
Abstract
Schizophrenia is one of the most troublesome psychiatric problems requiring long-term antipsychotic treatments. There is a scarcity of data regarding its overtime trend in Ethiopia.
Objective:
To explore the 5-year trend of schizophrenia at Hiwot Fana Specialized University Referral Hospital, Eastern Ethiopia.
Methods:
A hospital-based retrospective record review was conducted at Hiwot Fana Specialized University Referral Hospital, Eastern Ethiopia. Data were obtained from medical records of all registered psychiatric patients in the psychiatric follow-up clinic over 5 years from 2016 to 2020. An Extended Mantel-Haenszel chi-square test for the linear trend was used to examine the trend over the 5-year period.
Results:
Over the 5-year period stated (2016–2020), a total of 29,184 psychiatric patients were registered at the Hospital from which 18,598 (63.73 % (95% confidence interval: 0.63–0.64) were schizophrenia confirmed cases. Of the 18,598 patients, 15,362 (82.60%) were males and 7,625 (41%) were in 25–34 years of age category. It was revealed that the trend of newly diagnosed patients with schizophrenia increased from (0.44 (95% CI (0.39–0.47) in 2016 to 0.47(95% confidence interval: (0.44–0.49) in 2020 (χ2 = 3.87; p = 0.049). Those chewing Khat were disproportionately affected accounting for about half of the schizophrenia total cases reported.
Conclusion:
The magnitude of patients with schizophrenia being treated at the hospital increased over the 5 years studied. Tailored preventive and treatment interventions are needed to mitigate the problem. Community and institution-based customized interventions can be designed using the existing health system platforms.
Introduction
Schizophrenia is one of the most challenging psychiatric conditions, 1 characterized by hallucinations, incoherent speech, delusions, disorganized or unusual behavior.2,3 The disease affects more than 24 million people around the world.4,5 The problem was predicted to have a yearly incidence of 15.2 per 100,000 people and a lifetime occurrence of 0.5%–1%.6,7 According to the most recent epidemiological data, the overall lifetime prevalence of schizophrenia was 5.44 per 100,000 people, 8 contributing to the disease burden and resulting in chronicity and disability. 8 In terms of disability and mortality, mental illness is the major non-communicable disease in Ethiopia, 9 accounting for 11% of the total burden of disease, with schizophrenia and depression ranking in the top 10.10,11
Schizophrenia causes significant disability, accounting for approximately 1.1% of total disability-adjusted life years, and 2.8% of years lived with disability, 12 with 60% of people suffering from moderate to severe disabilities. 13 The disease typically manifests between the ages of 18 and 35 years, peaking in late adolescence or early adulthood. 14 It requires long-term treatment and has a significant effect on the quality of life for patients and their respective families. 15 It is the most stigmatized mental illness and has a significant, detrimental influence on people’s physical, social, economic, and health by disrupting personal and social relationships as well as financial stability, mostly affecting patients and their families.14,16
The onset of schizophrenia is influenced by a variety of factors, but genetic and psychosocial-environmental factors play the largest roles. 15 Biologically related people are more at risk of developing schizophrenia than unrelated people. 17 If both mother and father have schizophrenia, their children are 40% more likely to have it; dizygotic twins are 10% more likely; and monozygotic twins are 40%–50% more likely. 1 Some studies have been conducted in various parts of the world on the epidemiology of schizophrenia, according to one available Korean study finding, the prevalence rate of schizophrenia spectrum disorders was 0.61% over 5 years and 0.7% over 10 years. 18 Mental illness, especially schizophrenia, is a significant healthcare issue in many African nations. 19 There is a lack of access to evidence-based treatment options in Africa and other low- and middle-income countries, including Ethiopia.20,21 This is due to a lack of resources, such as psychiatric professionals and facilities, as well as persistent underinvestment. 21
