
Abstract
Foreign bodies in the nasal cavity are rarely seen in adults, and most cases are traumatic in origin. Multiple foreign bodies in adults are particularly rare. Foreign bodies induce pain, bleeding, and infection but are easily removed in most cases. A patient presented with multiple toothpick foreign bodies in the nasal cavity, which were introduced intentionally through an oroantral fistula. We report an adult case with 37 toothpicks in the nasal cavity, which were removed successfully with a nasal endoscope. Oroantral fistula closure was achieved through oral surgery. Voluntary insertion of foreign bodies into the body by patients with mental illnesses is relatively difficult to identify. Evaluating and managing the psychiatric problems of such patients during treatment planning are necessary.
Introduction
Although there have been numerous otolaryngological reports of foreign body insertion, foreign bodies in the nasal cavity and paranasal sinus are rarely seen in adults. Prolonged retention of foreign bodies in the nasal cavity and paranasal sinus may cause symptoms such as nasal stuffiness, nasal discharge, and hyposmia, as well as inducing orbital complications among other types, such as encephalomeningitis through the base of the skull. 1
A variety of foreign bodies have been reported in the nasal cavity and paranasal sinus, including pencils, wooden chips, plastic, metal sticks, and bullets; these foreign bodies can lead to various symptoms and complications may arise from toxicity.2,3 We report a case of sinusitis induced by voluntary insertion of 37 wooden toothpicks into the nasal and paranasal sinus via an oroantral fistula in a patient with mental illness. We removed the foreign bodies and treated the sinusitis without complications.
Case history
A 41-year-old female patient habitually suffered from nasal stuffiness, hyposmia, and hypogeusia. She presented to our hospital due to progressive worsening of nasal stuffiness, starting 1 month earlier. She had a history of surgery, chemotherapy, and radiation therapy for breast cancer (3 years earlier).
Nasal endoscopy performed at the initial examination showed a narrowed natural ostium of the right maxillary sinus and a polyp-shaped mass in the left sinus. The patient was confirmed to have anosmia (Korean version of the Sniffin’ Sticks Test (KVSS-II) score of 10.5 (anosmia range 10.69 ± 3.37), 4 positive in ammonia test). Paranasal sinus computed tomography (CT) revealed multiple straight hairlines spanning the base of the bilateral maxillary sinuses and anterior ethmoidal sinus (Figure 1). The radiologist mentioned that irregular lines were visible in both maxillary sinuses and oroantral fistulas. At the initial examination, bilateral endoscopic sinus surgery was performed due to a suspicion of bilateral chronic sinusitis or fungal sinusitis accompanied by bilateral oroantral fistula.

Coronal computed tomography images show multiple straight-air lines running from the base of the maxillary sinus to the roof of the ethmoid sinuses of both nasal cavities ((a) non-enhanced image and (b) enhanced image).
Surgery was performed under general anesthesia. After uncinectomy and middle meatal antrostomy, multiple foreign bodies that penetrated through the maxillary sinus walls over the ethmoid sinus were found on both sides (Figure 2). Eight foreign bodies on the right side and 29 on the left side were removed through the nasal cavity (Figure 2), and ethmoidectomy and sphenoidotomy were performed to conclude the surgery.
