
Abstract
Objectives:
Rapidly progressive interstitial pneumonia is a fatal disease with no established therapeutic options. The aim of this systematic review is to clarify the efficacy of interstitial pneumonia treatment utilizing direct hemoperfusion with a polymyxin B–immobilized fibre column.
Methods:
All patients with adult-onset rapidly progressive interstitial pneumonia including acute exacerbation of underlying chronic interstitial pneumonia were eligible. Primary studies of any design, which compared outcomes of direct hemoperfusion with a polymyxin B–immobilized fibre column treatment such as oxygenation and all-cause mortality with those of conventional therapy, were included. Electronic databases such as Medline and EMBASE were searched through October 7, 2018, and ICHUSHI, the largest database for medical articles in Japan, was also searched. Two reviewers independently extracted the relevant data and assessed the risk of bias in individual studies. The results were reported qualitatively due to substantial heterogeneity between studies.
Results:
Out of 775 records retrieved, 10 reports were eligible and 8 of them were included for further analysis. They were all retrospective studies including a total of 327 patients and contained some risk of bias. There was variation in the administration method of direct hemoperfusion with a polymyxin B–immobilized fibre column treatment such as the timing, frequency, duration and interval. Multivariate analyses of only two studies with historical controls demonstrated beneficial effects of direct hemoperfusion with a polymyxin B–immobilized fibre column treatment over conventional therapy with all-cause mortality hazard ratios of 0.345 (95% confidence interval: 0.127–0.936) and 0.505 (95% confidence interval: 0.270–0.904), respectively. A significant difference of an improvement in the ratio of partial arterial oxygen pressure to the fraction of inspired oxygen in-between two treatment groups was also reported in two studies utilizing historical controls with mean differences of 56.8 and 57.5 mmHg, respectively.
Conclusions:
There is currently insufficient data to support the use of direct hemoperfusion with a polymyxin B–immobilized fibre column treatment for rapidly progressive interstitial pneumonia. It should be instituted for research purposes only until new evidence is available.
Introduction
Interstitial pneumonia (IP) is a heterogeneous clinical entity with known and unknown aetiologies, which is characterized by fibrotic changes mixed with varying degrees of inflammation in the interstitium of the pulmonary parenchyma. 1 Idiopathic pulmonary fibrosis (IPF) is the most common type among idiopathic IPs. 2 The progression of IPF is noted to be accelerated beyond its expected clinical course without explicit causes and this phenomenon is known as acute exacerbation of IPF. 3 Acute exacerbation has also been reported to develop in other types of IP such as connective tissue disease–associated IP (CTD-IP). 4 Once IP is exacerbated, it is extremely difficult to treat. 5 Furthermore, IP can also arise as an acute or rapidly progressive form from the beginning, as in the case of IP complicated with amyopathic dermatomyositis. 6 No therapeutic agents have been proven to be effective for these devastating conditions. 7
The polymyxin B (PMX)–immobilized polystyrene fibre column is a medical device that was originally developed to treat septic patients by adsorbing endotoxin in the blood in conjunction with direct hemoperfusion (DHP). The efficacy of this treatment for sepsis remains controversial because of inconsistent results. Moreover, the findings of previous randomized controlled trials and systematic reviews have been refuted by recent reports.8–12 Nevertheless, some researchers utilized PMX-DHP to treat acute respiratory distress syndrome (ARDS) complicated with sepsis.13,14 These studies demonstrated that this treatment strategy improved the oxygenation and mortality regardless of both the triggers and the presence of endotoxin.13,14 This finding prompted clinicians to further utilize PMX-DHP for the treatment of patients with acute exacerbation of IPF, 15 CTD-IP, 16 and other types of rapidly progressive IPs, 17 since all these intractable conditions are characterized by a common pathological finding of diffuse alveolar damage. 18 This alveolar damage is also present in ARDS. 19 In addition, acute exacerbation of IPF exhibits enhanced neutrophil activity, 20 which is also the same immunopathological change present in ARDS. 19 Previous reports have described beneficial effects of PMX-DHP treatment for patients with rapidly progressive IP including acute exacerbation of IP. 21 However, most of the reports were based on a small number of participants and the efficacy of the treatment remains to be confirmed. Therefore, we conducted a systematic review to clarify the efficacy of PMX-DHP treatment for patients with rapidly progressive IP including acute exacerbation of IP. The study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO (CRD42018109356)).
Methods
This systematic review was prepared according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 22
Eligibility
The inclusion and exclusion of studies for the review were determined based on the participants, intervention, and study type.
