
Abstract
Background:
We developed a technique to preserve the entire nasolacrimal duct and inferior turbinate, by swinging the nasolacrimal duct upward and the inferior turbinate backward; that is, a nasolacrimal duct and inferior turbinate swing technique for sinonasal inverted papilloma of the maxillary sinus. In this study, we evaluated the long-term results of this technique.
Methods:
A retrospective analysis was performed on the data for 53 consecutive pathologically confirmed inverted papilloma patients who were treated using nasolacrimal duct and inferior turbinate swing technique. The frequency of recurrence, the degree of nasolacrimal duct and inferior turbinate preservation, and the frequency of adverse events were assessed.
Results:
The median follow-up period was 51 months (mean 62.5 months; range 10–187 months). No cases of recurrence within the maxillary sinus were observed among the cases treated using this technique, whereas three (5.7%) of the 53 cases experienced recurrence in areas other than the maxillary sinus. We could preserve the nasolacrimal duct in all cases. On the other hand, the inferior turbinate was resected during surgery in one case. No epiphora, dacryocystiits, numbness of the cheek, or collapse of the ala of the nose was observed.
Conclusion:
This nasolacrimal duct and inferior turbinate swing technique method is a safe and effective method for the excision of primary or recurrent inverted papilloma and demonstrates low rates of recurrence and complications.
Keywords
Introduction
Sinonasal inverted papilloma (IP) is one of the most common benign tumors occurring in this region. 1 IP is fundamentally benign in nature but can exhibit locally aggressive behavior, and it is known for its high recurrence rate and concomitant synchronous or metachronous malignant transformations. Therefore, thorough local resection is strongly recommended. 2 In the past, due to the high recurrence rates associated with intranasal surgery, external approaches, including lateral rhinotomy, were considered the gold standard for IP surgery. 1 However, with recent advancements in endoscopic instruments, surgical support tools and the development of endoscopic sinus surgery (ESS) techniques, ESS has shown lower tumor recurrence rates compared to external approaches.3,4 Consequently, ESS has become the gold standard for IP surgery.
Nevertheless, not all cases can be completely excised using ESS alone, particularly when the tumor attachment site extends into regions that are difficult to access via intranasal approaches, such as the frontal sinus, superior orbital fissure, or anterior wall of the maxillary sinus. In cases where intranasal approaches to the anterior wall of the maxillary sinus, for example, are hindered by structures such as the medial wall of the maxillary sinus, the nasolacrimal duct (ND), and the inferior turbinate (IT), a transnasal endoscopic medial maxillectomy (EMM) was developed to allow for the nearly complete resection of maxillary sinus tumors from within the nasal cavity.5–7 However, adverse effects such as epiphora (tearing) and nasal dryness were found to occur after removal of the ND and IT. To address these concerns, several institutions, including ours, have reported methods to preserve the ND and IT during EMM.8–11We developed a technique to preserve the entire ND and IT, and by swinging the ND upward and the IT backward; that is, a ND and IT swing (NDIT-swing) technique. 8
Inverted papilloma is characterized by its slow tumor growth rate due to its benign nature. Consequently, evaluating postoperative recurrence rates requires long-term follow-up. However, as this technique was developed relatively recently, few reports on the long-term results of this technique exist. In this study, we evaluated the long-term results of this technique to assess the associated recurrence rates, adverse events and other pertinent factors.
Materials and methods
Patients
(a) Inclusion criteria
A retrospective analysis was performed on data from patients with pathologically confirmed IP who were treated using the NDIT-swing technique between May 2005 and April 2023 at the Department of Otolaryngology, Head and Neck Surgery, Hokkaido University Hospital, a referral center located in Hokkaido prefecture, Japan.
(b) Exclusion criteria
Patients diagnosed with squamous cell carcinoma at the preoperative pathological examination were excluded from this study.
