
Abstract
Objective:
Newly hired nurses who do not transition well often leave their first nursing position or nursing prematurely, at great cost to themselves, the profession, hiring organizations and patients. The purpose of this secondary analysis study was to better understand the transition experience of new graduate nurses and experienced nurses as they moved to a new setting in nursing, and the preceptor’s role in that transition.
Methods:
Schlossberg’s Transition Theory provided the framework for the secondary analysis of a large qualitative data set that were collected from 118 newly hired nurses who were predominantly female and Caucasian with the majority being under the age of 30 years and having less than 1-year experience. The data available for secondary analysis included all transcripts from the original study.
Results:
Two main themes were identified: Institutional Support and Sense of Self.
Discussion:
Preceptors are critical early in the transition and the newly hired nurse continues to look for support beyond the first year of the transition. Hospitals should consider implementing transition to practice programs that support the newly hired nurse, to include those with prior experience, throughout the first year of transition and should also consider a mentorship program of support after the first year.
Introduction
Nurses can make many transitions during the course of a career including the first transition from student nurse (SN) to new graduate nurse (NGN). Other transitions for experienced nurses may include moving into a new role or specialty, or making a change to a new organization, or both. 1 Structured orientation programs employing preceptors have been used to ease the NGNs transition to professional practice. 2 The preceptor’s role in the successful transition of the NGN to practice cannot be underscored; preceptors play a vital role in effective orientation and retention of the NGN. 3 Preceptors are also used to facilitate successful transitions of experienced nurses who seeking change or moving to a new specialty area. However, little is known about the experience of a professional seeking a change in nursing specialty areas or the role the preceptor plays in that transition.
Implications of a difficult transition to practice
The transition from nursing student to NGN to the role of experienced registered nurse is challenging and long-lasting. It has been reported that it takes a NGN at least a full year to feel relaxed and self-assured practicing in the acute care setting. 4 Because of this lengthy and stressful transition, the retention rate of this vulnerable group of healthcare professionals is poor. 5 Reasons often cited by the NGN for attrition from the practice of nursing include an uncivil work environment, unreasonable workloads, poor nurse physician work relationships, high patient acuities and unfamiliar and advanced medical technology. 5
Early attrition from the profession is costly in terms of healthcare expenditures, patient safety, quality of care and lost human resources. 6 Approximately 25% of new nurses leave their position within the first year of practice, negatively influencing patient safety and healthcare outcomes. 7 It is estimated that the cost to replace one registered nurse (RN) who resigns from an acute care setting ranges from US$10,098 to US$88,000. 8 New nurses affect safety and the National Council State Boards of Nursing (NCSBN) asserts that more than 40% of NGN’s report making a medication error. 9 Conversely, organizations with lower turnover rates of nursing staff have reported fewer patient falls and serious medication errors.10,11
The literature does suggest that support from the hiring institution is essential if the newly hired nurse is to make a successful transition to practice (TTP). Although evidence suggests that a well-organized TTP program using preceptors to ease the transition to professional practice increases retention rates of the NGN, little is known about the preceptor’s contribution to the transition of the experienced nurse who is changing practice settings.12–14 Based on the evidence regarding the graduate nurse (GN), it can be hypothesized that an orientation program aimed at the successful transition of the experienced nurse can increase the retention rate of this valuable member of the healthcare team. The literature fails to describe a developed sense of self in the newly hired nurse, allowing the individual to self-identify learning needs and experiences perceived to be essential for a successful transition. Similar to studies by Klingbeil et al. 15 who examined comfort and confidence and Ziebert et al. 16 who examined supports and stressors of newly hired nurses, this study aims to fill a gap regarding needs and coping resources used by both experienced and NGNs as they transition to a new setting in nursing.
