equipment and other useful interventions, such as sunscreen cream. Such efforts can help in early detection, prevention, and intervention.
As part of their routine occupation, biological hazards can affect healthcare professionals due to contact with patients and visitors. The review of healthcare professionals on duty demonstrates how important it is to manage blood borne and airborne biological pathogens in the healthcare workforce. 20 There should be administrative guidance and training on how healthcare professionals can deal with biological hazards, and these professionals should be encouraged to report work-related incidents as soon as they occur or are suspected to have occurred to aid early intervention.
Ergonomic hazards in healthcare professionals tend to arise from lifting patients and hospital equipment. This requires careful prevention, assessment, and intervention, as the impact of ergonomic hazards on the musculoskeletal system of the affected healthcare professionals cannot be ignored. 34 Hospital administrators need to alleviate frequent job pressures by providing the necessary safe and ergonomic equipment, and hiring an adequate number of personnel. The professionals can work in properly planned shifts and teams to reduce fatigue, they should be trained in the correct techniques for lifting patients and equipment, and policies should be enforced to ensure compliance.
The findings on psychosocial hazards show that healthcare professionals can be affected by mental and psychological hazards, such as stress, as it is evident that healthcare professionals who suffer from stress are likely to suffer from fatigue and exhaustion. Healthcare professionals are trained to show less emotion, and thus, find it difficult to seek medical intervention. There is need for counseling and stress management for healthcare professionals, and the workers should be trained to manage stress. The workplace should be designed in such a manner as to prevent invasion, harassment, and violence against healthcare professionals. Overall, hospital administrations and healthcare professionals should focus on evidence-based strategies (engineering, administrative, and PPE) to manage OHS hazards.
Conclusion
The increasing prevalence of occupational hazards and work-related diseases among healthcare professionals in Taiwan is a concern. 66 Risk factors include exposure to hazards and a failure to follow hierarchical control strategies. Health care workers and administrators must work together to eliminate or minimize these hazards through the introduction of and strict adherence to engineering, administrative, and personal protective equipment (PPE) controls. The perceptions of workers can greatly affect their implementation of risk-mitigation strategies. 20
Study limitations
Selection bias is a concern here, despite the fact that we selected published and peer-reviewed articles, as well as unpublished but authoritative gray articles; the fact is that other unverifiable but potentially valuable reports were no doubt excluded. 67 Our reliance on observational studies (to the exclusion of intervention studies) and the heterogeneity of the included articles (in terms of methodology) posed a risk of bias and limited standardization. 68
Implications for further research
This study discovered relatively little research focusing on hospital workers in Taiwan, and thus, further empirical studies focusing on this group of healthcare givers are required and recommended. 68 Researchers should focus on the health status, work performance, and workplace retention of healthcare professionals, including the prevalence of morbidity and mortality. 67
Implication for policy and practice
The insights in this review provide a valuable reference for policy makers in establishing goals to deal with workplace hazards. 68 Hazard control strategies must be based on objective assessments of existing risks and the most appropriate measures to deal with them. 20
Conclusion
This systematic review confirmed a positive correlation between OHS hazards (biological, physical, chemical, and psychosocial), and work-related injuries, occupational health problems, and work-related diseases. The burden of disease and attributable fraction of work-related diseases and occupational injuries has been shown to cause considerable social and economic losses for employees, families, companies, countries, and societies at large. 8 Generally, the burden of disease is assessed using disease/disability adjusted life years. The burden of disease is measured as the impact of morbidity and premature mortality within a given area.2,69
Scholars and professionals agree that reducing, substituting, or eliminating OHS hazards in healthcare facilities is important for healthcare workers, helps to ensure patient safety, and enhances the overall quality of healthcare. 7 Many researchers have used the “hierarchy of controls,” which is based on the assumption that interventions are most effective when implemented at the source and least effective when applied at the worker level. 20
Gorman et al. listed control interventions from most to least effective as follows: elimination, substitution, engineering, administrative, and PPE. Researchers have also emphasized the importance of eliminating hazards or substituting hazardous materials with less hazardous materials.20,70
Taimela et al. 71 argued that administrative controls, such as training and ensuring adequate staffing, are crucial to eliminating or minimizing occupational hazards. Engineering controls, such as redesigning work spaces, ensuring adequate ventilation, and introducing automated systems for repetitive tasks, were emphasized by Liberati et al. 72 PPE, such as the use of gloves, clothing, and eye wear, are considered the least effective and have the most profound consequences in the event of failure by exposing the individual directly to the hazard. 20 Nonetheless, many researchers and professionals agree that all such controls should be applied collectively, in order to minimize the effects of hazards.20,70–72
Supplemental Material
Online_Appendix – Supplemental material for Occupational health and safety hazards faced by healthcare professionals in Taiwan: A systematic review of risk factors and control strategies
Supplemental material, Online_Appendix for Occupational health and safety hazards faced by healthcare professionals in Taiwan: A systematic review of risk factors and control strategies by Lin Che Huei, Lin Ya-Wen, Yang Chiu Ming, Hung Li Chen, Wang Jong Yi and Lin Ming Hung in SAGE Open Medicine
Footnotes
Authors’ note
The manuscript has not previously been published and is not under consideration by another journal.
Author contributions
Conceptualization was done by L.M.H., L.C.H., and W.J.Y. Data curation was done by L.M.H., L.C.H., W.J.Y. All authors did the Investigation and arrived at a Methodology together. Validation was done by Y.C.M., L.Y.W., and H.L.C. Resources were collected by L.M.H. and J.Y.W. Supervision was done by L.M.H. and L.C.H. Writing—original draft was done by L.M.H., L.C.H. Writing—review and editing was done by all the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethical approval was not sought for this study because this is a systematic review and all the literature has been published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.