All patients with adult-onset rapidly progressive IP were eligible regardless of whether their condition was idiopathic or secondary, which included CTD-IP and drug-induced IP. Acute exacerbation of underlying chronic IP was also eligible. Other diffuse pulmonary parenchymal diseases such as hypersensitivity pneumonitis and vasculitis-associated lung disease, which can be classified as interstitial lung disease (ILD), were also included.
Rapidly progressive IP was diagnosed based on the following criteria: (1) developing or worsening dyspnoea within a month, (2) insufficient or deterioration of oxygenation, (3) newly emerging bilateral radiological opacities, and (4) an exclusion of other complications such as pulmonary thromboembolism and cardiac failure. Participants were not limited by follow-up lengths, previous diagnosis of the disease, prior episodes of acute exacerbations, and treatment history. However, patients with a history of PMX-DHP treatment were ineligible.
The intervention of interest in this review was PMX-DHP treatment, which was performed utilizing the Toramyxin (Toray Medical Co., Ltd, Tokyo, Japan), PMX-immobilized polystyrene fibre column. 23 We included studies administering PMX-DHP treatment at different times, frequencies, durations, and intervals. Any additional therapies including medications and mechanical ventilation were also allowed to be instituted in conjunction with the procedure. Conventional therapy was defined as any treatment excluding PMX-DHP.
The primary outcomes were all-cause and pulmonary-cause mortality while the secondary outcomes were respiratory symptoms, oxygenation, pulmonary functions, radiological findings, health-related quality of life, and side effects such as thrombocytopenia, bleeding, and severe adverse effects.
Primary studies of any design comparing PMX-DHP with conventional therapy were included. It was preferable that any other treatment aside from PMX-DHP would be distributed equally across both comparative groups to evaluate the efficacy of the procedure. However, it was not considered as a prerequisite because non-randomized controlled studies were also allowed to be included in this review. Conference proceedings and articles with only abstracts were excluded due to concerns of insufficient data. For articles in other languages besides English, only reports published in Japanese were included because PMX-DHP was developed and first introduced into clinical practice in Japan. 24
Search
Literature searches were conducted with the following electronic databases: Medline (Ovid), EMBASE (Ovid), Science Citation Index Expanded (Web of Science), Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov. The searches were performed from the inception of each electronic database through October 7, 2018. The search terms were constructed using content-specific subject headings such as ‘interstitial lung disease’, ‘hemoperfusion’, and ‘polymyxins’, which were modified depending on the databases. Search terms were also combined with text words and their synonyms. A methodological filter was not added to a string of search terms to avoid restricting sensitivity (Supplemental Appendix). ICHUSHI (Japan Medical Abstracts Society), the largest database for medical articles in Japan, was also searched for records published in Japanese (from 1959 through April 26, 2019) using search terms translated into Japanese. The grey literature was identified using Google Scholar as previously reported. 25 Reference lists of eligible studies and relevant review articles were also hand-searched.
Study selection and data extraction
After removing duplicates, two reviewers (H.K. and O.M.P.) independently screened retrieved records by titles and abstracts and selected eligible articles by reviewing full-texts if needed. The same reviewers also extracted the data. Any disagreements arising from these processes were sought to be resolved through discussion.
The following data were extracted: (1) the first author name, study year, and location; (2) demographic features of participants such as age, gender, and ethnicity; (3) diagnosis of the disease; (4) the method of delivering PMX-DHP such as the timing, frequency, duration, and the interval; and (5) outcomes, statistical methods, summary statistics, and items associated with a risk of bias.
Risk of bias assessment
A risk of bias in individual studies was assessed by two reviewers (H.K. and O.M.P.) independently using the methodological index for non-randomized studies (minors) instrument. 26 It was composed of 12 items and each item was scored as either 0 if not reported, 1 if reported inadequately, or 2 if reported adequately. The overall risk of bias was assessed based on the score of each item. In addition, a total score was also calculated with the global ideal score of 24 for comparative studies. Any disagreements arising during the risk of bias assessment were resolved through discussion.
Statistical analysis
The binary outcomes such as mortality were summarized by hazard ratios (HRs) or odds ratios (ORs), while the continuous outcomes were reported by the mean difference (MD). The results were not combined due to a small number of studies and substantial clinical and methodological variation between studies. Accordingly, it was reported qualitatively based on the outcomes. The statistical significance was set to a p value of less than 0.05 and the 95% confidence interval (CI) was also presented.
Research ethics and patient consent
Neither ethical approval nor participant consent was sought as this study was based solely on the summary results of previously published articles. Individual patient data were not obtained or accessed.