About 4 to 5 million Africans experience difficulties with severe mental illnesses like schizophrenia. 22 Patients with schizophrenia have limited access to modern healthcare facilities in countries like Ethiopia, 23 where the healthcare infrastructure is underdeveloped. 22 For example, 90% of Ethiopians who had schizophrenia and other severe mental illnesses did not receive modern mental health services. 24 According to studies from some Sub-Saharan African countries, for instance, only about 21% of people with serious mental disorders like schizophrenia received any kind of modern treatment in Nigeria over the course of 1 year, and only 26% did so in South Africa.25,26 Similarly, only 10% of them in Ethiopia had access to modern psychiatric services. 27
Furthermore, studies have found that there is a widespread belief in Ethiopia 27 that people with schizophrenia are under the control of monsters, possessed by evil spirits, cursed by ancestral spirits, or the result of evil eyes. 28 As a result, those who are affected and/or their families frequently seek help from religious and traditional healers rather than from healthcare facilities.29,30 For example, the vast majority of Ethiopians find it extremely difficult, expensive, and rare to access contemporary mental health services.28,31 Patients typically wait until they have tried and failed to feel better using more traditional methods before seeking out modern mental health services, despite the fact that their mental health issues are frequently not recognized. 28 In addition, it is a typical practice in Ethiopia that family members frequently assist and care for people with schizophrenia and other severe mental illnesses at home. 32 Despite the fact that the problem has been found to be widespread in various parts of the world, 27 only a few epidemiological studies of schizophrenia have been conducted. 33 Given the distinctive sociocultural characteristics of this part of Ethiopia, there is little evidence in Ethiopia in general and Eastern Ethiopia in particular that emphasizes the significance of having data on this challenging disease in this area. Hence, our hypothesis was to see whether the trend of schizophrenia was supposed to be constant in time or not. Therefore, the purpose of this study was to explore the trend of schizophrenia at Hiwot Fana Specialized University Referral Hospital, Eastern Ethiopia.
Methods
Study area and period
The study was conducted from 1 June to 31 July 2021, at Hiwot Fana Specialized University Referral Hospital located in Harar Town, eastern Ethiopia. Harar is the capital city of Harari Regional State. The region is located in eastern Ethiopia, at a distance of 526 km from Addis Ababa (the capital city of Ethiopia). There are two public hospitals in the Harari Region (Hiwot Fana Specialized University Referral Hospital and Jogul Regional Referral Hospital). Hiwot Fana Specialized University Referral Hospital was established in 1941 and became a university specialized hospital in 2010. The hospital provides service to more than 154,196 patients yearly with various general and specialized clinics, including psychiatric services. The psychiatric unit includes 12 inpatient beds, of which 7 are reserved for male patients and 4 are for female patients. One bed is reserved for a neuropsychiatric patient, and there are three outpatient rooms with one psychiatrist. There are five first-degree psychiatric nurses and three clinical and community mental health practitioners with master’s degrees.
Study population and sample size
A total of 18,598 medical records on schizophrenia cases registered from 2016 to 2020 were included in this study.
Inclusion and exclusion criteria
The source population consisted of all psychiatric patients whose record was available from 2016 to 2020 in the psychiatric clinic, while the study population comprised only patients with schizophrenia whose records were complete and available from 2016 to 2020.
Exclusion criteria
Our study did not include any records available before 2016 and records which are unclear or incomplete (records which not clearly state the patient’s diagnosis, year of first diagnosis, age, sex, residence marital status educational status, occupation and substance use).
Study design
This study was a hospital-based retrospective record review of patients registered at the psychiatric follow-up clinic of the hospital from 2016 to 2020.
Study variables and measurements
The outcome variable was the magnitude of schizophrenia cases and 5-year time duration, sociodemographic characteristics (age, sex, marital status, residence and education) and behavior related to substance use (Khat, cigarette, and alcohol).