Schlossberg’s Transition Theory 17 is useful when investigating the transitions of the NGN or experienced nurses moving to new to practice settings or organizations and the effect of preceptors. Transitions are processes occurring over time, although the onset may be linked to one identifiable event. 17 Anderson et al. 17 describe the actual transition process as one of moving in, moving through and moving out. 17 This relates to the timeframe needed to successfully transition. The areas of support, strategies, self and situation are what Schlossberg describes as the 4 Ss. Anderson et al. 17 states that no matter what the transition is or where an individual is in the process each person deals with the event differently depending on these 4 Ss. 17 The components of the 4 Ss influence the ability of an individual to cope during a transition. These four components are regarded as either potential assets or liabilities allowing for changes in the ratio as an individual’s situation changes (Figure 1). Schlossberg’s work stems from a fascination with how adults develop and deal with life’s ups and downs. Although the transition experience of individuals may differ, the theoretical framework for understanding the individual transitioning is stable. For this reason, Schlossberg’s Transition Theory can be applied unchanged to aid in understanding the transition experience of nurses. 17

Schlossberg’s Transition Theory and the transition process and the NGN or RN changing practice settings. Adapted from Figure 2.1 (The Individual in Transition), Counseling Adults in Transition, Fourth Edition: Linking Schlossberg’s Theory With Practice in a Diverse World by Mary Anderson, PhD; Jane Goodman, PhD; Nancy Schlossberg, EdD. Reproduced with the permission of Copyright © 2011 Springer Publishing Company, LLC.
Purpose
In an effort to meet the needs of transitioning nurses (NGN and experienced), one pediatric specialty hospital in the Midwest developed a transition program for all nurses (NGN and experienced) entering the hospital system and modeled it after the TTP programs described in the nursing literature. Subsequent to implementation program evaluation was conducted. Data from this program evaluation were used for this secondary analysis. Program evaluation was broad in scope and included some information about preceptors. The purpose of this secondary analysis is to qualitatively address the following questions: (a) as NGNs and experienced nurses transition to a new professional practice setting how do their perceived needs for a successful transition change over the first year and (b) as NGNs and experienced nurses transition to a new professional practice setting how do their coping resources change over the first year of practice.
Method
Design
Data for this qualitative study were drawn from an existing data set for secondary analysis. The focus of the original study was to evaluate (stresses and challenges) a recently redesigned and expanded orientation program for newly hired nurses, including both NGNs and experienced nurses changing practice settings occurring at a pediatric specialty hospital located in a large metropolitan city in the Midwest. Institutional Review Board approval was granted for the original study. For this secondary analysis, permission for secondary data analysis was granted via an amendment to the original study and did not require additional participant consent. Central to the expanded orientation program was the incorporation of three Professional Development Days (PDDs) spanning the first year of employment. Data collection for the primary study took place over the course of 2 years with the final collection point occurring in March 2012. The sample size for the primary study was drawn from a pool of nurses hired over a 2-year period with no exclusion criteria. This includes baccalaureate and associate degree nurses recently graduating from an approved school of nursing, having passed licensure examination with less than 1 year of experience. Experienced nurse is defined as any RN who has worked for more than 1 year in the role. One-hundred and eighteen (n = 118) nurses who participated in the program and first PDD, completed the demographic survey and engaged in debriefing sessions about the extended orientation program were included in the original study and in this secondary analysis. Qualitative data from these debriefing sessions were gathered at approximately 3, 6 and 12 months after the date of hire and these timeframes corresponded with the timing of the three PDDs. In the original study, these three points in time were chosen based on a review of literature, being identified as significant peak times of stress for the NGN.18–20 Structured, focused questions for the original debriefing in order include the following: (a) What went well? (b) What did not go well? (c) Any surprises? and (d) What one thing would you change? In the original study, trained scribes who were not involved as facilitators captured the conversation with paper and pencil, taking extensive notes as participants spoke. Upon completion of the debriefing, the scribe’s notes were transcribed verbatim for analysis later. Details and findings from the original study have been published elsewhere.15,16
The transcriptions from the original study serve as the data set for this secondary analysis. In this case, the burden of participant selection, data sampling and sample size are confined to the limits of the primary study. The primary investigator in this secondary analysis was a PhD student who had access to all transcripts and raw data from debriefing sessions occurring in the original study. The original study provides a large, rich data set and was an excellent fit with the research questions in the secondary analysis. All transcripts (n = 118) from the debriefings were included in this secondary analysis.
