
Abstract
Objectives:
Patients undergoing double-balloon enteroscopy require sedatives such as midazolam; however, patient’s body motion often hampers the outcome of double-balloon enteroscopy. Recently, dexmedetomidine has been used for endoscopic sedation and was reported to effectively reduce body motion. This study aimed to evaluate the efficacy and safety of sedation with dexmedetomidine in double-balloon enteroscopy (UMIN ID000015785).
Methods:
A prospective, observational study was conducted in 81 patients who underwent 111 double-balloon enteroscopy from July to December 2015 (dexmedetomidine group). The medical records of 112 patients who underwent 166 double-balloon enteroscopy with midazolam and pentazocine sedation from January 1 to October 31, 2014, were used for comparison (midazolam group). After propensity score matching, 182 double-balloon enteroscopy (91 double-balloon enteroscopy for each group) were analyzed.
Results:
There were 13 cases (11.7%) with body movements in the dexmedetomidine group. Comparison of the two groups matched by propensity score showed that the dexmedetomidine group had less body movement (12.1% vs 34.1%, p = 0.001) and less respiratory depression (50.5% vs 68.1%, p = 0.023). Hypotension (8.8% vs 4.4%, p = 0.232) and bradycardia (2.2% vs 0%, p = 0.497) were not significantly different in the two groups.
Conclusion:
Using dexmedetomidine for conscious sedation can reduce body motion and respiratory depression compared to our previous records.
Introduction
Double-balloon enteroscopy (DBE), developed by Yamamoto and colleagues,1,2 enables the observation of the entire small-bowel and intervention such as biopsies, hemostasis, balloon dilatation, and/or polypectomy. However, DBE can be uncomfortable and time-consuming, and patients who undergo the procedure usually require sedatives and analgesics. 3 Midazolam (MDZ) or propofol is usually used for sedation during DBE, but these two agents tend to suppress respiration or blood pressure. Moreover, an analgesic is often needed during DBE which may induce further hypotension and respiratory depression. Restlessness or marked body movement during sedation with these agents hampers endoscopic interventions, which we also experienced during DBE. 4 Dexmedetomidine (DEX), an α2-adrenergic agonist, acts as a sedative by inhibiting the firing of the locus ceruleus of the brain stem and as an analgesic by inhibiting norepinephrine release at the neuroeffector junction. 5 Furthermore, DEX facilitates conscious sedation of patients and maintains stable respiration and circulation. Several randomized controlled trials have evaluated the efficacy of DEX in comparison with MDZ for gastrointestinal endoscopy, especially endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic submucosal dissection (ESD).4,6–10 However, there are no reports on the use of DEX in DBE. Therefore, the aim of our study was to prospectively evaluate the efficacy and safety of sedation with DEX in DBE.
Methods
Study design
First, consecutive patients who were scheduled for DBE with DEX sedation from July 1 to December 31, 2015, and who provided written consent were prospectively enrolled in the first part of this study. The exclusion criteria were (1) age ≤20 years and (2) serious organ disorder (i.e. heart failure (NYHA (New York Heart Association) classification grade 4), respiratory failure (Fletcher–Hugh–Jones classification grade 5), and hepatic failure (Child–Pugh classification grade C)). This part of the study included 84 patients (118 DBEs) (DEX group). However, three patients (seven DBEs) were excluded because the same insertion route was used during the second time, overtube was not used, insertion from stoma, and lack of records. Finally, 81 patients (111 DBEs) were enrolled.
Second, we retrospectively investigated the adverse events in patients who were sedated with MDZ (MDZ group). We compared the frequency of adverse events between the MDZ and the DEX groups using propensity score matching. For the patients in the second part of this study, we analyzed data of 136 patients who underwent 193 DBEs with MDZ and pentazocine sedation from January 1 to October 31, 2014, in our hospital. In total, 27 DBEs (24 patients) were excluded because they did not have a sedation record or only observation of the colon was performed; 166 DBEs (112 patients) remained.
This study was approved by the ethics committee of participating institution and was registered with a registry approved by the International Committee of Medical Journal Editors (UMIN ID000015785).
Study protocol and monitoring
All DBEs were carried out using either of the two types of DBE system, the diagnostic type (EN-450P, EN-580XP) and the therapeutic type (EN-450T, EN-580T) (Fujifilm, Tokyo, Japan), with CO2 insufflation. CO2 insufflation was used in All DBEs.
In the MDZ group, MDZ 0.02 mg/kg was injected intravenously for induction. Sedation was kept at levels 3–5 of the Ramsay Sedation Scale (RSS), which is equivalent to moderate sedation (Table 1). 11 MDZ 0.02 mg/kg or pentazocine 15 mg was additionally injected intravenously during restlessness, body movement, or awaking.
Ramsey Sedation Scale.