Schizophrenia was diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnostic criteria. 14
Data collection procedure and quality control
A uniform data abstraction checklist was prepared to gather relevant data from the medical records. The checklist has questions like the sociodemographic characteristics (age, sex, marital status, and education), diagnosis of the participant, including time of diagnosis, which was derived from the DSM-IV criteria (hallucinations, delusions, disorganized speech or behavior, catatonic, negative symptoms, and impaired functional activities with continuous signs of the disturbance persisted for 6 months). A structured questionnaire was used to assess the type of substance use (including khat, cigarette, and alcohol; if recorded in the chart, it was taken as substance use was present). Ten BSC nurses were assigned as data collection, four masters’ degree holders in clinical and community mental health supervised the data collection process, and data were extracted by reviewing follow-up charts and cards of patients. A 3-day training was given for the data collectors and supervisor on the objective of the study and how to review the documents as per the data extraction checklist. The pretest was conducted on 372 (2%) of patients with schizophrenia from Jogul Hospital located in the same setting. The results were used for the correction of the questionnaires. The principal investigator supervised the data collectors closely. Adequacy of the checklist was evaluated and ambiguous questions were improved before the actual data collection. Besides, daily monitoring of data for completeness and consistency was made.
Statistical analysis
Data were entered using Epi-data 3.1 and exported to STATA 14 for further analysis. Descriptive statistics were conducted using frequency and percentages for categorical measurements and mean and median were used to summarize continuous variables. Time (measured in years) was the main outcome of interest since it allowed for the estimation of changes in the status of schizophrenia over time and the estimation of the disease’s prevalence. The relationship between the observed and the anticipated trends of schizophrenia in each year was ascertained using descriptive statistics and a chi-square test technique with a confidence interval of 95% confidence level. The extended Mantel-Haenszel chi-square test was examined for a linear trend to look at trends in the proportion of patients with schizophrenia from 2016 to 2020. Participants’ age, gender, place of residence, and Khat chewing experiences were used to describe the outcome variable distribution.
Ethical considerations
Prior to data collection, the study protocol was approved by the Institutional Research Ethic Review Committee (IHRERC) of the Colleges of Health and Medical Science, Haramaya University (Ref. No. IHRERC/255/2020). In addition, the hospital’s administrative bodies issued a formal letter of permission to the relevant psychiatric department. Besides that, all details were kept private. Patients’ names were left out in favor of their card numbers, further ensuring the confidentiality of their personal data. This study was conducted following the Declaration of Helsinki.
Results
A retrospective study was carried out on 29,184 patients with psychiatric problems, of whom 18,598 (63.73%, 95% CI (0.63–0.64)) had schizophrenia and were registered at Hiwot Fana Specialized University Referral Hospital between 2016 and 2020. The mean (+SD) age of patients with schizophrenia was 31.4 (+10.5), ranging from 11 to 75 years of age. Among patients with schizophrenia, 27 (0.15%) were under the age categories of <15 years, 4571 (24.58%) 15–24 years, 7625(41.0%) between the age of 25 and 34 years, 4078 (21.93%) at the age category of 35–44 years of age, and 2297(12.35%) of them were over the age of 45 years. More than half (56.17%) of them were from urban areas; 3741 of them (26.42%) were unemployed), while out of 4595 newly diagnosed patients with psychiatric illness, 2059 (44.81%) of them were newly diagnosed as patients with schizophrenia (Table 1).
Socio-demographic characteristic of patients with schizophrenia at Hiwot Fana specialized university Hospital Eastern Ethiopia (2016 to 2020).

other: daily labor; house wife.
Trend of schizophrenia
The trend of patients with schizophrenia among all patients seen in psychiatric clinics has increased from 2732 (57%) patients in 2016 to 5079 (65%) patients in 2020. The findings revealed a significant difference in the number of patients with schizophrenia each year. This means that the trends of schizophrenia patients show a decrease one year and an increase the next. For example, there was a decrease in the number of patients with schizophrenia in 2016, which was followed by an increase in 2017, a slight decrease in 2018, and an increase from 2019 to 2020. In general, the chi-square test result indicates that the trend of schizophrenia is increasing (Figure 1).