Research questions
The qualitative data set generated by the original study supported the need for exploration and secondary data analysis. Specifically, further examination of the preceptor’s role in the transition experience of new nursing hires at a specialty hospital. Schlossberg’s Transition Theory as previously described 17 provides the framework for development of research questions that guide this analysis:
As NGNs and experienced nurses transition to a new professional practice setting how do their perceived needs for a successful transition change over the first year?
As NGNs and experienced nurses transition to a new professional practice setting how do their coping resources change over the first year of practice?
Data analysis
In this descriptive, qualitative study, a general inductive approach was utilized. This allows the researcher to examine the data without preconceived hypothetical/deductive ideas. Thus, the emergence of conceptual categories and descriptive themes can emerge supported by a framework (Schlossberg). Themes are usually embedded in a framework of interconnected ideas. 21 Analytic analysis and word count were also used. Analytic analysis was completed using manual techniques. Original transcripts were read and reread in the order they were collected to gain a greater appreciation for the context of the transcribed dialogue as it related to the research questions and framework. All transcripts were read line-by-line and during the second and subsequent reads, small bits of text, key words and phrases were identified and extracted. 21 After emerging themes were recorded, those themes were reread in an attempt to identify potential subthemes. Words that appeared to be used frequently and identified as being relevant to Schlossberg’s theory (support, strategies, self and situation) and the research questions as previously described were underlined and counted. Word counts are useful for discovering patterns of ideas in the body of the text of the transcription. 21
Rigor
Trustworthiness in this study was established by the use of a well-kept audit trail and thematic memos. The audit trail for this study included all raw data; the “clean” copy and the working copy. Thematic memos were collected, recorded and stored in a reflective journal kept by the principal investigator throughout the secondary analysis process. Thematic memos capture the cognitive process and ideas about connections between the data and emerging codes or themes as they relate to the research questions and Schlossberg’s Transition Theory. As data analysis progressed, the rules on what was included or discarded including reasons were recorded. A working copy of the raw data was reviewed individually and collaboratively by the research team for themes and subthemes. The process of staged data analysis and collaboration allowed for investigator triangulation, another method to help establish trustworthiness of findings and reduce bias-based decisions. 21
Results
The original data were collected from 118 nurses who self-report a mean age of 28 (±6.7(SD)) years; were predominately female (92.5%), Caucasian (92.5%) and baccalaureate (BSN) prepared (75.2%). There were 76 (64.4%) nurses with less than 1 year of experience. Due to similarities in research questions 1 and 2 and the overlap of findings related to perceived needs and coping resources, findings are presented together. Coping resources not related to perceived needs, addressed in research question 2 are addressed separately. Two main themes and five subthemes were identified: Institutional Support (subthemes: Human Connection, Process Approach and Resources) and Sense of Self (subtheme: Self-Awareness and Fear). Themes and subthemes including word count are presented in Table 1.
Themes, subthemes (word count) and Schlossberg’s Transition Theory.
