
Abstract
Varicella-zoster virus infection also known as chickenpox is a common clinical entity especially among unvaccinated children and adults. It is said that severity increases as the age increases. Approximately 5%–15% of adult varicella can produce pulmonary manifestations. Varicella pneumonitis occurs especially in at-risk individuals like pregnant, smokers, chronic lung diseases like chronic obstructive pulmonary disease, and immunosuppression. The authors describe a case of severe varicella pneumonitis in a healthy immunocompetent middle-aged woman which posed a great diagnostic challenge. The authors also want to highlight that how a common disease can pose a diagnostic dilemma and present with life-threatening organ failure and timely intervention is needed to prevent mortality.
Introduction
Varicella-zoster virus also known as Human Herpes Virus 3 is the causative agent of chickenpox. Once infected, the virus remains dormant in the dorsal root ganglion only to reactivate later when the trigger sets in or may remain latent throughout life. 1 Unvaccinated individuals are more prone to serious infections. Very rarely life-threatening complications have been observed in immunocompetent individuals also. 2 Varicella is a clinical diagnosis. However, a confirmatory diagnosis can be done by a polymerase chain reaction (PCR) from vesicle fluid, cerebrospinal fluid, bronchoalveolar lavage, and so on. 3 Currently available therapies for Varicella infections include acyclovir, valaciclovir, and famciclovir. In severe cases and suspected resistance to acyclovir, then Foscarnet may be used. 4
Case vignette
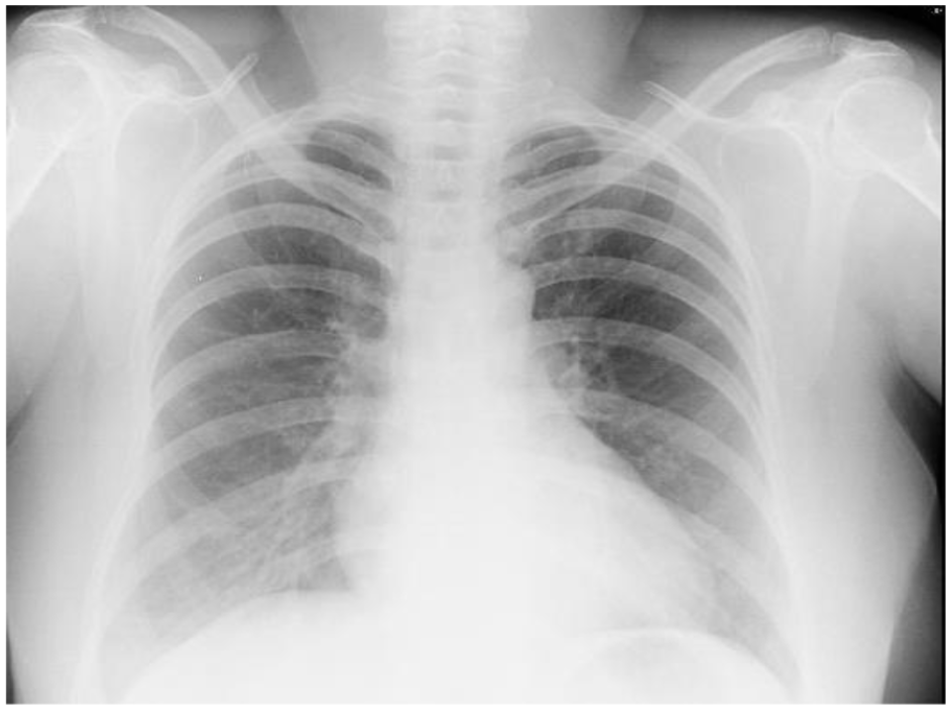
A 50-year-old female was brought to the emergency room with complaints of cough and breathlessness for 1 month. History of on and off low-grade fever was present. The patient had no underlying co-morbidities. On examination, she was tachypneic with a respiratory rate of 34 breaths/minute and saturation was 84% while breathing ambient air. Her pulse rate was 110/min and her blood pressure was 124/80 mm Hg. Respiratory examination revealed bilateral inspiratory crepitations in the lung bases. She was admitted to the high dependency unit because of pneumonia and type 1 respiratory failure. Her blood investigations revealed leukocytosis. Blood cultures were drawn and tests for renal function showed urea of 34 mg/dL, creatinine of 0.8 mg/dL, sodium of 134 mEq/L, and potassium of 3.4 mmol/L. Liver function tests showed total bilirubin of 1.8 mg/dL, aspartate transaminase (AST) (SGOT) of 34 U/L, alanine transaminase (ALT) (SGPT) of 40 U/L, prothrombin time of 11 s, and albumin level of 3.5 g/dL. The C-reactive peptide was elevated. X-ray done during admission revealed bilateral reticulonodular opacities in all lung zones as shown in Figure 1(a). Hence, a diagnosis of interstitial pneumonitis was made. She was started on intravenous (IV) antibiotics for community-acquired pneumonia and cotrimoxazole given empirically for Pneumocystis jirovecii (PCP). Oral glucocorticoids were also added for suspected PCP pneumonia.

(a) X-ray of the patient on arrival to the hospital. (b) A high-resolution CT scan of the lungs showing areas of ground glassing with fibrotic changes and bronchiectatic changes involving both the lungs. A pattern consistent with fibrotic NSIP.