Results
Out of 775 records identified through seven electronic databases, 31 records were retrieved as full-texts after removing duplicates (n = 124), non-English/non-Japanese articles (n = 6), ineligible articles (n = 382), and irrelevant literature (n = 232). Ten reports/studies comprising five reports in English and five reports in Japanese were eligible for this review (Figure 1). There were no clinical trials and all reports were retrospective observational studies conducted in Japan. PMX-DHP treatment was compared with conventional therapy in eight studies (Oishi et al., 27 Enomoto et al., 28 Takada et al., 29 Furusawa et al., 30 Ichiyasu et al., 31 Nishiura et al., 32 Yoshida et al., 33 and Ikeda et al. 34 ). Another study compared PMX-DHP treatment to plasma exchange (Imamura et al. 35 ) and an additional study compared PMX-DHP treatment with hemodiafiltration (HDF) to conventional therapy (Komaki et al. 36 ). These latter two studies were excluded from further analysis due to the difficulty in inferring the efficacy of the PMX-DHP treatment. The effects of PMX-DHP treatment were evaluated using historical controls in four studies (Oishi et al., 27 Enomoto et al., 28 Ichiyasu et al., 31 and Ikeda et al. 34 ) whereas two studies (Takada et al. 29 and Furusawa et al. 30 ) performed a parallel comparison between the two groups. The two groups with and without PMX-DHP treatment were ambiguous in the other two studies (Nishiura et al. 32 and Yoshida et al. 33 ) (Table 1).
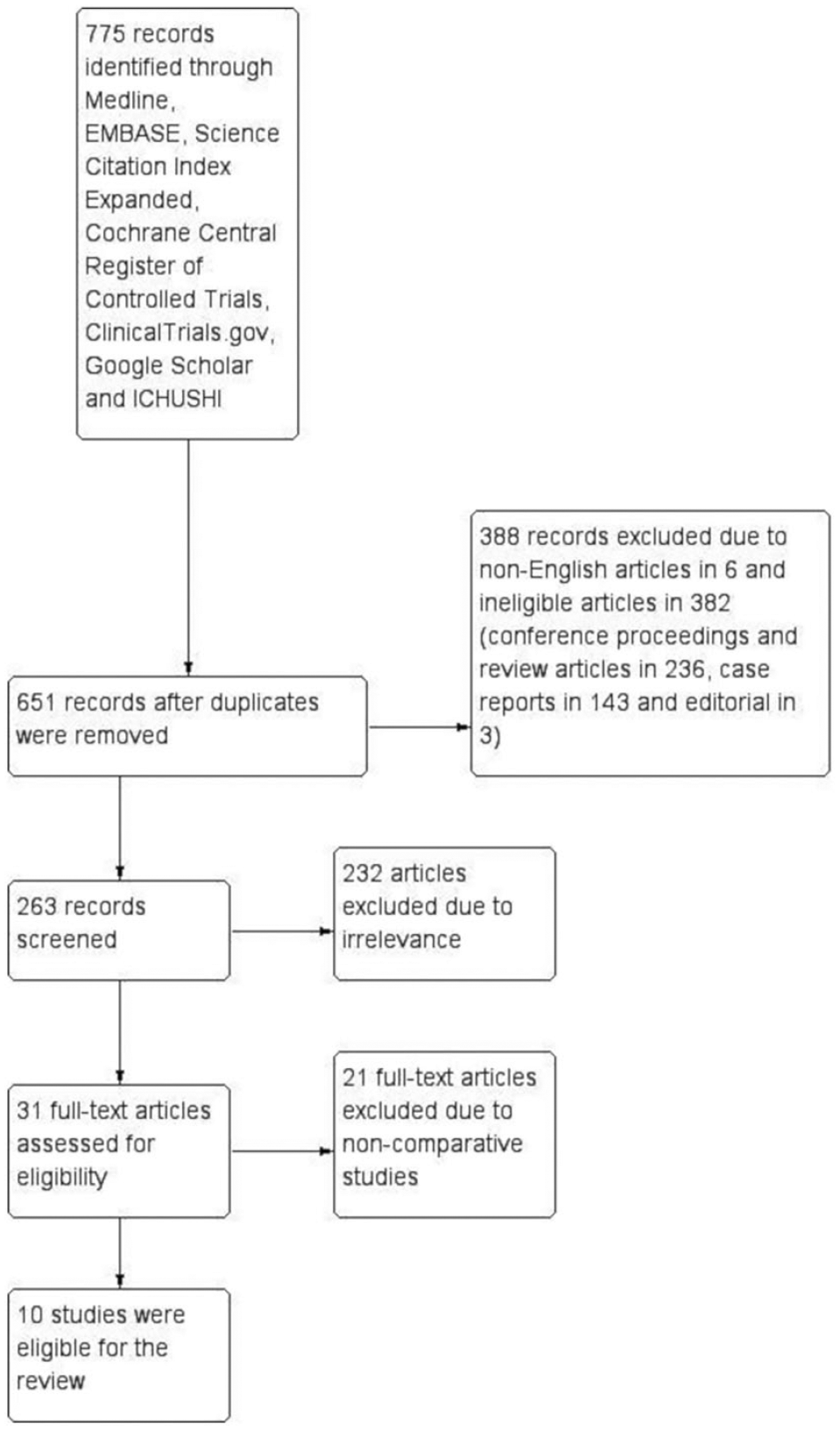
Study flow diagram.