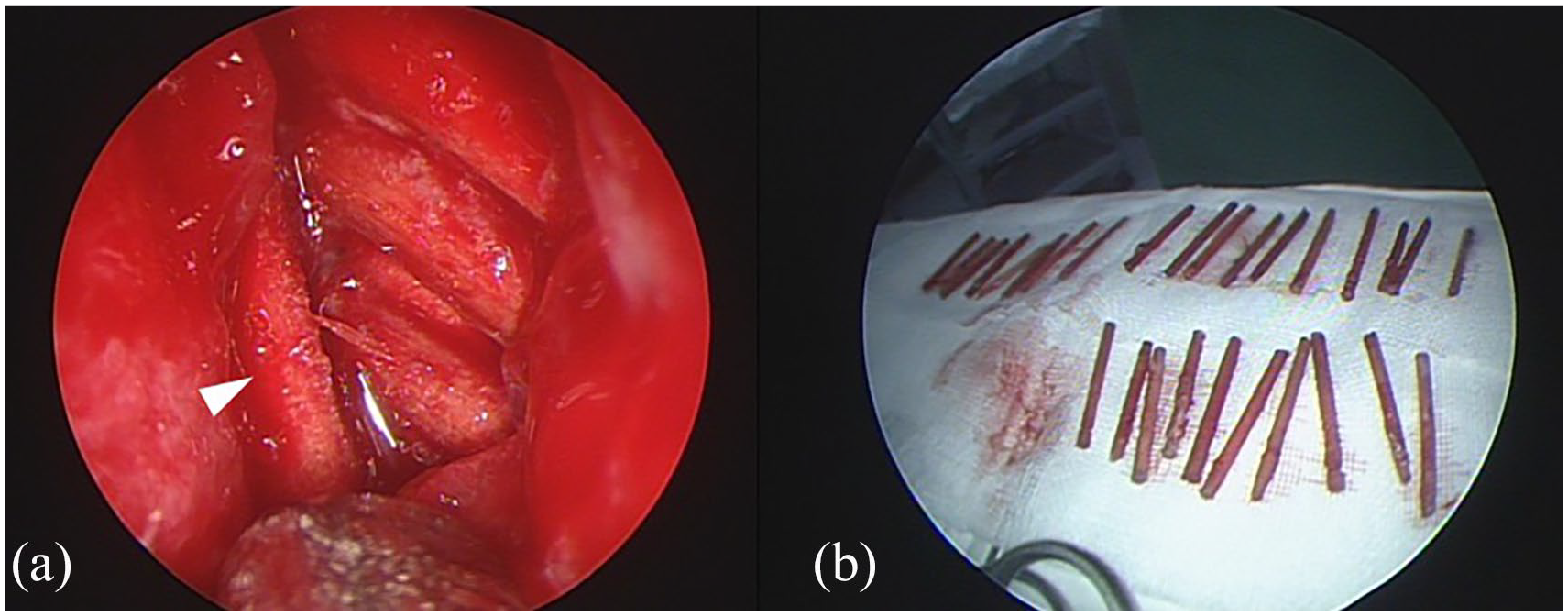
(a) Intraoperative nasal endoscopy view. Multiple wooden toothpicks were seen in the middle meatus of both nasal cavities (white triangle). (b) Eight toothpicks were removed from the right side and 27 from the left side. All foreign bodies were removed by the endoscopic endonasal route.
After the surgery, we suspected that the patient had voluntarily inserted the foreign bodies and referred her to the psychiatry department, which later reported that the patient derives pleasure from trimming toothpicks to a specific size and placing them into her nose. She said after molars fell out, she kept putting a toothpick in that place. However, further diagnostic evaluation was not performed because the patient refused. Inferior meatus fillers were removed on postoperative day (POD) 2, and the patient was discharged on POD 3. Middle meatus fillers were removed on POD 7 at the outpatient follow-up, but new toothpick foreign bodies were found over the left maxillary sinus and ethmoid sinus; these were removed. The patient stated that she inserted them after being discharged from hospital. At the 2-week follow-up, we again discovered foreign bodies inside the nasal cavity. The patient was scheduled for foreign body removal and correction of the oroantral fistula but was lost to follow-up for 2 years and 6 months. She again presented to the outpatient clinic after symptoms recurred and stated that she inserted more foreign bodies during this period. Four foreign bodies on the right side and 11 on the left side were removed through endoscopic sinus surgery under general anesthesia, and oroantral fistula closure was performed using the buccal flap for the left fistula and the palatal flap for the right fistula (Figure 3). She is currently being followed-up as an outpatient and has no symptoms.

Preoperative oroantral fistula ((a) left and (b) right) (white arrow). (c) The left oroantral fistula was closed with a buccal flap. (d) The right oroantral fistula was closed with a palatal flap.
Discussion
In a patient suspected of having foreign bodies in the nasal cavity and paranasal sinuses, the presence of foreign bodies can easily be confirmed based on detailed history taking and nasal endoscopy during the initial examination. The type and timing of symptoms may vary depending on the type of foreign body involved. In cases with early onset symptoms, the patient may present to the hospital early and receive rapid diagnosis and treatment. With a later onset of symptoms, the patient may be unaware of their condition and might be diagnosed incidentally. Furthermore, when patients lose consciousness, have a drug addiction or mental illness, or are unaware of their condition, a lack of symptoms suggesting foreign bodies may significantly delay their detection. In the present case, the patient voluntarily inserted foreign bodies through an oroantral fistula and presented to the hospital due to the resulting paranasal sinusitis symptoms. We could not initially diagnose the patient with foreign bodies in the nasal cavity and paranasal sinuses, because this was a case in which foreign bodies would not be suspected even with detailed history taking unless the patient complained of the symptoms thereof.
