
Abstract
Objectives:
The aim of this study is to report the aeroallergen sensitization profile in medically resistant chronic rhinosinusitis with or without nasal polyps and its relationship to asthma.
Methods:
Retrospective charts review of 402 chronic rhinosinusitis patients who failed to respond to medical treatment and scheduled for surgery at a tertiary academic center was performed. One hundred and fifty-five patients had chronic rhinosinusitis with nasal polyps and 247 patients had chronic rhinosinusitis without nasal polyps, furthermore; the two phenotypes were subdivided according to the presence or absence of asthma. Allergen-specific immunoglobulin E to 24 inhalant allergens was measured to all patients by the enzyme allergo-sorbent test.
Results:
The average age was 35 years (SD ± 13) with 236 males and 166 females. Two hundred and fifty-three patients (63%) were tested positive for at least one allergen with no significant difference between patients with or without polyp (in chronic rhinosinusitis with nasal polyps, 103 patients (66%) were positive compared with 150 patients (61%) in chronic rhinosinusitis without nasal polyps). There were no significant differences in the prevalence, type, and number of positive allergens between the two phenotypes. The prevalence of asthma was found to be 19% in patients with chronic rhinosinusitis without nasal polyps versus 46% in those with chronic rhinosinusitis with nasal polyps (p = 0.001), and the prevalence of high eosinophils was 27%, and 47% in both phenotypes, respectively (p = 0.0001).
Conclusions:
The prevalence of inhalational allergy in medically resistant chronic rhinosinusitis is high, however, this profile does not differ based on the presence of polyp. Patients with chronic rhinosinusitis with nasal polyps had a higher prevalence of asthma and blood eosinophils as compared with chronic rhinosinusitis without nasal polyps. Our results showed a little role of inhalant allergens in nasal polyps or asthma comorbidity in refractory sinusitis patients.
Introduction
Chronic rhinosinusitis (CRS) is a wide spectrum of disorders characterized by inflammation of the nasal and paranasal sinus mucosa for at least 12 consecutive weeks. 1 The condition is common and estimated to affect around 11% of the population with a significant impact on patients’ quality of life and socioeconomic burden. 2
CRS is classified into: CRS without nasal polyp (CRSsNP) and CRS with nasal polyp (CRSwNP). 3 Although nasal polyp is the most common mass in the nasal cavity, its etiology and pathogenesis remain obscure. 2 Viruses, bacteria, and fungi together with host and environmental factors with the likelihood of an array of underlying endotypes have all been implicated as a possible etiology. 4
Because eosinophils which are associated with atopic disorders comprise the most predominant inflammatory cells, allergy has been proposed to play a role in the pathogenesis of nasal polyps. However, the result of such association in literature is controversial. 5
The prevalence of allergic conditions has been steadily increasing worldwide. The World Allergy Organization estimates that 30%–40% of the world population is affected by one or more allergic diseases. 6 The role of atopy in CRS is widely debated in literature. The prevalence of allergic rhinitis in CRS varies considerably, ranging from 10% to 84%. 7
Diagnosis of allergic diseases depends on the clinical history and physical examination. Immunoglobulin E (IgE) antibody sensitization is confirmed using either in vivo skin prick test (SPT; puncture/intradermal) or in vitro allergen-specific IgE (sIgE) antibody assay. Both serum sIgE tests and SPT are sensitive and have almost similar diagnostic properties. 8 Williams et al. 9 reported 98% sensitivity and specificity of in vitro tests and they found that SPT and in vitro testing agree well for screening of allergic patients.
The prevalence of asthma in CRS also varies in the literature, ranging from 4% to 44%, whereas, 40% to 75% of asthmatic patients have concurrent CRS. 10 Medical and surgical treatment of CRS in patients with asthma have been shown to decrease both upper and lower respiratory tract symptoms. 5
The objectives of this study are to report the prevalence of inhalant allergy and asthma in medically resistant CRS and to compare this profile between patients with or without nasal polyps.