In the DEX group, patients were sedated with DEX using a loading dose of 6 μg/kg/h over 10 min followed by 0.4-μg/kg/h infusion until the bispectral index (BIS) on the electroencephalogram (EEG) reached 60–80, which is equivalent to moderate sedation. An additional pentazocine dose of 15 mg was given at the beginning of DBE. When needed, 1 mg MDZ, 7.5 or 15 mg pentazocine, or DEX dose adjustment was given.
The blood pressure, heart rate, oxygen saturation, and electrocardiogram were monitored during DBE. Blood pressure was measured every 2.5 min. In addition, BIS and body movements were recorded in the DEX group. Body movements were scored based on the responses described in Table 2.12,13
Score of body movement.

Propensity score matching
To compare sedation between the DEX and the MDZ groups, we obtained two subsets from each group using propensity score matching. The propensity scores were estimated using a logistic regression model that included the following 10 covariates: age, sex, body mass index, ASA (American Society of Anesthesiologists) physical status (≤2 and ≥3), surgical history, indication, heart disease (none, NYHA <3, and NYHA ≥3), respiratory diseases (none, Hugh–Jones ≤3, and Hugh–Jones ≥4), insertion route, and type of endoscope. Based on the propensity score for receiving DEX, patients who received DEX and those who received MDZ were matched on a 1:1 basis.
Patients’ and endoscopists’ assessment
After examination, we handed questionnaires to the patients and collected them on the next day. Both patients and endoscopists evaluated the state of sedation during DBE using a 5-point Likert scale (1, unacceptable; 2, not so good; 3, fair; 4, enough; 5, excellent).
Definition
Hypotension is defined as a decrease in systolic blood pressure ≥30% from baseline and systolic blood pressure <80 mmHg; respiratory depression is defined as percutaneous oxygen saturation level <90%; bradycardia is defined as decrease in heart rate ≥30% from baseline and <40 beats/min.
In both groups, body motion was considered present if body restraint was required for violent body movement, that is, level 4 or 5 in the movement scale.
Statistical analyses
Continuous data were compared using the Mann–Whitney test. Categorical variables were tested using the corrected χ2 test or Fisher’s exact test, as appropriate. Multivariate analysis was performed using multiple logistic analyses. A p-value <0.05 was used to indicate statistical significance. All statistical analyses without propensity score were performed with the SPSS software (Statistical Package for Social Science, IBM SPSS Statistics, version 23 for Windows; IBM, Armonk, NY, USA). Propensity score matching was performed with JMP, version 11 (SAS Institute, Cary, NC, USA).
Ethical approval
This study was approved by the ethics committee of our hospital. Written informed consent was obtained from all patients before DBE.
Results
Patient and examination characteristics
The patient and examination characteristics, and adverse events in DBE are summarized in Tables 3 and 4. All patients were Japanese.
Patient characteristics in MDZ group and DEX group before propensity score matching.

MDZ: midazolam; DEX: dexmedetomidine; BMI: body mass index; ASA-PS: American Society of Anesthesiologists–physical status; NYHA: New York Heart Association; IBD: inflammatory bowel disease; OGIB: obscure gastrointestinal bleeding.
Examination characteristics in MDZ group and DEX group before propensity score matching.