Overall Trend of schizophrenia at Hiwot Fana Specialized University Hospital, Eastern Ethiopia, a 5 Years’ retrospective Analysis (2016 to 2020) from 1 June to 31 July 2021.
Trend of newly diagnosed patients with schizophrenia
There was an increasing trend in newly diagnosed patients with schizophrenia during the specified period 182 in 2016 to 616 in 2020 in the study area with a slope of 104 on a linear scale, and there is statistical significance for the decline of newly diagnosed schizophrenia (Figure 2).

Trends of newly diagnosed schizophrenia at Hiwot Fana Specialized University Hospital, Eastern Ethiopia, a 5 Years’ retrospective Analysis (2016 to 2020) from 1 June to 31 July 2021.
The proportion of newly diagnosed schizophrenia among all clients visiting psychiatric outpatients has increased from 0.44 (95% CI (0.39–0.47)) in 2016 to 0.47 (95% CI (0.44–0.49)) in 2020 (Table 2).
Baseline proportion of newly diagnosed patients with schizophrenia at Hiwot Fana Specialized University Hospital, Eastern Ethiopia (2016–2020).

χ2: Chi-square; OR: Odds Ratio.
The trends of schizophrenia at baseline were statistically significant with a Mantel-Haenszel χ2 = 9.67 (p = 0.0018) and that the overall number of new and repeated patients with schizophrenia who visited the hospital over the 5 years was varied throughout the 5-year observations (Table 3).
Trends of schizophrenia at Hiwot Fana Specialized University Hospital, Eastern Ethiopia (2016 to 2020).
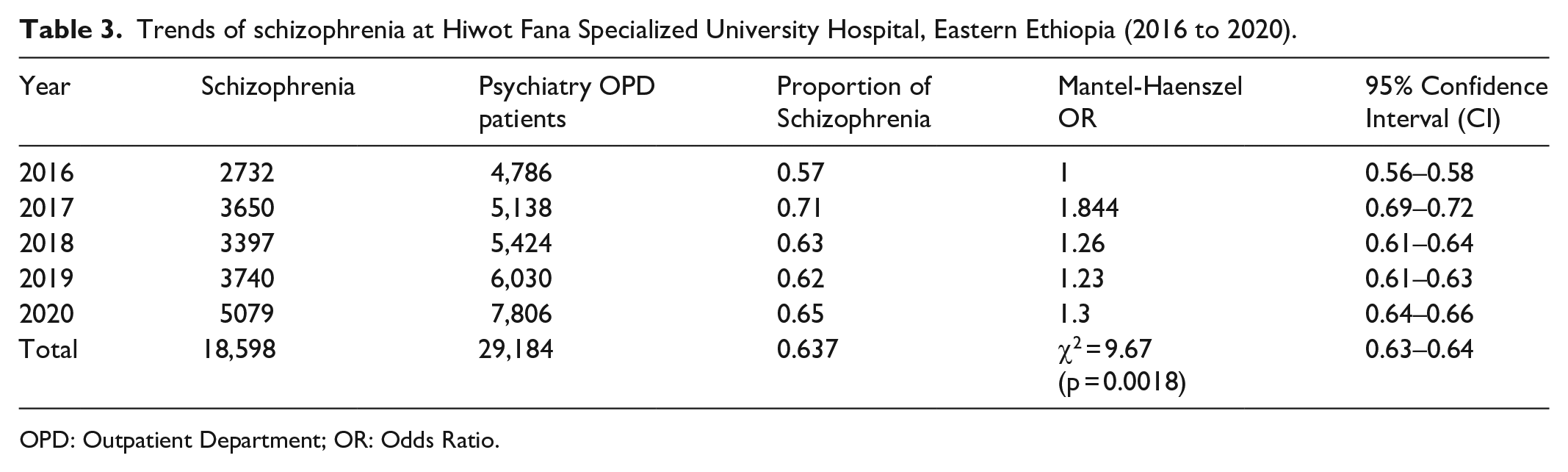
OPD: Outpatient Department; OR: Odds Ratio.
