
Abstract
Objectives:
Despite the well-established association between self-rated health and mortality, research findings have been inconsistent regarding how men and women differ on this link. Using a national sample in the United States, this study compared American male and female older adults for the predictive role of baseline self-rated health on the short-term risk of mortality.
Methods:
This longitudinal study followed 1500 older adults (573 men (38.2%) and 927 women (61.8%)) aged 66 years or older for 3 years from 2001 to 2004. The main predictor of interest was self-rated health, which was measured using a single item in 2001. The outcome was the risk of all-cause mortality during the 3-year follow-up period. Demographic factors (race and age), socio-economic factors (education and marital status), and health behaviors (smoking and drinking) were covariates. Gender was the focal moderator. We ran logistic regression models in the pooled sample and also stratified by gender, with self-rated health treated as either nominal variables, poor compared to other levels (i.e. fair, good, or excellent) or excellent compared to other levels (i.e. good, fair, or poor), or an ordinal variable.
Results:
In the pooled sample, baseline self-rated health predicted mortality risk, regardless of how the variable was treated. We found a significant interaction between gender and poor self-rated health, indicating a stronger effect of poor self-rated health on mortality risk for men compared to women. Gender did not interact with excellent self-rated health on mortality.
Conclusion:
Perceived poor self-rated health better reflects risk of mortality over a short period of time for older men compared to older women. Clinicians may need to take poor self-rated health of older men very seriously. Future research should test whether the differential predictive validity of self-rated health based on gender is due to a different meaning of poor self-rated health for older men and women and whether poor self-rated health reflects different health statuses based on gender.
Background
For more than half a century, single-item measures of self-rated health (SRH) have been used in community surveys.1,2 The widespread application of single-item SRH measures is due to the high efficiency as well as high validity of single-item measures in estimating the overall health of individuals.3–6 The combination of high feasibility, 7 low cost, 8 and high validity5,6 has made SRH a widely accepted health indicator for national surveys in most countries.8,9 In the United States, a single-item SRH measure is being used to monitor the health of Americans, as recommended by the Institute of Medicine (IOM).10,11
Poor SRH predicts medical conditions, 12 healthcare use,8,11 and other aspects of morbidity, 13 such as quality of life 14 and physical function. 15 Poor SRH is also a strong predictor of mortality risk. 10 The link between SRH and mortality is above and beyond objective health measures16–20 and holds true across a wide range of populations, geographic regions, as well as follow-up periods.16–21 Individuals who perceive their health to be poor are at a higher risk of mortality compared to those who perceive their health as good, and individuals who report their health as excellent are at the lowest risk of mortality compared to others.7,8,16–19
For at least three reasons, we were interested in comparing the effects of SRH on the short-term risk of mortality across genders. First, while the predictive role of SRH on mortality may differ among men and women,22–24 studies have reported inconsistent results.23,25–29 While most studies have found a stronger predictor role of SRH among men than women,24,30 there are also studies that have not found any gender differences,26,31 or even a stronger association among women. 27 For instance, Benyamini and colleagues studied how SRH predicts mortality over 4 and 9 years in an Israeli national sample of 622 women and 730 men. While for both genders SRH predicted short-term mortality (4 years of follow-up) rather than long-term mortality (9 years of follow-up), the highest predictive role was seen for older women, compared with any other gender by age groups. 23 In a study by Grant and colleagues, SRH better predicted mortality for men than women. This study found a stable association between poor SRH and risk of mortality for men over varying follow-up periods; however, such a link declined over time for women. 28
Second, most studies have studied long-term risk of mortality, and less is known on short-term risk. Ferraro and Kelley-Moore 32 showed that SRH better predicts the risk of mortality in the short-term rather than the long-term. In addition, by focusing on the short-term effects of SRH on mortality, we could avoid the problem of change in covariates during the follow-up periods, as in shorter time periods covariates are less likely to change. This study could help us replicate our SRH–long-term mortality risk for short-term follow-up periods. 20 Thus, we focused on mortality over a short period rather than a long period. Third, SRH has previously been treated as nominal and ordinal variables, 20 so it is unknown whether it is poor SRH that predicts mortality or excellent SRH that predicts survival. 23
We conducted this study to explore gender differences in the association between SRH and short-term risk of all-cause mortality among older Americans.