Summary of individual study features.

AIP: acute interstitial pneumonia; CHP: chronic hypersensitivity pneumonitis; CPA: cyclophosphamide; CS: corticosteroid; CyA: cyclosporine; CTD: connective tissue disease; DM: dermatomyositis; IIP: idiopathic interstitial pneumonia; IPF: idiopathic pulmonary fibrosis; IQR: interquartile range; MCTD: mixed connective tissue disease; MPA: microscopic polyangiitis; NSIP: non-specific interstitial pneumonia; PM: polymyositis; PMX-DHP; direct hemoperfusion with polymyxin B–immobilized fibre column; RA: rheumatoid arthritis; Retro-cohort: retrospective cohort study; SD: standard deviation; SLE: systemic lupus erythematosus; SSc: systemic sclerosis; Tac: tacrolimus.
Indicates retrospective observational studies with a historical control.
Includes four cases each of rheumatoid arthritis, dermatomyositis, and undifferentiated CTD and one case of rheumatoid arthritis overlapped with Sjögren syndrome distributed over the two treatment groups.
Includes two cases each of acute interstitial pneumonia and drug-induced pneumonitis and two unspecified cases distributed over the two treatment groups.
Statistics not specified.
Compares PMX-DHP treatment to plasma exchange.
Compares PMX-DHP treatment in conjunction with hemodiafiltration to conventional therapy.
Only acute exacerbation of IPF was treated in three studies (Oishi et al., 27 Enomoto et al., 28 and Yoshida et al. 33 ). In the other studies, acute exacerbation of other types of IPs and newly emerging rapidly progressive IP were also treated. In addition, one study (Nishiura et al. 32 ) had unclear details regarding the baseline IPs. Out of a total of 327 patients included in the review, 151 patients underwent PMX-DHP treatment while 176 patients received conventional therapy lacking PMX-DHP treatment. The PMX-DHP treatment group included 78 patients with IPF, 12 patients with idiopathic non-specific interstitial pneumonia (NSIP), 31 patients with CTD-IP, 19 patients with other diseases, and 11 patients with not adequately explained IP, while the conventional therapy group included 103, 9, 33, 18, and 13 patients with the same diseases, respectively (Table 1). In seven studies that documented the gender distribution in both comparative groups (Oishi et al., 27 Enomoto et al., 28 Takada et al., 29 Furusawa et al., 30 Ichiyasu et al., 31 Nishiura et al., 32 and Ikeda et al. 34 ), there were 96 men and 38 women in the PMX-DHP treatment group while the conventional therapy group included 86 men and 50 women. The mean or median age of participants ranged from 65 to 75.8 and 66.5 to 79.7 years in the PMX-DHP treatment group and the conventional therapy group, respectively (Table 1). All individual studies included in the review contained some risk of bias. In particular, the prospective collection of data, loss to follow-up, calculation of the study size, and contemporary groups were not or inadequately explained in the majority of the studies (Table 2).
Risk of bias in individual studies.

PMX-DHP treatment
In two studies (Nishiura et al. 32 and Ikeda et al. 34 ), PMX-DHP treatment was implemented in cases of acute exacerbation of IP that were unresponsive to corticosteroid pulse therapy with and without mechanical ventilation, respectively.