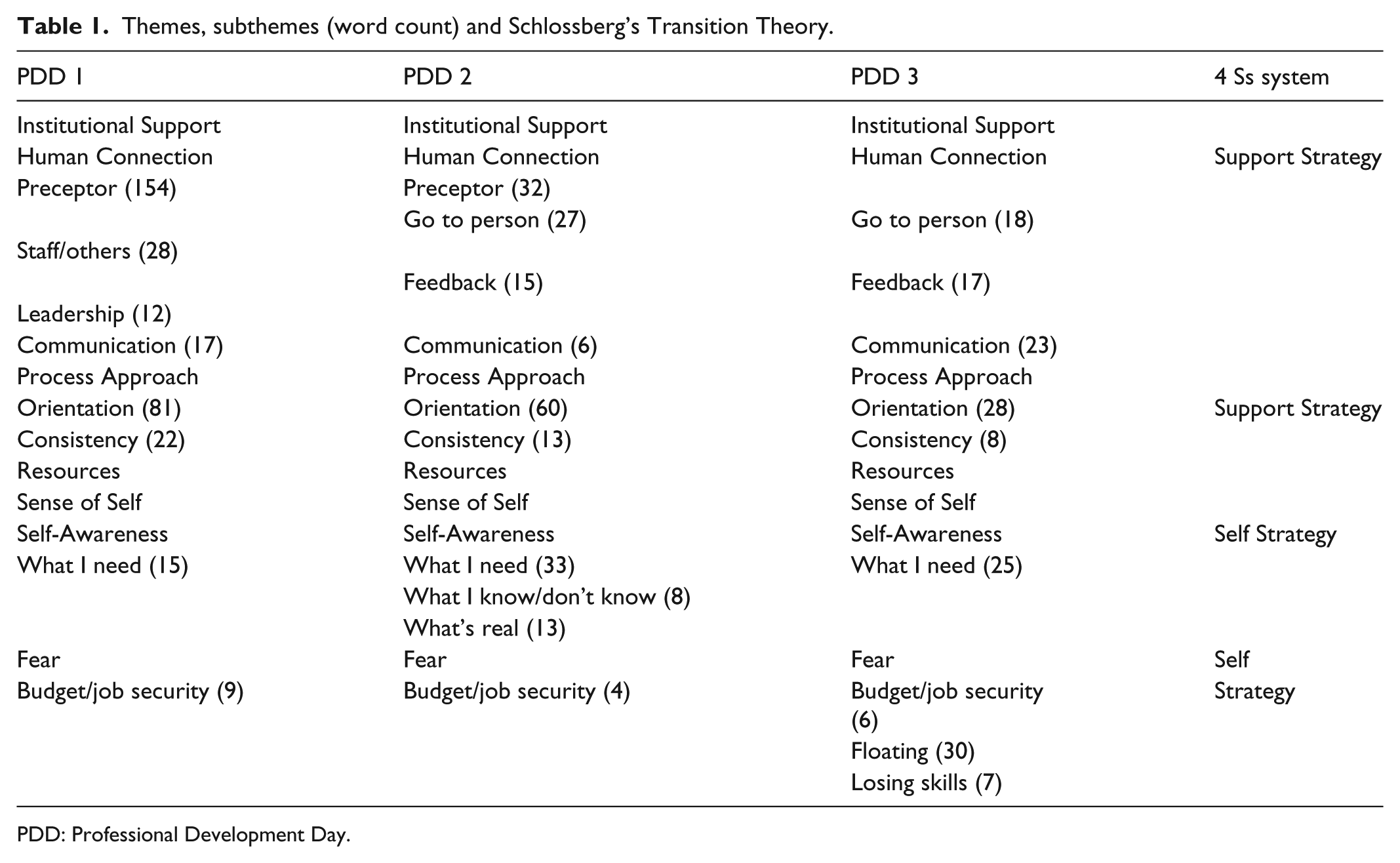
PDD: Professional Development Day.
Institutional support
Institutional Support is a formal and informal functional system of social structure and encouragement that is typically provided by hiring organizations to ease the transition of nurses to new roles through interconnectedness. The subthemes of Human Connection, Process Approach and Resources help guide transitions. Newly hired nurses look to the institution to provide support needed for a successful transition to independent practice. Similarly, newly hired nurses perceived that a Human Connection is needed to make a successful transition. Four groups of individuals were identified by the newly hired nurses, as being critical to a successful transition they include the preceptor, staff and others, leadership and a “go to” person. First, the newly hired nurses perceive preceptors as important and necessary for successful TTP. Preceptors were considered to be a major asset under certain conditions: when the numbers of preceptors were small, a trusting relationship had been established and communication between multiple preceptors was evident. Many participants commented that a consistent and small number of preceptors during the transition were preferred. The following remarks were made by NGNs from the first PDD. “… a total of six preceptors so far. It’s much better with less variability.” Another participant remarked, “… great preceptors … had two main preceptors ….” Yet another NGN participant remarked as to why a smaller number of preceptors had been preferred and stated, I liked having two to three preceptors to work with toward the end of orientation … different perspectives … see different things to focus on … I had reached a point where I was ready to be off orientation and feeling there was not much more I could learn from my preceptor, but having different people toward the end they saw what I still needed.