Methods
Design and setting
This was a longitudinal panel study with 3 years of follow-up. Data came from Waves 1 and 2 of the Religion, Aging, and Health Survey, a household survey from 2001 until 2004.
Ethics
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants included in the study. The University of Michigan Institutional Review Board (IRB) approved the study protocol.
Sampling and participants
The population of this study at the baseline interview was limited to White or Black older Americans. All participants were household residents, noninstitutionalized, English-speaking, and at least 66 years of age. Geographically, the study was limited to the contiguous United States (i.e. residents of Alaska and Hawaii were excluded). Older Blacks were over-sampled and represented roughly half the sample (752 Blacks). The overall response rate for the baseline interviews was 62%. The study population was limited to Christians or those who were never associated with any faith. Analytical sample included 1500 older adults (573 men (38.2%) and 927 women (61.8%)). A face-to-face interview was used for data collection.
Measures
All interviews were conducted by Harris Interactive. SRH measured at baseline (2001) was the main predictor of interest, and all-cause mortality over the 3-year follow-up period was the main outcome. Demographic factors (race and age), socio-economic factors (education and marital status), and health behaviors (smoking and drinking), all measured at baseline (2001), were covariates. Gender was the moderator.
SRH
Respondents were asked to classify their SRH as excellent, good, fair, or poor. As past literature has treated SRH in distinct ways,20,33–36 we treated SRH as a nominal variable, as well as an ordinal variable. First, we calculated the effects of “poor health” compared to other levels (i.e. excellent, good, fair). Then, we tested the effect of “excellent” versus others (i.e. good, fair, or poor). These cutoff points are commonly used in the literature. Ordinal SRH was coded from 1 (excellent) to 4 (poor), with higher values indicative of worse SRH.33–36
All-cause mortality
Information on occurrence of death from 2001 through 2004 was obtained through the informants, death certificates, and the national death index. Mortality during the follow-up was treated as a dichotomous variable, irrespective of time and cause of death. In 1460 cases (97.3%) from 1500 individuals, survival status in 2004 was known. Overall, 208 individuals deceased. From this number, 82 were male and 126 were female.
Demographic factors
Race was measured based on self-identified race and ethnicity (Blacks or African Americans vs Whites or Caucasian), with Whites being the reference category. Age was measured in 2001, and treated as a continuous measure.
Socio-economic factors
Socio-economic status was measured using education (high school diploma vs without high school diploma (reference category)) and marital status (married vs any other status (reference category)) in 2001. The item for the measurement of education was “Did you get a high school diploma or pass the high school equivalency test?” Both variables were treated as nominal variables.
Health behaviors
Health behaviors (smoking and drinking) were measured in 2001 and were treated as nominal variables. Items included “Do you ever drink beer, wine, or liquor?” and “Do you smoke cigarettes now?” Response items included (1) Yes, (2) No, (3) No answer, (4) Not sure, and (5) Decline to answer.
Statistical analysis
We used SPSS 20.0 (IBM Corporation NY, USA) for data analysis. In our models, SRH was the independent variable, mortality was the main outcome variable, and demographic factors (race and age), socio-economic factors (education and marital status), and health behaviors (smoking and drinking) were covariates. Gender was our moderator of interest. We fitted logistic regressions without (Model 1) and with interaction (Model 2) in the pooled sample and specific to men (Model 3) and women (Model 4). We used logistic regressions to model mortality, independent of its time, because of lack of access to time of death. 37 Odds ratios (ORs), 95% confidence intervals (CIs), and p-values were reported. Baseline SRH was missing in four cases.
Survival status was missing in 112 individuals (7.5%) because researchers could not locate the participants. Variables such as gender and age were not missing in any individuals. Smoking and drinking were missing in two cases. Marital status, education, and age were missing in 12, 14, and 14 cases, respectively. We did not impute any data but rather used our model on the individuals with complete data.
Results
The study followed 1500 men and women for 3 years. Overall, 208 (13.87%) participants were found to be deceased. Of this, 82 were men and 126 were women.
Table 1 presents descriptive statistics overall based on gender. As this table shows, compared to men, women reported worse SRH, had lower education, were less frequently married, were less frequently a current smoker, and were less frequently a lifetime drinker.
Descriptive statistics for the analytic sample, stratified by gender and overall.