This study was approved by the Institutional Review Board of Hokkaido University Hospital (No. 023-0263), and the study was performed in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
Indications for NDIT-swing
Tumor attachment to the maxillary sinus that couldn’t be managed with standard EMM without resection of the ND and IT were indications for this technique. In particular, tumor attachment to the anterior, inferior, or lateral wall of the maxillary sinus were good indications for NDIT-swing. Patients in whom the tumor directly invaded to the ND and/or IT were not indicated for this technique.
Selection of surgical procedure by staging
The primary tumor extension sited were classified according to the Krouse staging system with some modifications.12,13 The tumor stage was finally determined from tumor attachment site, which was confirmed during surgery. We preoperatively identified the IP attachment site by computed tomography (CT) and magnetic resonance imaging 14 and chose the surgical procedure in accordance with the tumor attachment site.
For Krouse stage T1 and T2 patients, standard ESS was chosen. T3 diseases were divided into subgroups T3a and T3b; the latter group contained tumors extending into the frontal sinus or supraorbital recess, with the remaining T3 tumors categorized as T3a. T3a patients were treated with ESS or EMM with/without NDIT-swing. An external approach to surgery was considered for the T3b patients as such tumors do not offer easy intranasal access for endoscopic procedures and are frequently observed as sites of recurrence. 15 T4 patients were treated on a case-by-case basis. 12
Surgical procedure
As the most important factor in preventing recurrence in IP is the removal of the origin of the tumor, 16 we employed the “attachment-oriented endoscopic surgical technique” described in a previous study 17 for complete resection of the tumor. The surgical procedure began with tumor debulking using a microdebrider to identify the tumor’s point of origin. The mucosa around the tumor attachment site was safely excised with a free margin. Bone at the tumor attachment site was drilled away.
In cases where the tumor attachment site extended into the maxillary sinus, the NDIT-swing technique was applied. We combined the previously reported ND swing technique 8 with the IT swing method 11 to preserve the functionality of the ND and IT while obtaining a clear visual field and working space. The surgery was primarily conducted endoscopically. An external approach was added when complete excision could not be achieved intranasally.
A comprehensive description of this surgical technique has been provided in previous reports.8,11 In summary, the procedure involved the following steps:
The IT was flipped in the cephalad direction, and the ND opening was identified.
The IT was dissected, leaving the posterior end intact, beginning from the anterior end and passing through the dorsal side.
The IT was swung and flipped toward the nasopharynx.
The mucosa of the frontal process of the maxilla was incised from the level of the base of the middle turbinate to the base of the IT, dissected using Colorado micro-needles and subsequently removed.
The mucosa surrounding the ND opening was also incised.
A dissector was inserted between the frontal process of the maxilla and the lacrimal bone, and the lacrimal bone was detached posteriorly.
The frontal process of maxilla was excised using a Kerrison punch.
The ND was detached from the surrounding bone and swung upwards.
The medial wall of the maxillary sinus was removed.
After completing the treatment within the maxillary sinus, the swung IT was returned to its original position, and the anterior end was sutured with absorbable sutures. The ND, swung upward, was also returned to its original position.
If necessary, we approached from the opposite nasal cavity through the nasal septum. 18 This method can be performed with four hands, so it is useful for cases where the root of the tooth protrudes from the lower wall of the maxillary sinus (Figure 1).

Surgical procedure of the NDIT-swing method. (a and b) The IT was dissected, leaving the posterior end intact. (c) The IT was swung and flipped toward the nasopharynx. (d) The mucosa of the frontal process of maxilla was removed from the level of the base of the middle turbinate to the base of the IT. (e) The mucosa surrounding the ND opening was also incised. (f) The lacrimal bone and the frontal process of maxilla was excised and the ND was swung upward. (h and i) The medial wall of the maxillary sinus was removed, and the tumor in the maxillary sinus was resected. (j) The swung IT was returned to its original position, and the anterior end was sutured.