Preceptors were most relevant to the nurse during the first 3 months of the transition and decreased over the course of the first year. This is demonstrated by the number of times the word preceptor appeared during the first PDD and tapered during subsequent interviews (Table 1).
During the first PDD, the newly hired nurses who were changing practice settings perceived staff and others as another part of the Human Connection needed for successful transitions to practice. An experienced nurse who was changing practice setting and specialty area stated, “I’m not a new nurse … came from the adult world … nurses were very helpful to me and identified resources.” Another NGN participant noted, “… staff always have an answer for me … they know where to look.” Perceived needs for a successful transition in relationship to the theme Human Connection changed over time for the participants. As the statements about preceptors deceased over time, different support persons emerged. Participants from the second and third PDDs perceived the need for a “go to” person to help support them with the transition (Table 1). A “go to” person was described using terms such as mentor and resource person. Mentors were support persons who had a more formal role and were identified by the hiring institution as such. Participants from the second PDD perceived the mentor as “… some sort of bridge between orientation and being off.” Still others perceived a mentor or resource person was needed to “… help you find your way.”
Key to Human Connection was the perception that feedback from preceptors and leadership was needed for a successful transition and was noted at PDD two and three. Participants desired feedback to be timely at the second PDD and desired an increase in positive feedback at the third. Feedback that was rushed or lacked thoughtful consideration was considered a liability; however, feedback that was timely and constructive was thought to be an asset. A NGN participant from the second PDD wanted more constructive criticism and described the evaluation process in terms of a liability when they stated they felt like the evaluation process was “… cut and paste … I know I need to improve as a new RN so tell me.” Another NGN participant from the second PDD remarked that it felt that the performance evaluation was something they had to get done and it didn’t feel like “decent feedback” and another participant stated they had not even had a 90-day evaluation. Participants from the third PDD session also remarked about positive feedback noting that there was “not enough.” A NGN participant remarked about the content and delivery of feedback, “… need more positive feedback person to person, not by email from leadership. The face to face encouragement is what matters most not the electronic feedback.”
Structure is key in Institutional Support. Both groups experienced and newly hired nurses perceived that Process Approach, or a step-by-step method of doing something, is needed to ensure a successful transition to professional practice. Both groups were provided a structured, ordinal orientation, moving them through the orientation in an organized and orderly fashion with a graduated progression of increasingly difficult patient care assignments. The benefits of an organized orientation were noted at all three PDDs. Participants remarked that “… staged orientation was good … was going well.” One NGN participant from the third PDD remarked, “… staged orientation was good, but it was hard with so many on orientation.” Similarly, experienced nurses perceived that a tailored orientation based on prior experience was needed to help them successfully and quickly transition to the new pediatric practice specialty. One experienced nurse participant from the first PDD stated that “… orientation was aimed more toward NGNs … need something more formalized for experienced RNs.” Another experienced nurse participant from second PDD made a similar remark when it was stated that prior experience needs to be acknowledged, “… they sometimes treat us like new grads.”
A key component of Institutional Support is typically access to adequate resources to support the smooth transition of nurses. Competing for access to resources and opportunities were noted to be a problem and liability for the NGN and the experienced nurse. Both groups of nurses perceived that open access to high acuity patients was needed for a successful transition to professional practice. Participants were able to see the inherent problem with large groups of new hires starting orientation and professional practice at essentially the same time. A NGN participant from the first PDD stated that “… it makes it hard that a group starts all at the same time … they all need the same experiences.” One NGN participant from the third PDD summarized stating, “Don’t hire a bunch of new RNs all at the same time. This causes issues for over a year down the road.”