The overall proportion of patients with mental illness at the baseline (Extended Mantel-Haenszel chi-square) and the proportion of newly diagnosed patients with mental illness increased from 0.087 (2016) to 0.169 (2020). The proportion of reaped case increased significantly in 2016, then decreased from 2017 to 2019, and then increased slightly in 2020. Contrarily, the proportion of newly diagnosed patients decreased in 2016, increased from 2017 to 2019, and then decreased slightly in 2020 (Table 4).
Newly diagnosed patients with mental illness at baseline (Extended Mantel-Haenszel chi-square and proportion) at Hiwot Fana Specialized University Hospital, Eastern Ethiopia (2016 to 2020).
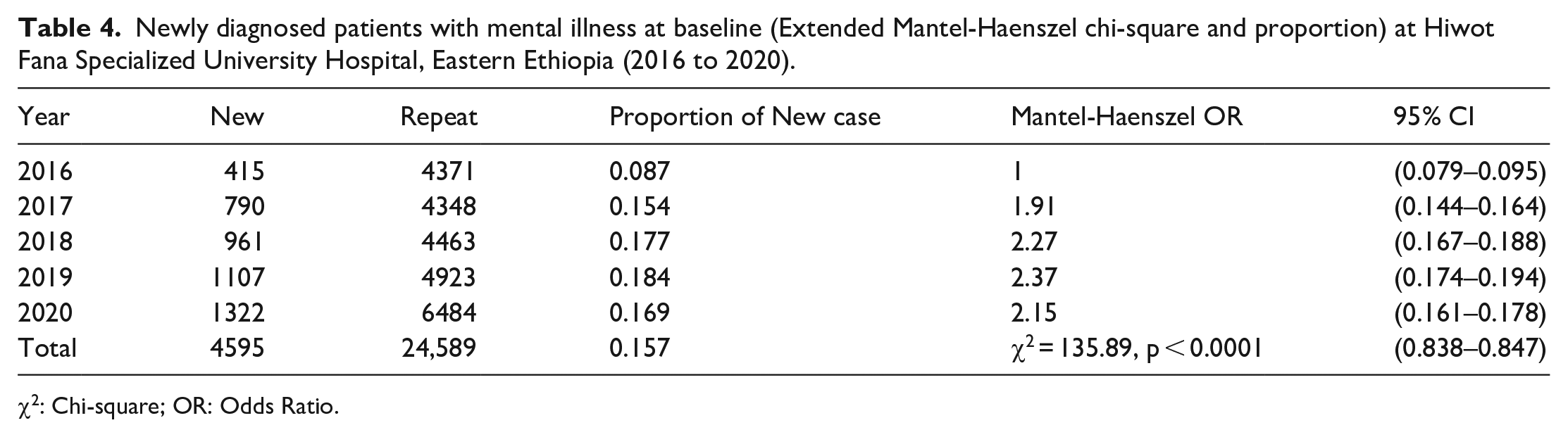
χ2: Chi-square; OR: Odds Ratio.
Age- and sex-related schizophrenia
Male patients with schizophrenia increased from 2289 (59.07%) in 2016 to 4176 (69.21%) in 2020. Of the 18,598 patients, 15,362 males with schizophrenia were between the ages of 25 and 34 years, while 1012 (31.27%) of the females with schizophrenia were between the ages of 25 and 34 years (Figure 3).