PMX-DHP was administered at different time points after manifestation of the disease. Oishi et al. 27 and Furusawa et al. 30 reported the time at treatment since the onset of the disease as a range from 1 to 22 and 1 to 53 days, respectively. The mean time at PMX-DHP treatment since admission was 101.5 h in one study (Nishiura et al. 32 ) and it ranged from 0 to 17 days in another report (Enomoto et al. 28 ). Although one study (Ikeda et al. 34 ) also described the time at treatment since admission, it was not clearly reported. An additional report (Ichiyasu et al. 31 ) described the time at PMX-DHP treatment since the diagnosis of the disease, which ranged from 0 to 48 days. Takada et al. 29 mentioned a delay in instituting the PMX-DHP treatment after steroid pulse therapy, which was 0 in six patients and 2–6 days in seven patients (Table 3). The time point of initiating PMX-DHP treatment was unclear in one study (Yoshida et al. 33 ).
Method of administering direct hemoperfusion with polymyxin B–immobilized fibre column (PMX-DHP) treatment.
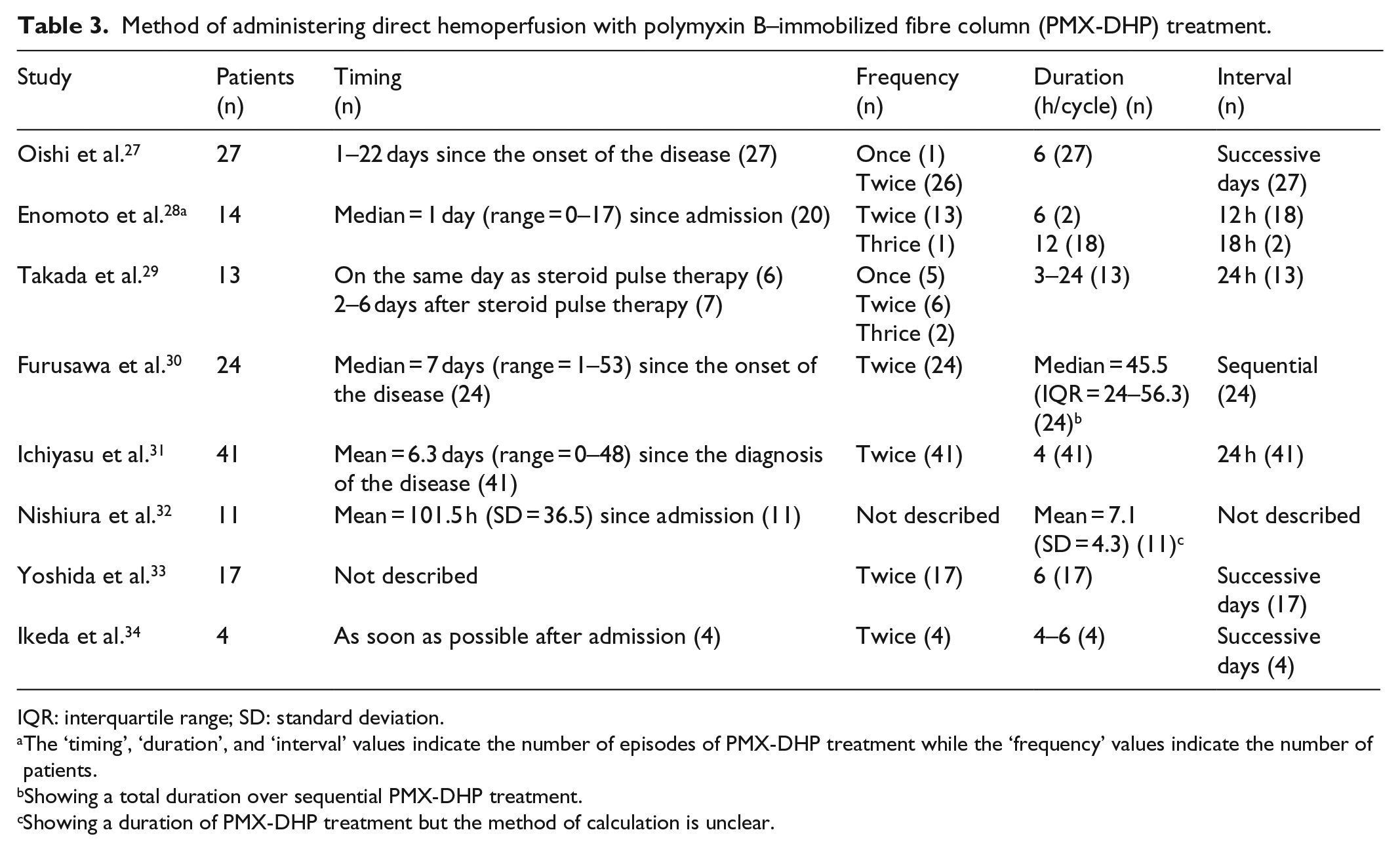
IQR: interquartile range; SD: standard deviation.