Assessment of recurrence and adverse effects
The frequency of recurrence, the degree of preservation of the ND and IT, and the frequency of adverse events such as numbness of the cheek and collapse of the ala of the nose were assessed.
Numbness of the cheek was not evaluated for cases in which the Caldwell-Luc (CL) surgery was performed during previous surgery as the symptom existed after the previous surgery.
Statistics
Nonrecurrence rate was calculated for recurrence from disease or the date of the last follow-up for nonrecurrent patients. All parameters were calculated using the Kaplan–Meier method. Statistical analysis was performed using R statistical software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
Fifty-three patients were enrolled in this study. The total number of IP cases operated on at our hospital during the same period was 124, of which 42% underwent this surgical method. Patients consisted of 33 males and 20 females, with a median age of 61years (range 26–86 years). Seven patients (13.2%) were diagnosed with T2, 37 (69.8%) with T3a, 5 (9.4%) with T3b, and 4 (7.5%) with T4 disease. The median follow-up period was 51 months (mean 62.5 months; range, 10–187 months). Of the 53 patients, 34 (64.1%) had previously untreated disease, and 19 (35.8%) had recurrent disease after prior treatment. All 53 patients (100%) had tumors arising in the maxillary sinus. In addition to the maxillary sinus, tumors in 14 (26.4%) patients progressed into the ethmoid sinus, 5 (9.4%) into the frontal sinus and 2 (3.8%) into the sphenoid sinus. Tumors in three patients (5.7%) were confirmed postoperatively as malignant (Table 1).
Baseline characteristics of all study patients.

IP: inverted papilloma.
Surgical procedure
All 53 patients underwent ESS with NDIT-swing. Seven of these patients required additional surgical approaches. Specifically, five patients underwent a trans-antrum (TA) approach, with four of them having previously undergone CL surgery. In these cases, the anterior maxillary sinus bone was missing, and the tumor pedicle was present in the same area, so a TA approach was added. In the one remaining patient, the tumor was located on the inferior wall of the maxillary sinus, and the maxillary sinus was well pneumatized. Therefore, many tooth roots extended into the sinus floor and the tumor was located between the roots. As complete resection of the tumor was considered to be difficult, so we added a TA approach (a canine fossa trephine approach). Finally, the tumor in this case was confirmed malignant on the basis of postoperative histopathological examination.
Additionally, two patients underwent extranasal frontal surgery. As the tumors in these patients were attached on the upper part of the frontal sinus, we chose extranasal frontal surgery.
Recurrence
No cases of recurrence within the maxillary sinus were observed among the cases undergoing this surgical technique, whereas three of the 53 (5.7%) cases experienced recurrence in an area other than the maxillary sinus. The first case had multiple tumors in the bilateral nasal cavities. Although a significant portion of the nasal mucosa was resected during surgery, recurrence occurred outside the resection area within the nasal cavity. In the second case, the tumor extended into the maxillary sinus, ethmoid sinus, and frontal sinus. Despite undergoing ESS and additional tumor excision via extranasal frontal surgery, recurrence was observed on the contralateral anterior ethmoid sinus roof. The last case had tumor extension into the maxillary sinus, anterior ethmoid sinus, and supraorbital recess. ESS was performed to remove the tumor, but recurrence was detected in the supraorbital recess region. In all three cases of recurrence, subsequent surgery successfully removed the tumors using ESS alone. The time elapsed from the repeat surgeries ranged from 3 to 94 months, with all cases demonstrating favorable outcomes without further recurrence (Table 2 and Figure 2).
Characteristics of patients with recurrence.

ESS: endoscopic sinus surgery; NED: no evidence of disease; Mo: month.

Non-recurrence rate.
ND and IT preservation
No case showed direct invasion to the ND so we could assess ND preservation in any cases. On the other hand, direct invasion of the IT mucosa was observed in one patient, and the IT of the patient was resected during surgery. All of the preserved IT remained at the time of the final visit (Figure 3).