Methods
After obtaining approval from the Institutional Review Board Committee of King Abdullah University Hospital (IRB number 6/123/2019), charts and medical records of consecutive adult CRS patients who failed to respond to medical treatment (antibiotic, saline irrigation, topical steroid, and/or oral steroid) and scheduled to undergo endoscopic sinus surgery under the authors’ care between July 2011 and May 2019 were retrospectively reviewed. Some of the characteristics of these subjects have been reported in our previous publications.11,12
All subjects were diagnosed according to CRS criteria as defined by internationally recognized consensus statements. 6
The patients were divided into two phenotypes; CRSwNP and CRSsNP, and each phenotype was subdivided according to the presence and absence of asthma. All patients had detailed history, clinical examination, including nasal endoscopy and sinonasal computed tomography (CT) scan. Exclusion criteria included; allergic fungal sinusitis, known cases of food allergy, granulomatous diseases, cystic fibrosis, primary ciliary dysfunction, sinonasal tumors, and pediatric patients.
Charts and electronic records were reviewed for demographic data, presence and absence of nasal polyps, associated asthma, eosinophilia (defined as an increase in peripheral blood eosinophilic leukocytes to more than 500 cells per microliter (μL) of blood), total IgE (tIgE) level, and serum concentration of sIgE to 24 inhaled allergens measured by the enzyme allergo-sorbent test which was performed according to the manufacturer’s protocol (Euroimmun® kits, Medizinische Labordiagnostika, Lubeck, Germany). The results were graded into six classes according to the protocol. Class 1 or more was defined as positive (class 1 is the least positive concentration and class 6 is the highest). Summation of all positive sIgE classes for each patient was calculated.
The tested seasonal allergens were grass pollen, grain pollen, rye, tree pollen, olive, mulb tree, flower mix, and herb, while Dermatophagoides farinae, cockroach, feather mix, cago, pets, mold, penicillium, cladosporium, Alternaria fumigatus, and Alternaria alternata were the tested perennial allergens.
Sample size determination
The sample size was determined using a single population proportion formula based on the following assumptions: 11% prevalence of CRS, 2 95% confidence level, and 5% margin of error. After adding 5% as incomplete or inconsistent data, a sample size of 402 patients was found to be sufficient to show any statistically significant value.
Statistical analysis
Continuous variables are presented as mean ± standard deviation (with interquartile range), or n (%) according to the data distribution. A p value of <0.05 was considered statistically significant. Parametric data were analyzed using the unpaired t-test, while the Mann–Whitney U test was used for nonparametric data analysis. For categorical data analysis; the chi-square test or Fisher’s exact test was used as appropriate. A nonparametric Spearman correlation was used to examine the relation between the total serum IgE level and number of positive inhaled allergens, as well as the correlation between the total serum IgE level and sum of sIgE class.
Results
Four hundred and two patients were included. The average age was 35 years (SD ±3) with 236 males and 166 females. There were no significant differences between CRSwNP and CRSsNP patients based on age, gender distribution, and tIgE level (Tables 1 and 2).
Patient’s demographic features and clinical characteristics.

CRSsNP: chronic rhinosinusitis without nasal polyps; CRSwNP: chronic rhinosinusitis with nasal polyps; IgE: immunoglobulin E.
Patient’s characteristics according to the presence of asthma.

CRSsNP: chronic rhinosinusitis without nasal polyps; CRSwNP: chronic rhinosinusitis with nasal polyps; IgE: immunoglobulin E.
One hundred and fifty patients (61%) in the CRSsNP group and103 patients (66%) in CRSwNP had positive results for at least one tested allergen (p = 0.25), with an overall rate of 63%. The average summation of class level in CRSsNP was 4.4 compared with 4.6 in CRSwNP; this difference was statistically insignificant (p = 0.8; Table 1).
A weak positive non-significant correlation was found between tIgE level and the number of positive allergens as well as between tIgE level and the sum of sIgE class in both groups (Table 1).