The theme, Institutional Support, is closely linked to Support and Strategies in Schlossberg 4 Ss system. Support is key to handling stressors. Stress is typically drawn from multiple sources and associated with transitions. Results from this analysis found that the Human Connection is important. Human Connection includes role models who teach, instruct supervise and socialize the newly hired nurses. Strategies allow newly hired nurses to cope with the transition. Coping Strategies include those that seek to modify the situation, modify the meaning of the situation or manage stress. Individuals, who make up the Human Connection, assist the newly hired nurse to directly manage the stress of a transition, strengthen their resources and help ensure a successful transition. Institutional Support and the associated subthemes allow nurses to modify the situation and ease the strain of the transition.
Sense of self
The second theme that emerged from the data was Sense of Self (Table 1). Sense of Self is described as an internal awakening or an awareness of Self that allows participants to identify needs, fears and uncertainties that lie within the self and serve to undermine a successful transition. Participants from the first PDD were able to identify what type of patient experiences they thought they needed in order to make a successful transition and stated, “… need to take the same patients more than once to build skills with that patient and build skills by repetition.” Participants could also identify unit-based learning opportunities that they determined would be helpful and necessary for a successful transition. A NGN participant from the second PDD commented, “Need more time with experienced preceptor … need more one on one time … my preceptor was resourced out during my orientation, so she wasn’t available as she should have been.” A NGN participant from the third PDD noted, “We all need a lot more cross-training across the intensive care units (ICUs).”
Additional coping resources not related to perceived needs
Findings from the second research question, addressing changes in coping resources over the first year of practice contributed to the emergence of Sense of Self as a theme and generated coping resources that were not related to perceived needs. By the second PDD or at the 6-month mark of transition, participants realized what was needed in terms of experiences and opportunities. They were also becoming aware of what they knew and what they still needed to learn (Table 1). A NGN participant from the second PDD who had orientation during the summer months with little exposure to common respiratory issues during the viral season noted “… may need some orientation outside of ‘normal patient population seasons.’” The same participant went onto say, “… don’t know patient population or how to treat them … wasn’t captured during orientation.” Another NGN participant said, “… can figure things out now … trusting intuition … know who needs to be seen first.” Another NGN participant added, “… big picture starting to come together.”
One NGN participant from the second PDD states “… was half way through orientation … don’t know what to do with some kids.” An experienced nurse from the second PDD made a similar remark and stated how much she still questioned herself. As participants from the second PDD were able to describe what they knew and did not know, they were also able to recognize and verbalize what was real in terms of taking care of the specialty patient population. Participants were beginning to realize the actuality of caring for critically ill children. This is only evident in the data at the 6-month mark or at PDD2. A NGN participant stated, “… was part of an ugly code, bereavement issues discussed but this was nothing I expected. Don’t sugar coat the experience that patients will die during orientation … give us the ugly details.” Another NGN participant added, “… be less gentle when this information is presented.”
Fear was a sub theme emerging from the data in relationship to the theme Sense of Self and it was represented across all points in time. Participants were all employed during a time of organizational change within the specialty hospital system, leading to concerns about budget and job security. Participants were also afraid that during times of fluctuating census skills would be lost. A participant from the third PDD stated, “… difficult to keep up on skills and knowledge since I’m a new grad and feel like I’m losing my skills.” Participants also had concerns and fear about floating to different units. A NGN participant remarked, “Sometimes it feels so unsafe to float ….”
The theme Sense of Self maps to Self and Strategies of the 4 Ss system. Sense of Self and Self-Awareness about what the participants needed, what they knew and did not know and what they perceived as real were an effective coping Strategy for successful transition to professional practice. The greatest time of Self-Awareness occurred at the second PDD, when participants verbalized all three elements of self-awareness as a coping resource. The negative energy and internal chaos created by a sense of fear is counterproductive but must be acknowledged as a coping Strategy used by both groups of nurses. Fear as a coping Strategy was used as a response to untoward situations that arose during the process of transition. As nurses’ transition to professional practice or transition to a new professional practice setting, they use many coping resources to make a successful transition. Throughout the first year of transition, participants relied on a mix of Support, Self and Strategies as they moved in and through transition (Figure 1).