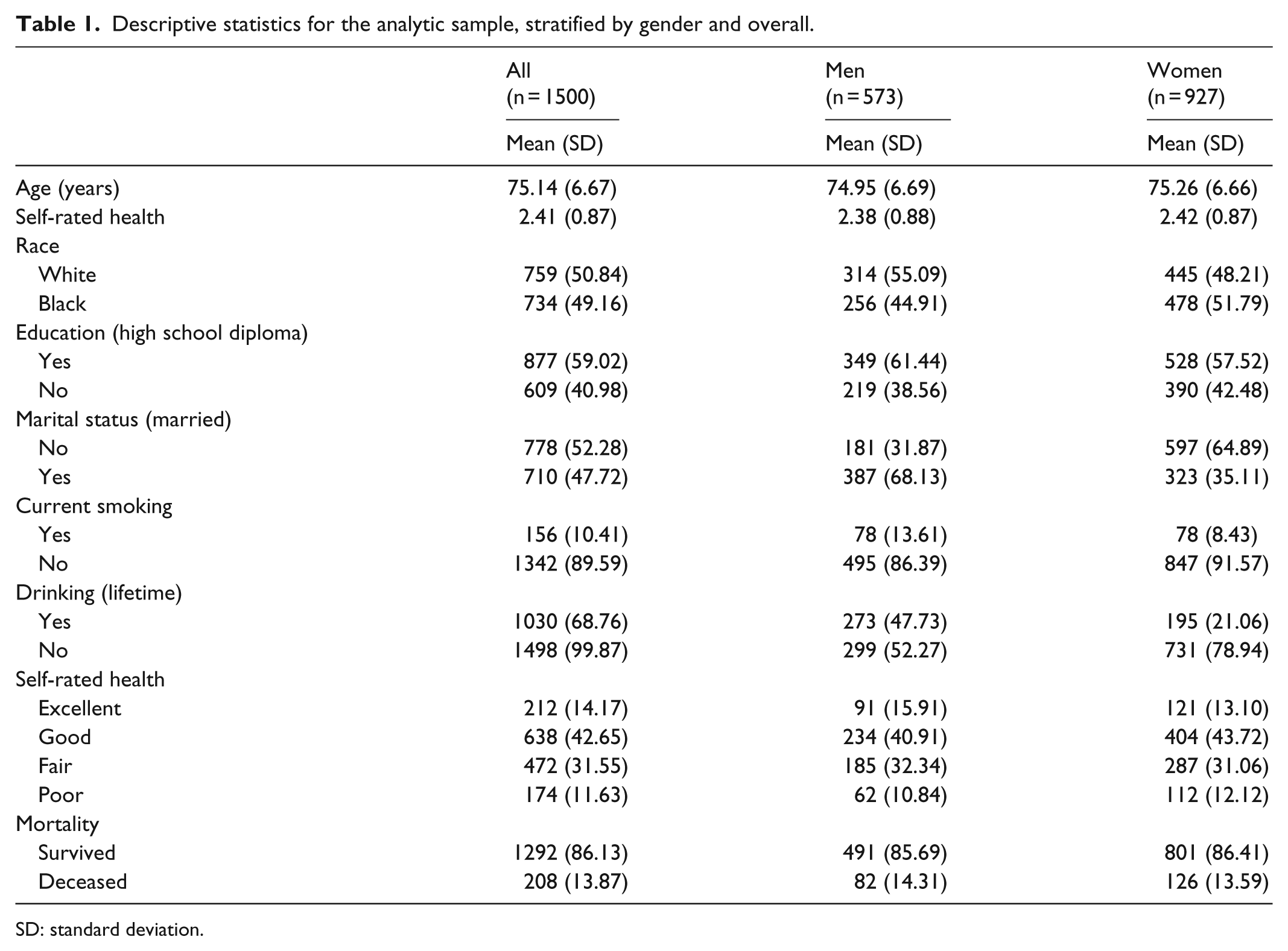
SD: standard deviation.
Table 2 shows the results of three logistic regression models. Model 1 was fitted in the pooled sample, and Model 2 and Model 3 are stratified models based on gender. In the pooled sample, as well as in both men and women, compared to those in excellent health, those with fair or poor health were at a higher risk of mortality, with the risk being larger for poor health than fair health. However, mortality of those who perceived their health to be good was not significantly different from those who found themselves in excellent health.
The association between baseline self-rated health (2001) and subsequent all-cause mortality (2001–2004) using logistic regression among 573 men and 927 women.