The prevalence of asthma in patients with CRSsNP was 9% versus 46% in CRSwNP (p = 0.0001), and the prevalence of high eosinophils was 27% and 47% in both phenotypes, respectively (p = 0.0001; Table 1). We did not find a statistical significance for tIgE level, and positive serology test between both phenotypes according to the presence or absence of asthma, however, for summation of sIgE, statistical significance was seen (Table 2).
The average number of positive allergens in CRSsNP was 2.6 and in CRSwNP was 2.5 (p = 0.8), this difference was insignificant (Table 1). The detailed association after subdividing the phenotypes according to the presence of asthma is shown in Table 3.
Number of positive inhalation stuffs allergens in each group.

CRSsNP: chronic rhinosinusitis without nasal polyps; CRSwNP: chronic rhinosinusitis with nasal polyps; p: p value.
The two subtypes were also comparable according to the highest sIgE class (Figure 1). The number of patients who were reactive to seasonal allergens was 42 (10%; 22 patients (9%) for CRSsNP and 21 patients (13%) for CRSwNP), while for perennial allergens, the number was 86 (21%; 46 patients (19%) for CRSsNP and 40 patients (25%) for CRSwNP), and for both perennial and seasonal ones was 120 patients (30%; 77 patients for CRSsNP and 43 patients for CRSwNP), these differences were statistically insignificant (Figure 2).

Patients display according to the highest enzyme allergo-sorbent test class.

Classification of patients based on type of allergy.
Dermatophagoides farina was the most frequent sensitized allergen in both groups followed by grass pollen, and mold 2 (30%, 20%, and 18%, respectively). For each single tested allergen, there was no significant difference in the percentage of positive inhalation sensitization between the two studied groups (Figure 3).
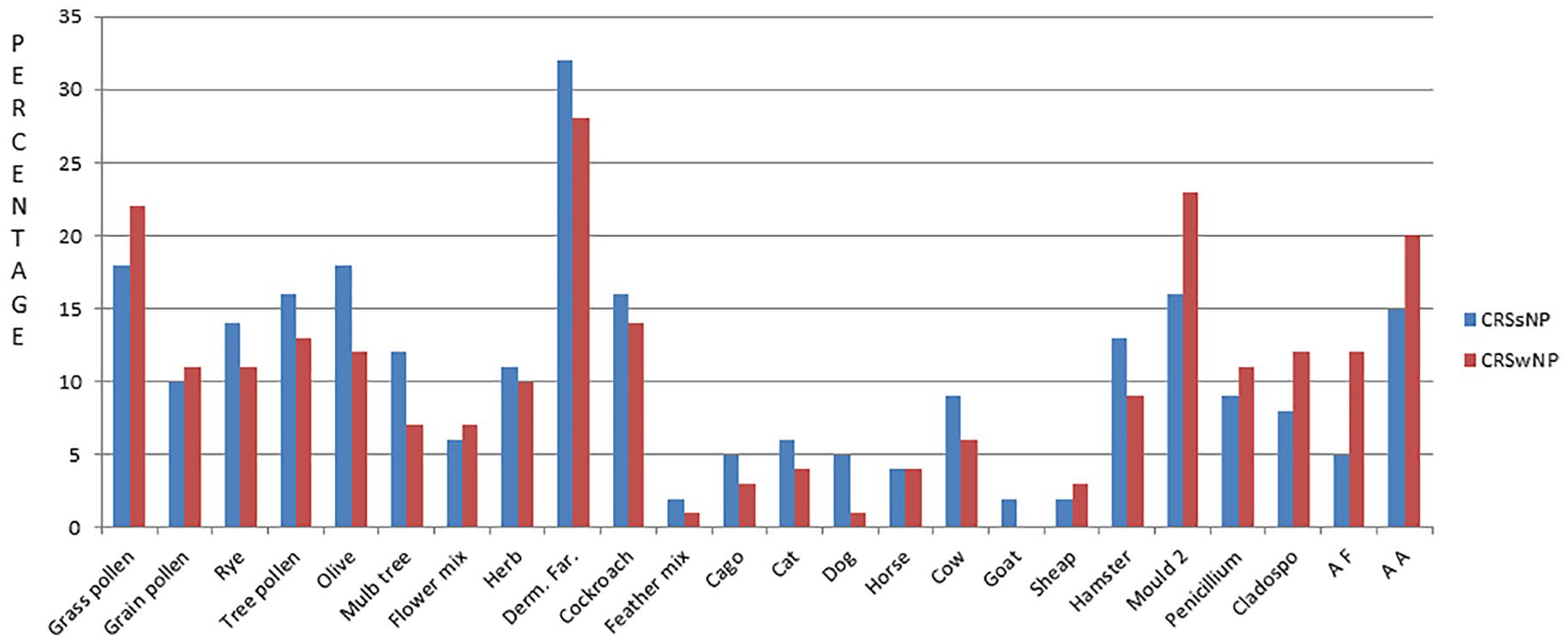
Patient’s sensitivity to each tested allergen.