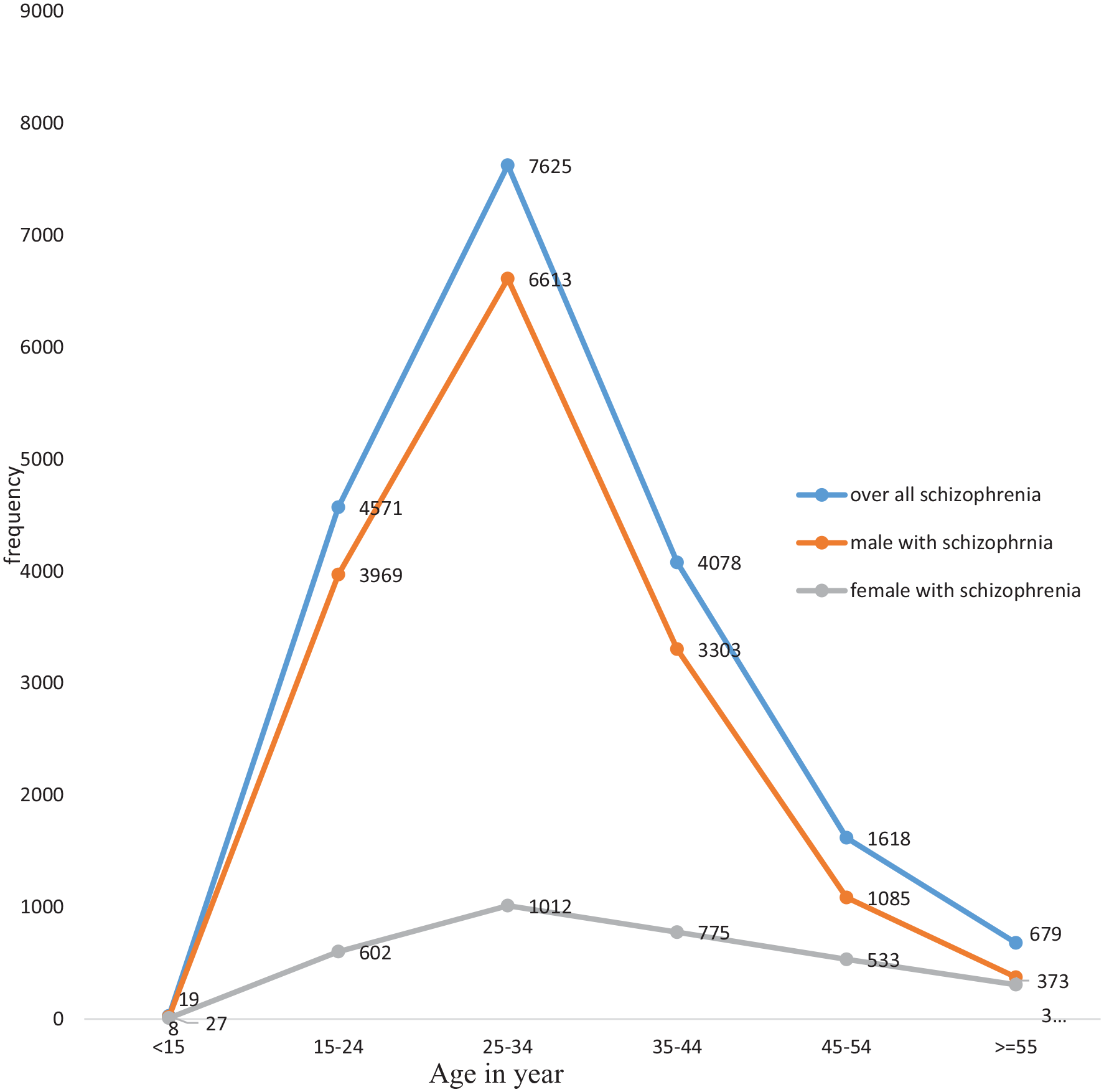
Trend of schizophrenia in different age groups and genders of participants at Hiwot Fana specialized University Hospital in Eastern Ethiopia: a five-year retrospective analysis (2016 to 2020) from June 1 to July 31, 2021.