OR: odds ratio; CI: confidence interval; SRH: self-rated health.
SRH treated as an ordinal measure.
Table 3 summarizes the results of logistic regressions where SRH was treated as a dichotomous variable, excellent health versus others. According to this table, excellent health did not interact with gender on risk of mortality. However, excellent health was predictive of mortality among men but not women.
The association between baseline self-rated health (2001) and subsequent all-cause mortality (2001–2004) using logistic regression in the pooled sample (n = 1500).

OR: odds ratio; CI: confidence interval; SRH: self-rated health.
SRH treated as a nominal variable, comparing category excellent to others (good, fair, poor) SRH.
Table 4 provides a summary of logistic regressions where SRH was treated as a dichotomous variable, poor health versus others. According to this table, poor health was predictive of a higher risk of mortality in the pooled sample, and for men as well as for women. Poor health had an interaction with gender, suggesting a stronger effect of baseline poor health on mortality among men compared to women.
The association between baseline self-rated health (2001) and subsequent all-cause mortality (2001–2004) using logistic regression in the pooled sample (n = 1500).

SRH treated as a nominal variable, comparing category poor to others (excellent, good, fair) SRH.
OR: odds ratio; CI: confidence interval; SRH: self-rated health.
Discussion
We found a stronger predictive role for poor SRH on the risk of mortality over a 3-year period for older men compared to older women; however, we could not replicate this finding for excellent SRH. Thus, while SRH predicts 3-year mortality risk, reporting “poor” health better indicates high mortality risk for older men than older women. Reporting “excellent” health, however, similarly reflects a lower risk of mortality among older men and women.
Our overall finding that SRH predicts risk of death in the pooled sample is in line with previous research works.5,8,10,16,17,38 Similar to our findings, Spiers et al. 24 found a stronger predictive effect of SRH in men than in women. Grant and colleagues also showed a stable association of poor SRH with mortality among men over varying follow-up periods. However, the link showed a decline over time among women. 28 There are, however, several studies that did not find any gender differences in the SRH–mortality risk.23,26,31There are also studies that have shown a stronger association between SRH and mortality among women compared to men.23,27,28 For instance, Onawola and LaVeist conducted a 6-year study of survival among the 1209 African American respondents in the Longitudinal Study on Aging (LSOA) and showed that SRH was an independent predictor of mortality for women, but not men. 30 Benyamini et al. 23 studied an Israeli nationally representative sample of 622 women and 730 men and found that the highest predictive role of SRH was for the older (ages 75–84 years) women, compared with other gender by age groups. Grant et al. 28 used data from 4380 noninstitutionalized individuals aged 70 years and older and also found a weaker link between SRH and mortality for men than for women.
Different studies have controlled for different sets of covariates. Benyamini et al. 23 adjusted for sociodemographic and health covariates, such as age, place of birth, education, source of income, living arrangement, chronic conditions (heart disease, diabetes, hypertension, etc.), activities of daily living (ADL), physical activity, cognitive status, and depressive symptoms. Grant et al. controlled for age, race, education, marital status, body mass index, difficulty performing ADL, social contacts, self-reported stroke, heart disease, cancer, diabetes, and recent hospitalization.