The ‘timing’, ‘duration’, and ‘interval’ values indicate the number of episodes of PMX-DHP treatment while the ‘frequency’ values indicate the number of patients.
Showing a total duration over sequential PMX-DHP treatment.
Showing a duration of PMX-DHP treatment but the method of calculation is unclear.
The method of administering the PMX-DHP treatment also varied between studies except for the flow rate (from 60 to 100 mL/min), types of anticoagulants (either heparin or nafamostat mesilate), and access to the blood secured through a double-lumen catheter placed in an internal jugular or femoral vein. In five studies (Oishi et al., 27 Enomoto et al., 28 Ichiyasu et al., 31 Yoshida et al., 33 and Ikeda et al. 34 ), the procedure was performed twice at an interval of 24 h or less and the treatment duration ranged between 4 and 12 h for each cycle. In addition, there were two patients, each of whom were only treated once or thrice. Takada et al. 29 administered the PMX-DHP treatment either once, twice, or three times with each cycle lasting from 3 to 24 h. Furusawa et al. 31 utilized two PMX-DHP columns sequentially and continued the treatment as long as possible beyond 2 h, which resulted in a median duration of 45.5 h. The remaining study (Nishiura et al. 32 ) also reported the mean duration of PMX-DHP treatment as 7.1 h, but the method of administering the procedure was not described in more detail (Table 3).
Conventional therapy
All participants were treated with steroid pulse therapy. Other conventional therapies were not described clearly in three studies (Nishiura et al., 32 Yoshida et al., 33 and Ikeda et al. 34 ) while in five other studies (Oishi et al., 27 Enomoto et al., 28 Takada et al., 29 Furusawa et al., 30 and Ichiyasu et al. 31 ), there was no significant difference in therapy between the two treatment groups (except for PMX-DHP) although no statistical analysis was presented (Table 1). All participants in these studies received a tapering dose of corticosteroids after steroid pulse therapy. One additional immunosuppressant such as cyclophosphamide, cyclosporine, or tacrolimus was administered to 47 patients in the PMX-DHP treatment group and 47 patients in the conventional therapy group, while two additional immunosuppressive agents were administered to 22 patients in the former group and 14 patients in the latter group (Table 1). Sivelestat sodium hydrate was administered to 41 patients in PMX-DHP treatment group and 37 patients in the conventional therapy group (Oishi et al., 27 Enomoto et al., 28 Ichiyasu et al., 31 and Nishiura et al. 32 ). Sivelestat is neutrophil elastase inhibitor, which is widely used in Japan to treat acute lung injury 37 based on the evidence that neutrophils play the central role in the pathogenesis of the disease. 19
Outcomes
Only two studies (Oishi et al. 27 and Enomoto et al. 28 ) reported the oxygenation, while all-cause mortality was described in all studies except for one (Oishi et al. 27 ), which mentioned disease-related mortality (Table 4). Other outcomes such as symptoms, pulmonary functions, radiological findings, and health-related quality of life were not investigated in any study.
Summary of the effect of direct hemoperfusion with polymyxin B–immobilized fibre column (PMX-DHP) treatment. a

HR: hazard ratio; MD: mean difference; NS: not significant; OR: odds ratio; P/F ratio: ratio of partial arterial oxygen pressure to fraction of inspired oxygen.
The number in parenthesis indicates the 95% confidence interval unless otherwise specified.
Indicates overall mortality unless otherwise specified.
Oishi et al. 27 reported a significant difference of an improvement in the ratio of partial arterial oxygen pressure to the fraction of inspired oxygen (P/F ratio) between PMX-DHP treatment and conventional therapy as 59.0 mmHg in the former and 2.2 mmHg in the latter group with a MD of 56.8 mmHg (p = 0.044). Enomoto et al. 28 also reported a similar result with an improvement in the P/F ratio of 58.2 mmHg in PMX-DHP treated patients and 0.7 mmHg in patients subjected to conventional therapy (MD = 57.5 mmHg, p = 0.034) (Table 4).
Oishi et al. 27 reported that disease-related mortality determined by the log-rank test was better for patients subjected to PMX-DHP treatment than those treated with conventional therapy (p = 0.04). The multivariate analysis conducted in the same study also demonstrated a similar result favouring PMX-DHP treatment over conventional therapy with a HR of 0.442 (95% CI = 0.223–0.873) (Table 4).