Schizophrenia and substance use
Substance abuse is common among patients with schizophrenia. As a result, 7843 (42.18%) of schizophrenia patients chewed Khat, 1709 (9.19%) mixed it with cigarettes, and 1025 (5.51%) used more than two psychoactive substances (poly substance users). Generally, the number of patients with schizophrenia who use substances increased significantly from 2016 to 2020; for example, 112 in 2016, 2267 in 2017, 1599 in 2018, 1837 in 2019, and 2028 in 2020, whereas the number of polysubstance users fluctuated. For example, there was a high record in 2016, decrements in 2017, and then an increase from 2018 to 2020 (Figure 4).

substance use among patients with schizophrenia at Hiwot Fana specialized university hospital in Eastern Ethiopia, a five-year retrospective analysis (2016 to 2020) from June 1 to July 31, 2021.
Discussion
Our findings show that the percentage of patients with schizophrenia has increased significantly over the last 5 years of observation (2016 to 2020). Each year, the number of patients with schizophrenia fluctuates significantly, with a decrease 1 year and an increase the next. Schizophrenia was more prevalent among men, those in productive age groups, urban dwellers, and Khat users.
Out of all clients who visit the psychiatry department, the percentage of patients diagnosed with schizophrenia increased from 57% to 65% between 2016 and 2020. Our findings were in agreement with other studies from Malaga (Spain) and elsewhere.34,35 However, our study prevalence was higher than other studies from Madonna University Teaching Hospital in Pakistan and Saudi Arabia.36-38 In addition, our findings were lower than the 10-year trends reported in China and the Democratic Republic of Korea.39,40 The characteristics of the study participants, study designs, socioeconomic status, cultural context, study setting, methodology, and diagnostic tools employed and sample size may all contribute to the differences between studies that have been observed. In addition, this might be connected to the rising psychoactive substance use in the eastern Ethiopian community.
We found that schizophrenia is more common in men than in women. Our findings are consistent with those of other studies from Malaga (Spain),32,33 but different from other studies by Perälä et al. 41 that found no gender difference. The discrepancy may be explained by the fact that men use psychoactive substances more frequently than women, which may raise their risk of developing schizophrenia.34,42 In every age group, gender differences were seen, and our results are consistent with earlier studies showing that schizophrenia manifests at different ages in men and women, with men experiencing the disease younger than women.15,43 The fact that men in the study area use substances like Khat and cigarettes more frequently than women may contribute to the disparities, aggravating the situation among men. Another reason may be that female patients cannot access mental health care because they depend financially on their husbands, fathers, and brothers.44,45
Our findings imply that productive age groups had a higher percentage of schizophrenia. These results contradict other studies from Korea, 40 but are in agreement with earlier studies from Spain and other areas of Ethiopia.35,46 This may be due to the social circumstances in which this group lives, which encourage and amplify the stress brought on by their financial situation and increase substance misuse. 47 Our findings suggest that the prevalence of schizophrenia is higher in urban areas than in rural areas, which is consistent with an earlier study from Spain that showed similar rates in urban populations. 35 However, our findings contradict a systematic review. 48 Possible reasons for higher rates might be that urban areas are likely to be connected to contemporary urban lifestyles, the growth of urban areas, and a potential difference in the degree of symptom awareness between rural and urban areas. Or urban living has more social and professional demands than rural living, emphasizing the limitations and social dysfunction of people with schizophrenia in these areas. In addition, social support and attitudes toward psychiatric conditions, including schizophrenia, may be more harmful in rural areas, leading to a higher percentage of people with schizophrenia going unreported or deterred from accessing treatment. 40 In our study area, psychiatric treatment services are found in most urban areas; therefore, mental health services are easily accessible in nearby health facilities, including comprehensive awareness creation services.