Change over time
Early on in the transition, the NGN and the experienced nurse relied upon the preceptor to help them with the transition. Over time, at approximately the 6-month mark or at PDD 2, the newly hired nurses moved away from reliance on the preceptor and looked to a mentor or another resource person to provide them with personal support needed for successful transition. The reliance on a mentor or other assigned resource nurse is still evident 1 year after hire or at PDD 3 indicating the newly hired nurse still required a go to person for questions and help with unfamiliar patient care situations. The need to connect with leadership is noted early in the transition or at approximately 3 months after the hire date or at PDD 1. At PDD 2, newly hired nurses sought timely and constructive feedback. Over time and at PDD 3, nurses were looking for more positive feedback that was delivered face to face.
Throughout the process of transition, newly hired nurses found a staged orientation to be helpful and a bridge to successful nursing practice. Participants throughout the first year of practice also perceived that unobstructed access to high acuity patients was vital to successful transition.
Newly hired nurses, at PDD 2 had a heightened sense of self and self-awareness and were able to identify what they know and what they don’t know in addition to what they need for successful transition. They also have a sense of what is real within the pediatric specialty population and can express that realization. Both groups also used fear as a coping mechanism and this shadowed both groups throughout the first year of practice and transition.
Discussion
The purpose of this secondary analysis was to examine and describe NGNs and experienced nurses’ transitions to practice and perceived needs for a successful transition over the first year of practice. Similarly, to describe how coping resources change over the first year. The NGN and the experienced nurse specialty share a similar path as they transition to independent practice or alternatively into new care environment. Each relies on Institutional Support including The Human Connection, Process Approaches and Resources to provide a more robust transition. Preceptors are just one component of this. The role of the preceptors is important even for nurses with experience and were considered to be a major asset under certain conditions: when the numbers of preceptors were small, a trusting relationship had been established and communication between multiple preceptors was evident. This study revealed that both groups value the Human Connection and support offered by a limited number of preceptors. Of note, this finding differs from what the current body of literature suggests. Literature consistently describes that the preferred method for orienting the nurse in transition is 1:1 consistent pairing of preceptor with newly hired nurses, regardless of level of experience or years of practice.4,12,18,22 Findings from this analysis suggest that the nurse in transition prefers a small and consistent group of preceptors.15,16
As each group of transitioning nurses moves from reliance on a preceptor, they look for a mentor or “go to” person as another coping resource and Human Connection to help them when questions arise, or difficult patient care situations occur.4,16,18,23 The literature also identifies feedback as a type of support newly hired nurses seek.4,18 Fink et al. 18 reported that NGNs identified nurse manager feedback as a way that would have facilitated TTP. The experienced nurse expects a well-planned orientation program, and an orientation tailored to individual learning needs acknowledging prior experience. The literature suggests that the use of well-planned and executed orientation programs increases the retention of newly hired nurses.24,25 Nurses in both groups also competed for resources and unfettered access to high acuity patients throughout orientation. This is another finding that has not been previously reported.
Participants had a heightened Sense of Self and Self-Awareness that emerged in the findings at the 6-month mark of the transition. The phrases “what I know and don’t know are present only at this point. The phrase, “what’s real” is present at the second and third PDD. The Sense of Self and the ability to articulate: What I Need, What I Know and Don’t Know have not been reported in the literature and should be considered a new finding. The ability to sense and voice: What’s Real, deals with the harsh reality of dying patients. The literature also suggests that participants were able to identify: What’s Real when caring for patients at end of life and dealing with futility of care. 18
Fear as a coping resource was identified in this study, is considered a liability and has not been reported elsewhere in the nursing literature. In spite of the upheaval caused by organizational change while data were collected, participants were still fearful. Concerns with regard to the practice of floating and losing skills due to fluctuating census shadowed both groups of nurses throughout the entire first year of practice. Nurses who participated in the extended orientation program used a variety of coping resources to aid them with the transition that were consistent with 3 of the 4 Ss: Support, Strategy and Self. Findings also suggest that newly hired nurses never moved out of transition but were mired in it for the entire first year of practice.