When a foreign body in the nasal cavity or paranasal sinuses is suspected, the possibility of multiple foreign bodies should be considered. The first test that should be performed is a simple X-ray; CT or magnetic resonance imaging (MRI) may also be useful for a more accurate diagnosis. Simple X-ray is only useful for detecting metallic foreign bodies, while ultrasound cannot distinguish between fat and foreign bodies, and also requires proficiency to perform the test and interpret the results. Paranasal sinus CT is the most useful imaging modality for the diagnosis and treatment of nasal cavity and paranasal sinus diseases, as it can reveal injuries to the paranasal sinuses, the positional relationships among major muscles, bones, and soft tissues, and the shape and features of the foreign body. Although it is challenging to identify organic, glass, and plastic foreign bodies, which show similar shades to the surrounding tissues, wooden foreign bodies, as seen in our case, can be detected by examining the patterns in multiple paranasal sinus CT scans acquired over a short period. 5
When removing foreign bodies from the nasal cavity and paranasal sinuses, their locations must first be identified through detailed evaluation, physical tests, and radiological investigations, followed by surgery that avoids injuring healthy nasal cavity, adjacent orbital tissue and the base of the skull as far as possible. In the present case, we had initially planned an endoscopic paranasal sinus surgery following diagnosis of chronic paranasal sinusitis and an intranasal mass. Uncinectomy and middle meatal antrostomy were performed, through which foreign bodies were discovered and removed through the nasal cavity. The consequent paranasal sinusitis was then treated with ethmoidectomy and sphenoidotomy, and the fistulas were closed using buccal and palatal flaps.
The patient in this case was found to have a peach allergy during preoperative testing, and we confirmed sensitization to peach antigen, but with no sensitization to other antigens, in the Multiple Allergen Screening Test (MAST). The wooden toothpicks used throughout Korea are made of birch trees; the major antigen for birch trees is Bet v1, which is associated with birch-apple syndrome. 6 Birch pollen is found in peaches, and Pru p1, 3, and 4 have been reported to be involved. Therefore, we suspected that the patient developed a peach allergy as a result of a cross reaction with birch tree antigen due to prolonged retention of the toothpicks. The patient also stated that she developed a peach allergy after inserting the toothpicks, which suggests the possibility of an oral allergy syndrome. Opinions vary regarding the best treatment for an oroantral fistula. Because paranasal sinusitis occurs in 50% and 90% of cases within 48 h and 2 weeks of fistula formation, respectively, some researchers state that surgical treatment is essential within 24 h of fistula formation. It has also been argued that, in cases in which the fistula is small (~2 mm) and not accompanied by paranasal sinusitis, drug therapy for at least 3 weeks should be the first-line therapy, as the fistula may close with early drug therapy. It is known that closing a fistula is difficult with drug therapy beginning more than 3 weeks after onset or in the presence of maxillary sinusitis. However, given that antibiotic treatment alone can sometimes close the fistula in such cases, antibiotic therapy may be beneficial as a first-line treatment for small fistulas, even more than 3 weeks after onset or in the presence of maxillary sinusitis. When antibiotic treatment alone is ineffective, reconstruction using only buccal and palatal flaps, or using soft tissue and osteo-flaps, are other options. The former technique has a success rate of about 70%–80%, while the latter method has been reported to be associated with a low rate or absence of recurrence.
In this patient, we suspected mental illness based on her statement that she feels pleasure after inserting trimmed wooden toothpicks into the maxillary sinuses and nasal cavity through an oroantral fistula. Andereggen et al. 7 reported a paranoid schizophrenic patient who voluntarily inserted a foreign body into the cranial cavity, and Alsarraf and Bailet 8 reported a patient who intentionally placed a foreign body into the sphenoidal sinus. Thus, voluntary insertion of foreign bodies into the body is relatively common among patients with mental illnesses, so evaluating and managing their psychiatric problems during treatment planning is necessary to prevent recurrence. We recommended that the patient in this case and her caregiver seek a psychiatric consultation, during which treatment was advised based on the high likelihood of schizophrenia suggested by the screening test; however, the patient refused. In the future, concurrent management of psychiatric problems should be provided to improve treatment outcomes and long-term prognosis. After the second surgery, she was referred to the psychiatrist again for treatment.
Conclusion
Along with a review of relevant literature, we presented a patient suspected of mental illness with paranasal sinusitis induced by voluntary insertion of wooden toothpicks into an oroantral fistula. A good treatment outcome was attained by removing the foreign bodies through endoscopic sinus surgery and closing the fistula with palatal and buccal mucosa.
Footnotes
Author’s Note
Young Joon Jun is now affiliated with Department of Otorhinolaryngology-Head and Neck Surgery, Eulji University College of Medicine, Uijeongbu-si, Gyeonggi-do, South Korea.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SoonChunHyang University Research Fund.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article. Informed consent was received from the patient. The patient had decisional capacity to provide consent.