Out of the other seven studies comparing all-cause mortality between the two groups, Enomoto et al. 28 and Ichiyasu et al. 31 demonstrated significantly better survival for patients subjected to PMX-DHP treatment over those treated with conventional therapy with HRs of 0.399 (95% CI = 0.161–0.988) and 0.485 (95% CI = 0.260–0.904), respectively. The multivariate analysis conducted by the same studies (Enomoto et al. 28 and Ichiyasu et al. 31 ) also confirmed similar results with HRs of 0.345 (95% CI = 0.127–0.936) and 0.505 (95% CI = 0.270–0.904), respectively.
Nishiura et al. 32 reported a better 4-week survival of patients subjected to PMX-DHP treatment by the log-rank test (p = 0.037), but there was no statistically significant difference in 12-week survival (p = 0.249). The multivariate result from the same study was statistically non-significant for both 4-week and 12-week mortality with ORs of 0.40 (95% CI = 0.02–5.01) and 0.75 (95% CI = 0.46–4.99), respectively, although there was a trend favouring PMX-DHP treatment (Table 4).
Takada et al. 29 and Furusawa et al. 30 found no difference in all-cause mortality between the two groups by the log-rank test. However, multivariate analysis was not conducted (Table 4). Yoshida et al. 33 reported no statistically significant difference in 90-day mortality by univariate analysis with a HR of 0.593 (95% CI = 0.189–1.859) although there was a trend favouring PMX-DHP treatment. The remaining one study (Ikeda et al. 34 ) reported 1- and 3-month survival rates, which were better for patients receiving PMX-DHP treatment (100% vs 50% and 75% vs 25%, respectively). However, statistical analysis was not conducted.
Overall, the beneficial effects of PMX-DHP treatment on oxygenation and mortality were only demonstrated by studies with historical controls (Oishi et al., 27 Enomoto et al., 28 and Ichiyasu et al. 31 ) except for a 4-week survival documented in one study (Nishiura et al. 32 ). In contrast, studies that conducted a parallel comparison did not generate significant results.
The following side effects related to the procedure were reported: one case of a local haematoma at the puncture site in one study (Oishi et al. 27 ), one case of mild pulmonary thromboembolism in each of two studies (Oishi et al. 27 and Enomoto et al. 28 ), and several cases of thrombocytopenia in one study (Oishi et al. 27 ). These adverse effects were not severe enough to cause death, decompensate the circulatory system, or discontinue PMX-DHP treatment although Furusawa et al. 30 documented one case of haemoptysis, which led to the termination of the treatment. Therefore, the procedure was considered safe and tolerable with no serious adverse effects (Table 4).
Discussion
This systematic review clarified current evidence regarding the efficacy of PMX-DHP treatment for rapidly progressive IP including acute exacerbation of underlying chronic IP. Oxygenation was improved after PMX-DHP treatment, but the effects of the procedure on all-cause mortality were inconsistent between studies. There was no statistically significant difference in all-cause mortality between PMX-DHP treatment and conventional therapy in studies utilizing a parallel comparison. However, the all-cause mortality was significantly better for patients subjected to PMX-DHP treatment in studies utilizing a historical control. One study with ambiguously defined comparative groups demonstrated a better 4-week survival for patients treated with PMX-DHP treatment, but there was no statistically significant difference by multivariate analysis. There was also no significant difference in 12-week survival by both univariate and multivariate analysis in the same study. Therefore, there is currently insufficient data to support the use of PMX-DHP for rapidly progressive IP in daily clinical practice because well-designed studies demonstrated that survival of the disease was not improved. Pulmonary oxygenation may be temporarily improved, but the finding was also based solely on studies with historical controls. Based on these findings, PMX-DHP treatment should be instituted for research purposes only until new evidence is available.
PMX-DHP was originally developed to adsorb and eliminate endotoxin in the blood of septic patients utilizing the property of PMX. 38 PMX can adsorb endotoxin derived from Gram-negative bacteria, although its clinical use is limited due to serious side effects such as nephrotoxicity and neurotoxicity. 39 The PMX-immobilized polystyrene fibre column contains a fabric knitted with a polystyrene-based carrier fibre, which is covalently linked to PMX. 40 Subsequent studies revealed that other circulatory molecules involved in the pathogenesis of acute exacerbation of IP such as active neutrophils, as well as pro-inflammatory and pro-fibrotic cytokines, are also adsorbed by the medical device and removed from the blood.40–43 In addition, a reduction in these immunological markers was also confirmed in bronchoalveolar lavage fluid after PMX-DHP treatment. 44 These cellular and humoral mediators may be reduced or eliminated from the pulmonary parenchyma shortly after initiating PMX-DHP treatment, which may lead to a temporary improvement of pulmonary oxygenation through a change of vascular permeability. 45 However, this treatment will not address the underlying pathogenesis of this fatal phenomenon. The mechanism that triggers IP progression remains unknown. However, external stimuli or intrinsic acceleration of fibrotic processes may be involved. 5 Since PMX-DHP treatment does not address the underlying cause of the disease, the condition may worsen after discontinuing the treatment unless it is controlled with other therapy. In addition, all-cause mortality will not only be affected by the initial treatment, but will also be influenced by comorbidities or complications such as infection and cardiovascular disease. Therefore, it may be difficult to improve the prognosis of the disease with PMX-DHP treatment alone. However, PMX-DHP treatment may have potential utility as an adjunctive treatment to a mainstream therapy such as corticosteroids and other immunosuppressive agents.