We found that those who were jobless, unmarried (single), and divorced had a higher risk of schizophrenia, which matches earlier studies by Kebede and Alem (1999). This might be due to social isolation, placing an additional burden on economic and emotional well-being, leading to increased stress. 49
According to this study, most people with schizophrenia use psychoactive substances, with 50.91% reporting a history of Khat chewing at some point in their lives. Our findings are higher than the study conducted by Ayano and his colleagues at the Specialized Mental Hospital of St. Amanuel. 50 Eastern Ethiopian communities’ economic well-being is mostly dependent on the cultivation and marketing of Khat. People in eastern Ethiopia are more likely to acquire the habit of consuming Khat because it is freely available and socially accepted there.50–53 In addition, people with schizophrenia may use Khat to increase their coping mechanisms from side effects of antipsychotic medications. 54
Strength of the study
According to our knowledge, this is the first study of its kind, to explore the trend of schizophrenia at Hiwot Fana Specialized University Referral Hospital, Eastern Ethiopia, revealing that schizophrenia has increased significantly during the 5 years. These findings are also used as baseline data for further research on schizophrenia.
Limitations of the study
One limitation of this study was that the patients were not directly interviewed by the researcher or data collectors because the study was based on a retrospective record review. As a result, from reviewed charts, some variables had missing data which resulted in incomplete data. In addition, we did not undertake a separate sample size calculation for the study but included all available cases in the period included which still might limit the power of the study. Moreover, as the study only captured those patients having mental health problems, it did not allow us to make advanced inferential statistics to clearly depict the potential predictors over time increment of schizophrenia problem.
Conclusion
Patients with schizophrenia being treated at Hiwot Fana Specialized University Hospital are increasing over time as shown. People in their productive age group are disproportionately affected, and those who chew khat are most at risk. The magnitude is generally found to be higher in males than in females. It is therefore recommended that early mental health and substance use screening and awareness creation on substance use and mental health is required to improve the level of care for the increasing schizophrenia problem in the study area, eastern Ethiopia needs a comprehensive program for the treatment, prevention, and care of this problem. In addition, institution-based customized interventions can be created to increase the community’s awareness on different levels. The Hospital should improve the recording systems and handling of patients charts, including common risk factors, in the psychiatric outpatient setting. Future research is recommended for exploring beyond the patient card information to explicitly indicate what are the potential predictors contributing to the overtime increment of schizophrenia.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221132160 – Supplemental material for Exploring the trend of Schizophrenia at Hiwot Fana specialized university referral hospital, Eastern, Ethiopia (2016–2020): A 5-year retrospective analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121221132160 for Exploring the trend of Schizophrenia at Hiwot Fana specialized university referral hospital, Eastern, Ethiopia (2016–2020): A 5-year retrospective analysis by Fethia Mohammed, Biftu Geda, Tesfaye Assebe Yadeta and Yadeta Dessie in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our gratitude to Haramaya University for providing the funding and materials needed to complete this study. First and foremost, we would like to express our sincere gratitude and appreciation to the hospital record office and data collectors for their cooperation with our overall activities.
Authors’ contributions
Each author made a significant contribution to the concept, study design, data collection, analysis, and interpretation of the study results. Moreover, the authors read the manuscript draft, made contributions to its creation, and ultimately chose which journal would publish this article. The final draft of the manuscript was read and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from * Ethical clearance was obtained from Institutional Health Research Ethics Review Committee (IHRERC) of College of Health and Medical Sciences (Ref. No. IHRERC/255/2020*.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Haramaya University and the Ministry of Education provided funding for the study. However, the funding agency had no role in designing the study, data collection, analysis, data entry, interpretation of data, or manuscript writing.
Informed consent
Informed voluntary, written, and signed consent was obtained from legally authorized representatives of the hospital before the study. Confidentiality of patient information was also assured by omitting their names and using card numbers instead. This study was conducted following the Declaration of Helsinki
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.