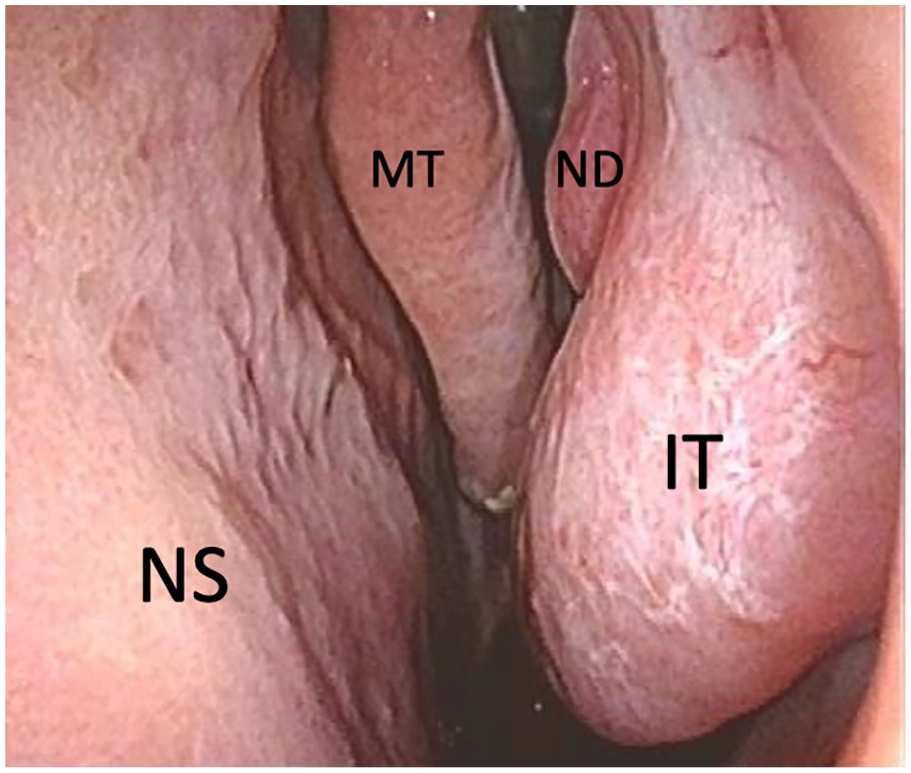
The inferior turbinate at 7 years after surgery.
Adverse events
No cases suffered collapse of the ala of the nose, epiphora, dacryocystiits, or nasal dryness in our study. Further, no numbness of the cheek were observed in patients other than those previously undergoing CL surgery.
Discussion
In this study, patients with IP in the maxillary sinus treated using the NDIT-swing technique were observed for an average of over 5 years, and no recurrence was observed within the maxillary sinus. These results were due to the good field of view that covered the entire maxillary sinus and good working space obtained using this surgical method, allowing us to perform attachment-oriented surgery without hindrance.
The prelacrimal approach (PA) is also a method of performing EMM while preserving the ND and IT. The general PA and NDIT-swing differ in terms of the following 2 points; (1) whether the ND and IT are preserved as one unit or separately, and (2) whether the rim of the piriform foramen is excised. Both methods can secure the field of view and working space while preserving the ND and IT, but the advantages of the NDIT-swing are (1) when approaching from the contralateral side, it does not interfere with access to the ND and IT, and (2) as the rim of the piriform foramen is not incised, collapse of the ala of the nose and sensory disturbance in the cheek area are less likely to occur. In fact, it has been reported that nasal alar deformity occurs in 7.0% and cheek discomfort occurs in 5.6% of patients with a PA, 19 but neither of these adverse events were observed in this study.