Discussion
CRS is classified into CRSwNP and CRSsNP. This classification is based on histopathology, immune response, clinical course, and treatment prognosis.2,13 In this study, aeroallergen sensitization was common in refractory CRS; however, we did not find significant differences between severity, frequency, and type of allergy among CRS phenotypes. However, in CRSwNP, the prevalence of asthma and high eosinophils were significantly higher than in CRSsNP.
The heterogeneity of CRS is going far beyond classification into phenotypes to an emphasis on defining CRS endotypes (i.e. subclassifying CRS based on distinct functional or pathobiological mechanisms of disease). 4 CRS and asthma have shown to share biochemical, histological, and clinical characteristics. In Western countries, CRSwNP and asthma share a type 2 inflammatory disease associated with eosinophilic inflammation and edema. The inflammation characterized by elevated levels of IL-4, IL-5, IL-13, IL-17, nitric oxide, and eosinophils, whereas CRSsNP is a neutrophilic, type 1 predominant response inflammation with increased expression of transforming growth factor, interferon gamma and collagen.4,14
Although the contribution of allergy in CRS with or without nasal polyposis has been extensively studied in literature, the association between both common medical conditions continues to be controversial. 13 The majority of studies demonstrated a steady increase in the prevalence of atopy in refractory sinusitis patients. Kennedy 15 found that 57% of 120 patients, undergoing functional endoscopic sinus surgery (FESS) for CRS without differentiating between subtypes, were tested positive for inhalational allergy. In another retrospective study of 200 consecutive patients required FESS for refractory CRS, the authors found 84% of patients had positive allergy tests using a combination of SPT and radio-allergo-sorbent test (RAST) with 58% of patients having multiple allergen sensitivities. 16 In our study, 253 patients (63%) tested positive for at least one aeroallergen and 192 patients (48%) had multiple allergen sensitization.
Our results are consistent with the previous studies directly comparing the frequency of inhalational allergy between CRS patients with or without nasal polyps.2,5,17 Pearlman et al. 5 studied the effect of atopy on the severity of CRS and the presence of nasal polyps. They found the prevalence of CRSwNP to be similar between atopic and non-atopic patients, and reported a weak association between Lund–MacKay score and atopic status. Gelincik et al. 17 evaluated whether history of CRS is more prevalent in patients with allergic rhinitis than in those with non-allergic persistent rhinitis. They concluded that allergic and non-allergic rhinitis may contribute similarly to the development of CRS.
Tan et al. 2 conducted a study to analyze the frequency and distribution of allergen sensitivity in 125 patients failing medical therapy for CRSwNP and CRSsNP. One or more positive skin test results were found in 82% of patients (85.4% in CRSwNP and 79.4% in CRSsNP) with no significant difference between both groups. Also, there were no significant differences in the rates of positive skin test results to any single allergen between both groups. However, the mean number of positive skin tests was insignificantly higher in CRSwNP patients compared with CRSsNP (3.7 vs 2.9). In our study; we did not find a significant difference between both groups for the average number of positive inhalational allergens.