There is still a need for studies that explore various mechanisms by which SRH may have a better predictive role for mortality among men or women. According to the “sponge” hypothesis proposed by Wolinsky and Tierney, women have a higher awareness of their physical symptoms. Thus, despite a higher accuracy of SRH among women, their reports of chronic disease and symptoms are also more accurate, leaving little information to be supplemented by SRH. This phenomenon may result in a weaker link between SRH and mortality association for women, when health status is controlled. 27 Benyamini and colleagues showed that women’s SRH is more inclusive and more sensitive to a wider range of health problems and better reflects negative affect. In their study, better reflection of affect in SRH among women explained the weaker association of SRH and mortality among women, compared with men. 29 The fact that SRH more commonly reflects life-threatening conditions among men may be another explanation for the stronger predictive role of SRH in men than in women. 24 Finally, as women have a longer life expectancy than men and experience more years of disability and ill health, 39 on average, elderly men who perceive their health to be poor are more likely to be closer to death than women of the same age who believe their health is poor. Additionally, on average, elderly women who rate their health as excellent live longer than men of the same age who rate their own health as excellent. 23 In a study by Singh-Manoux et al., 18 using the Whitehall II study, SRH predicted mortality equally well in men and women; however, the covariates better explained the SRH–mortality relationship in men compared with women, suggesting that SRH better reflects baseline health status among men. Gender also alters trajectories of SRH over the life-course, which may explain why SRH differently predicts mortality of men and women. While men have higher SRH throughout most of adulthood than women, men experience steeper linear rates of decline than women. Thus, decline in SRH better predicts subsequent decline after late adulthood for men than for women. 40
Our findings have implications for clinical and public health practices with older men and women. The better predictive power of SRH on the subsequent risk of mortality among men compared to women advocates for the application of a single-item SRH measure as a standard screening tool for detection of the health needs of elderly men. In other words, solely relying on single-item SRH measures may not equally detect the risk of premature death among older women in the United States.6,41,42 Our findings also suggest that SRH may not be a valid tool for a comparison of the health status of men and women as it differently reflects mortality risk across genders. Solely relying on single-item SRH measures to detect the individuals with the highest health needs in geriatric settings may result in more error for women than men. Still, SRH should be considered a strong measure for health assessment for daily practice and outcome evaluation. For older women, however, we recommend other measures be supplemented for screening and monitoring purposes.
While there were gender differences in the mortality risk associated with poor health, we could not find any gender difference in the survival benefit associated with reporting excellent health among older adults. SRH has both threshold (increase in mortality after a certain level of SRH) and gradient (each incremental increase in SRH) effects on the risk of all-cause mortality.10,16,17 We also found a graded association between SRH and mortality (Table 3), at least for good, fair, and poor SRH. However, we did not find evidence for the protective effect of excellent health on mortality. The literature has reported a dose–response pattern in the SRH–mortality association, suggesting that any incremental decline in SRH from excellent to poor increases subsequent risk of mortality.10,16,17
The study adds to the available literature. This is because of the inconsistency in the literature and the focus of most studies on longer periods.19,43–47 Future research should test possible explanations for differential SRH–mortality association based on gender. Future studies should also adjust for affect, chronic disease, type of chronic disease, coping, perceived control, stigma, symptoms, awareness about physical symptoms, and access and use of health services. The effects of all these confounders/mediators may possibly differ between men and women. 48
Our study was not free of limitations. First and foremost, this article only shows the relationship between SRH and mortality, without addressing any explanation for why men and women differ in this association. Second, our study did not include any objective measures of health, such as chronic medical conditions. 20 Another limitation was low response rate, which may have biased the estimates due to selection bias. This is particularly important because in most surveys, respondents tend to be healthier than non-respondents; thus, the results of the analysis may not be representative of the population as a whole. Time-varying covariates are believed to be less of a problem in this study, as we focused on the short-term risk of mortality. We intentionally focused on the short-term effects of SRH on mortality to avoid the problem of dynamic covariates in long follow-up periods. Ferraro and Kelley-Moore 32 have shown that SRH better predicts short-term mortality compared to long-term mortality. In short time periods, covariates are less likely to change. Finally, we used logistic regression rather than Cox regression because we did not have information on time of death. This can be a limitation, given the strength of the time-to-event analysis.49,50 There is a need for additional research to understand whether SRH differently reflects socio-economic status, healthcare use, and the physical and mental health of men and women.
To conclude, SRH may better predict short-term risk of mortality among male compared to female older Americans. This may be due to gender differences in health domains and the needs that poor SRH reflects.41,42,51 The same level of SRH may mean different health needs and trajectories for older men and women, even over a short period of time.
Footnotes
Acknowledgements
The Religion, Aging, and Health Survey was supported by National Institute on Aging (PI: Neal Krause; R01 AG 014749) and per the NIH Public Access Policy requires that peer-reviewed research publications generated with NIH support are made available to the public through PubMed Central. NIH is not responsible for the data collection or analyses represented in this article. Data were accessed through The Interuniversity Consortium for Political and Social Research (ICPSR), the Institute of Social Research, University of Michigan.
Authors’ contributions
S. A. designed and analyzed this work, drafted, and revised the article. S.A. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.A. was supported by the Heinz C. Prechter Bipolar Research Fund and the Richard Tam Foundation at the University of Michigan Depression Center.
Ethics
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants included in the study. University of Michigan Institutional review board (IRB) approved the study protocol.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.