On the other hand, the disadvantages of the NDIT-swing are that it requires a more lateral approach than does the PA, which makes it difficult to perform surgery in cases where the maxillary sinus is well-pneumatized and the root of the tooth protrudes from the maxillary sinus floor. 8 The PA is easier than the NDIT-swing to manage in this situation as the rim of the piriform foramen is excised, allowing for a linear approach. Although the NDIT-swing allows a similar approach to the PA by resecting the rim of the piriform foramen, there is a risk of deformation of the nasal alar. Therefore, instead of resecting the pyriform rim, we performed a canine fossa trephine approach 20 in this situation. In this method, a small hole is created in an area where the infra-orbital nerve is unlikely to be damaged, and an instrument is inserted through the small hole. When used in conjunction with the endonasal approach, it becomes easier to treat the intricate areas of the maxillary sinus floor. In this study, we experienced one case in which the canine fossa trephine approach was combined, but the surgery was completed without deformation of the nasal alar or sensory disturbance, and no recurrence was observed.
The recurrent cases that occurred in this study were multifocal cases with the tumor attached in supraorbital recess. In multifocal cases, recurrence often occurs after skipping, and it is difficult to set a safety margin and eliminate recurrence using the concept of attachment-oriented surgery. Additionally, the supraorbital recess is sandwiched between the orbit and the skull base and is deep and narrow, making it difficult to drill. Control of the supraorbital recess is difficult even with external incision. The management of these two situations is regarded as a future challenge.
In cases with previous lateral rhinotomy or CL surgery, the bone in the anterior wall of the maxillary sinus is often missing. In these cases, it is difficult to control the tumor from with intranasal approach because the tumor has directly invaded the connective tissue. In this case, it is necessary to approach the surgery from outside the nose. As endoscopic surgery is currently the gold standard for IP surgery, the number of cases in which the previous surgery included an external incision is expected to decrease.
There are several limitations to the current study. First, this study was not large in scale, so the results of this study might have been affected by the small cohort size. Second, as this study was undertaken at a single institute, the surgeons available to perform this technique were limited, so that future multicenter studies should confirm the usefulness of this technique. Third, the preserved IT may create a blind spot in the maxillary sinus after surgery when rigid endoscopes are used for postoperative monitoring. In contrast, using a flexible fiber scope usually enables monitoring of the entire maxillary sinus after surgery. Fourth, if the tumor invades the ND or IT, resection of these structures will be necessary. Finally, this study is a retrospective observational study and is not a comparative study with other surgical methods. Therefore, the sample size and power analysis were not examined.
Conclusion
This long-term follow-up study demonstrated that the NDIT-swing technique is a safe and effective method for the excision of primary or recurrent IP and it shows low rates of recurrence and complications.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241271877 – Supplemental material for Long-term results of nasolacrimal duct and inferior turbinate swing technique for inverted papilloma of the maxillary sinus
Supplemental material, sj-docx-1-smo-10.1177_20503121241271877 for Long-term results of nasolacrimal duct and inferior turbinate swing technique for inverted papilloma of the maxillary sinus by Yuji Nakamaru, Masanobu Suzuki, Ken Shizuki, Aya Honma, Akira Nakazono, Shogo Kimura, Ryosuke Watanabe, Satoshi Kano, Nayuta Tsushima, Takayoshi Suzuki and Akihiro Homma in SAGE Open Medicine
Footnotes
Acknowledgements
Not applicable.
Author contributions
YN: drafting the manuscript, study concept and design, acquisition and interpretation of data. MS: acquisition and interpretation of data. KS: create illustrations. AH, AN, SK, RW, SK, and NT: acquisition of data. TS: statistical analysis. AH: drafting and finalizing of the manuscript.
Availability of data and material
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Study is supported by the Ministry of Education, Culture, Sports, Science and Technology of Japan (23738243 and 20245309 to Y.N.).
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Hokkaido University Hospital (No. 023-0263).
Consent for publication
Written informed consent for publication was obtained from all individual participants included in the study.
Competing interests
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.