Although FESS has proven to be safe, effective, and efficient management procedure for medically resistant CRS, a subset of patients continues to be symptomatic and often considered as refractory cases. Nasal congestion and postnasal drip are common symptoms in these patients. 1 Our findings of high prevalence of aeroallergen sensitization in medically resistant sinusitis may explain, at least in part, the persistent complaints of these overlapping symptoms after successful sinus surgery. Ramadan and Hinerman 18 found allergy treatment before sinus surgery significantly improved surgical success rate from 64% to 84% after 1-year follow-up.
Dávila et al. 7 conducted a multicenter observational study to evaluate the effect of atopy on the quality of life in nasal polyp patients. The prevalence of atopy was 50% among their patients. A statistically significant difference was observed between the type and severity of associated rhinitis. Persistent moderate or severe rhinitis was more frequent in non-atopic nasal polyp patients, whereas the intensity of nasal polyp symptoms score was significantly higher in atopic patients with nasal polyps and they had worse quality of life.
Some studies found a higher rate of sensitivity to perennial allergens in patients with CRSwNP as compared with healthy individuals and suggested the duration of exposure may play a role in development of nasal polyps. 19 Our study coincides with Tan et al. 2 and failed to demonstrate a significant difference between seasonal or perennial allergy prevalence and CRS subtypes.
The pathogenesis of CRS is still an active research topic. Fungi, the superantigen, the biofilm, and the microbiome hypotheses are environmental factors contributing to CRS. However, these hypotheses are unable to explain the full pattern of CRS. Fungi and bacteria are thus considered disease modifiers rather than the direct cause of CRS. 20
The eicosanoid and the immune barrier hypotheses focus on host factors. The eicosanoid hypothesis did not get widespread of interest with low supported evidence. The hypothesis of mucosal epithelial barrier dysfunction has recently been proposed by many authors. Epithelial barrier dysfunction allows immune system sensitization to multiple allergens. Whether the environmental allergens cause breakdown of the epithelial barrier and predispose to CRS or sinusitis is responsible for enabling allergens penetration is still unclear. Both effects may occur in variable degrees in different patients.2,20
Total serum IgE is a relatively crude method and of limited value for detecting allergic diseases. A high level of tIgE does not necessarily indicate allergy as many other diseases can elevate its level. Normal tIgE does not also exclude allergy because the level may drop between allergen exposure as in seasonal allergy and its level depends on the length of time between exposures. 21 We found a weak non-significant correlation between tIgE and the number of positive aeroallergens as well as between tIgE and summation of sIgE class.
The prevalence of asthma among patients with CRSsNP in this cohort was 19% in CRSsNP and 46% in CRSwNP patients (p = 0.001) which coincide with previously published studies. Stevens et al. 4 found that asthma prevalence was 24% in CRSsNP and 54% in CRSwNP patients who underwent endoscopic sinus surgery. Promsopa et al. 3 reported a 17% prevalence of asthma in a CRSsNP and 48% in a CRSwNP with significant difference between both groups (p = 0.0000). Tan et al. 2 found that asthma was seen in 30% and 63% of CRSsNP and CRSwNP, respectively. Benjamin et al. 1 reported a 36% prevalence of asthma in CRSsNP versus 56% in CRSwNP (p < 0.0001).
The main limitations of this study are its retrospective data analysis with lack of control group and the tertiary academic setting where a highly selective group of patients are being referred, however, this article is the first from our region to report the prevalence and association between nasal polyps, allergy, and CRS.
Conclusion
The prevalence of inhalational allergy in medically resistant CRS is high, however, this profile does not differ based on the presence of polyp. Patients with CRSwNP had a higher prevalence of asthma and blood eosinophils as compared with CRSsNP. Our results showed a little role of inhalant allergens in nasal polyps or asthma comorbidity in refractory sinusitis patients. More studies are needed to further understand the complex relationship between upper and lower airway diseases that will guide to better effective management.
Footnotes
Acknowledgements
The preliminary results were presented in EndoBarcelona 2018 8th World Congress.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Institutional Review Board of Jordan University of Science and Technology (at King Abdullah University Hospital; approval number: 6/123/2019).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was waived by the Institutional Review Board/Ethics Committee because of the study method (retrospective study).