Limitations
One of the distinct limitations of secondary analysis of data is that the researcher is unable to ask participants additional, follow-up questions. The ability to ask additional questions may have uncovered coping resources employed by both groups of nurses as they transitioned to practice. Lack of an audiotaped interview in this instance has limitations and advantages. An audiotaped interview would have also provided a more detailed data set. However, it would have been impossible to identify which remarks the experienced nurse made without the transcription process, as individuals were noted as experienced or not during the PDDs. A second limitation that must be considered when interpreting the findings is the study site and population. The original study was conducted at a single pediatric specialty hospital located in the Midwest. The sample was predominantly white females who had been prepared at the baccalaureate level. Therefore, findings from the current study represent only those participants who took part in the original study and cannot be generalized to different programs in other organizations. Another limitation is some time has lapsed since the original study was conducted. Despite this, understanding transitions is a timely and relevant nursing issue.
Implications
It has been well studied and documented that NGNs struggle with the transition to independent practice. Knowing this, nursing educators should make overt efforts to prepare graduating nursing students for transition to professional practice. A capstone course that includes a frank discussion about length of time needed to successfully transition, the emotional aspects including fear and heightened awareness of the long process may help the NGN conceptualize and better manage the process. The capstone course should also include a precepted clinical experience that comes with clear learning objectives, benchmarks and outcome objectives that can be utilized to measure student’s progress. Learning activities designed to have the student begin to see the patient as a whole or “see the big picture” versus a singular diagnosis, set of lab values and diagnostic test results, will also help the student begin to think like a nurse and may make the transition to NGN easier.
During the first 6 months of transition, healthcare organizations need to realize that the newly hired nurses focus is egocentric and concerned with assimilation to the role and new work setting. With this in mind, orientation programs for both groups of nurses should be well structured and each group should be provided with a small and consistent group of preceptors who will help lead them through the transition. Orientation for the experienced nurse should be tailored based on an assessment of what is specifically needed and identified as essential for successful transition. During the second 6 months of the transition, the newly hired nurses focus is less egocentric and they begin to see the “bigger picture” of patient care. During this timeframe, the newly hired nurses should be supported by a group of well-placed mentors who can assist in guiding them through this next stage of transition. Hospital educators may also want to consider simulation-based learning, providing newly hired and transitioning nurses with low incident high risk experiences. Simulation may alleviate the anxiety caused when these types of patient care experiences are limited by patient census or competing members of staff. Healthcare organizations may also want to consider staggering the hiring process rather than hiring large numbers in the early summer and December when new graduates enter the workforce.
Despite easing due to the most recent recession, the nursing shortage in the United States is expected to grow to 260,000 RNs by 2025. 26 The European Union forecasts a shortage of 800,000 by the year 2020. 27 For these reasons, the public and the profession should adopt and implement nurse residency programs (NRPs). Similarly, NRPs should be required for the nurse who is transitioning to a new nursing specialty. The Report on the Future of Nursing (recommendation III) calls for the implementation of NRPs and asserts that state boards of nursing, accrediting bodies, the federal government, and healthcare organizations should take actions to support nurses’ completion of a TTP program or NRPs. 28 These programs should be supported and available to the nurse upon completion of a prelicensure program, or when the nurse transitions to a new clinical practice area. 28
In the years since the publication of The Future of Nursing Report, NRPs have been developed or expanded by the institutions that hire the nurses but systematic efforts to accurately track the growth of these programs is limited. Progress is difficult to track because the term “residency” has many different definitions, the length of residency programs vary greatly and residency programs are offered to nurses at all levels of education in many different healthcare settings. Because of these variations and the fact that comprehensive data on residencies is sparse, it is difficult to evaluate the overall growth of NRPs. 29 If nursing is to address the predicted global shortage of this valuable healthcare asset, we have a responsibility to explore avenues that will help NGNs and experienced nurses successfully transition to new practice settings and keep them a member of the profession.
Footnotes
Acknowledgements
The authors thank Carol Klingbeil DNP, RN, CPNP-PC, University of Wisconsin, Milwaukee,
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Children’s Hospital of Wisconsin (CHW 10/43).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from all subjects before the study. (original study)