There are some methodological limitations to this review. The findings were based on a qualitative analysis of individual studies and a meta-analysis was not conducted due to the small number of studies and substantial heterogeneity between the studies. Accordingly, some of the results may have been affected by type 2 errors due to the small number of participants. In addition, all studies included in this review were deemed as containing some risk of bias. In particular, the overall risk of bias score of the articles published in Japanese was lower than the articles published in English. Furthermore, Japanese research groups conducted all of the studies. This is likely due to the facts that PMX-DHP treatment was first approved for clinical use in Japan and a fatal form of IP affects Japanese patients more frequently than other ethnicities. 46 These unbalanced reports will extremely limit the generalizability of the findings of this review. Although there may be some studies that were not published due to non-significant results, it was difficult to confirm statistically because only a small number of studies were included in this review. Therefore, we propose the following suggestions for future research to address these limitations. First, a multi-institutional randomized controlled trial is imperative to confirm the efficacy of the treatment. If a cohort study is designed, a high-quality study is essential, which is self-evident from the findings of this review that only studies with a historical control generated significant results. Second, since PMX-DHP treatment is considered as an adjunctive therapy to other conventional treatments, the optimal method of administering the PMX-DHP treatment needs to be considered to maximize the beneficial effects of the procedure in a trial. This review revealed that the time point of initiating PMX-DHP treatment and its duration were diverse, which may have led to inconsistent results between studies, although some reports emphasized the importance of early treatment administration.27,29,30 Third, no studies described other clinically relevant outcomes such as symptoms, pulmonary functions, radiological findings, and health-related quality of life. Therefore, future studies should address these important outcomes. Fourth, studies in other countries or regions such as North America and Europe are required to confirm the efficacy of the treatment. Fifth, articles published in other languages besides English and Japanese were excluded due to a lack of resources in this study. It is preferable to avoid language restrictions in a future review. However, we believe that the impact of this decision was minimal as the number of studies excluded based on this criterion was small. Furthermore, it is an advantage in this study that the largest database for medical articles in Japan was searched for the review given the assumption that a number of research regarding PMX-DHP treatment may have been reported in Japanese since it was developed and first approved for clinical use in Japan. Finally, this systematic review needs to be updated with additional reports in an appropriate timeline.
Conclusion
In summary, there is currently insufficient data to support the use of PMX-DHP for rapidly progressive IP (including acute exacerbation of underlying chronic IP) in daily clinical practice. A thorough and rigorous study such as a randomized controlled trial is urgent to confirm the significance of this promising treatment.
Supplemental Material
Supplement_appendix_R1 – Supplemental material for A systematic review of the efficacy of direct hemoperfusion with a polymyxin B–immobilized fibre column to treat rapidly progressive interstitial pneumonia
Supplemental material, Supplement_appendix_R1 for A systematic review of the efficacy of direct hemoperfusion with a polymyxin B–immobilized fibre column to treat rapidly progressive interstitial pneumonia by Hiroyuki Kamiya and Ogee Mer Panlaqui in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge that this manuscript was proofread for English by a professional editing company (Cambridge English Correction Service). We would also like to thank Mrs Minako Kisaichi, a librarian, for her support to retrieve articles published in Japanese.
Authors’ contributions
H. K. planned the entire research project and analysed the data. He also summarized the result and wrote the manuscript. H.K. has full access to the data and takes responsibility for its integrity as well as the accuracy of the analysis. O.M.P. contributed to conceptualize the research project and supported through literature search, data extraction, and risk of bias assessment. He was also involved in drafting the manuscript.
Data sharing
The dataset used and/or analysed for this review will be available from the corresponding author upon a reasonable request and may become open to the public through a digital repository (such as Dryad) after the final result is published in a journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.