The patient, however, did not show improvement as would be expected with the above treatment. Her oxygen requirement increased every day from 4 L nasal cannula to 60% venturi. Arterial blood gas analysis persistently showed type 1 respiratory failure. Hence, the authors decided to proceed with high-resolution computerized tomography (HRCT) of the chest which showed bilateral symmetrical diffuse ground-glass opacities with superimposed fibrotic changes noted in the form of irregular inter/intralobular septal thickening with associated mild tractional bronchiectasis as shown in Figure 1(b). These findings were consistent with fibrotic non-specific interstitial pneumonitis (NSIP). Hence, a decision to add azathioprine was made along with steroids for the NSIP. To find the etiology of NSIP, an auto-immune workup was done consisting of anti-nuclear antibody, antineutrophil cytoplasmic antibody titers, and rheumatoid factor which were negative.
At this stage, the authors took a Pulmonologist opinion, and bronchoscopy was done. Bronchial washings were collected for bacterial culture, acid-fast bacilli, and nucleic acid amplification test for tuberculosis, fungal culture, nocardiosis, and molecular tests for PCP. To our dismay, all of which were reported to be negative. As a further course of action, we had planned for a lung biopsy. However, we decided to take a complete medical history and redo examination for any missing clues aiding the diagnosis.
A review of medical history and repeat general physical examination was carried out again. Careful examination revealed herpetic lesions with vesicles at the C3 dermatomal level. She was not vaccinated for varicella previously or during her childhood. She also did not suffer from chickenpox illness before this admission. She was not taking any immunosuppressants or steroids. She also had no history of household contact with a similar case or any exposure elsewhere she could remember. She was living with her husband and four children and none of them had any recent chickenpox or herpes zoster. Hence, a possibility of disseminated varicella infection with varicella pneumonia was considered. She was started on IV acyclovir with adequate hydration and monitoring of renal function daily. The patient showed dramatic improvement clinically. IV acyclovir was given for a total duration of 10 days. Post-treatment completion her X-ray showed improvement in the form of disappearing infiltrates as shown in Figure 2. She was gradually tapered off oxygen and discharged without need for supplemental oxygen after 37 days of hospital stay. She is still under follow-up of the Internal Medicine unit chief as a token of gratitude.
A follow-up chest radiography of the same patient showing near-complete resolution of the lung infiltrates.
Discussion
Varicella is a common clinical diagnosis in our setting, especially in children. However, the virus remains dormant in the body once recovered from primary infection. It can reactivate later in the presence of some stressors or acute illness. 1 Here, we report a potentially lethal complication of varicella which is varicella pneumonia. Cases of varicella pneumonia continue to be reported to date even in immunocompetent individuals.5,6 The rates of varicella pneumonia range from 5% to 15% in the adults affected with varicella. 7 It is seen mainly among individuals with underlying lung disease, immunosuppression, pregnancy, or smokers. The authors assume that it is even rare among individuals with a normal lung. Hence, needs a high index of clinical suspicion especially if the herpetic lesions are not visible. The radiological findings seen usually are nodular opacities involving all the lung fields. 8 This was consistent in our case report also. Further HRCT lungs revealed a fibrotic NSIP pattern which may be considered as an atypical presentation of varicella pneumonia. The authors recommend using IV acyclovir for severe varicella pneumonia and also adjuvant glucocorticoid may be added as per evidence given by Adhami et al. 9 The authors believe that this case report would highlight the potentially life-threatening, however, treatable complication of varicella in an immunocompetent adult.
The authors faced a great diagnostic dilemma as the clinical presentation initially appeared to be like an interstitial lung disease supported by type 1 respiratory failure, X-Ray was suggestive of bilateral interstitial infiltrates and HRCT thorax further confirming the same. At this point, the differential diagnosis is only a few. The authors considered possibilities of acute interstitial pneumonia, occupational lung disease, extrinsic allergic alveolitis, autoimmune/connective tissue disease involving the lung, and P. jirovecii pneumonia. However, the patient should have responded to corticosteroids which she did not and bronchoalveolar lavage was negative for PCP, and the patient also did not respond with cotrimoxazole. There was also no history of occupational exposure to any allergens or metals. She was a housewife doing her daily routine as usual for the last 25 years. There was also no history of travel. The next option was to get a lung biopsy and proceed further. However, we decided to take a thorough history and redo the complete physical examination before doing such an invasive procedure. It was only after retaking the history that the patient showed her neck having a few vesicular lesions and some healed crusted lesions at the C3 dermatomal level on the left side. She also admitted to not having been vaccinated for chickenpox during her childhood. Hence, the authors decided to start empirical therapy for varicella with intravenous acyclovir as the last option and ruling out other possibilities. To our surprise, she responded well to treatment and a retrospective diagnosis of varicella pneumonia was made. It was a matter of concern and a learning experience for the authors that a common clinical condition can present as such a rare manifestation, confusing the diagnostic picture. We believe that always repeating a history-taking session and a redo examination can completely change the outcome in difficult cases like this.
Conclusion
This case vignette highlights the importance of thorough history taking and clinical examination skills in diagnosing complicated cases. Whenever in doubt, always having a multi-disciplinary approach may benefit the patient as to make the right diagnosis at the right time. This case also highlights a rare manifestation of a common disease that can get completely missed, not because of a lack of knowledge about it but rather a lack of clinical suspicion at that point of time. The authors also want to highlight the importance of vaccination and post-exposure prophylaxis to prevent developing the disease or severe disease.
Footnotes
Acknowledgements
The authors thank the patient for giving us consent to publish this case report. This case report would not have been possible without the support from our Departmental Head, Professor Raviraj V Acharya. The authors are grateful to Kasturba Medical College, Health Sciences Library, and Manipal University for providing an opportunity to draft out the case report and also for addressing the spelling and grammatical errors in the final stages of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.