MDZ: midazolam; DEX: dexmedetomidine.
Adverse events
In the MDZ group, of 166 DBEs, 46 (27.7%) had body motion; 7 (1.2%), hypotension; 128 (77.1%), respiratory depression; and 6 (3.6%), bradycardia. There were three perforations, one pancreatitis, one bleeding, and one aspiration pneumonia.
In the DEX group, of 111 DBEs, 13 (11.7%) had body motions and 13 (11.7%) had hypotension. In 55 cases (49.5%), nasal oxygen was given due to decrease in SpO2 level, but no intubation was required. Bradycardia was seen in two cases (1.8%). Body motions were seen especially in peroral DBE. Eight (61.5%) of 13 were due to gag reflex during endoscope insertion. There were one pancreatitis and one aspiration pneumonia. The adverse events in each group are shown in Table 5.
Adverse events in MDZ group and DEX group before propensity score matching.
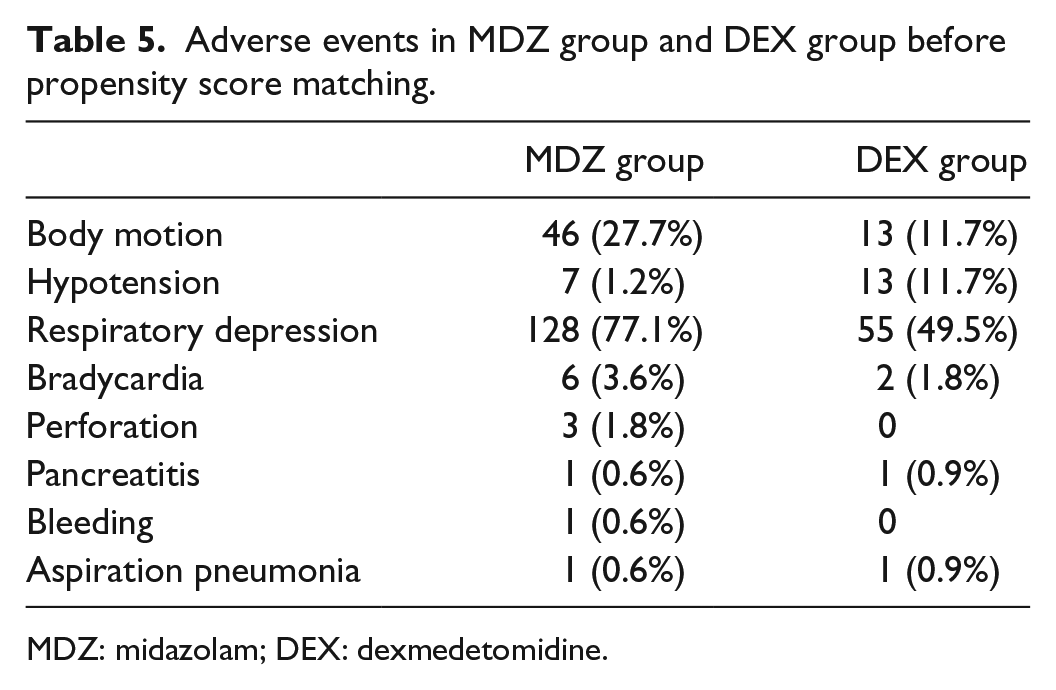
MDZ: midazolam; DEX: dexmedetomidine.
Propensity score matching
After propensity score matching, 182 cases (91 for each group) were selected. The patient and examination characteristics after propensity score matching are summarized in Tables 6 and 7, respectively. In the DEX group, there was less body motion and less respiratory depression. Hypotension and bradycardia were not significantly different in the two groups (Table 8).
Patient characteristics in MDZ group and DEX group after propensity score matching.

MDZ: midazolam; DEX: dexmedetomidine; BMI: body mass index; ASA-PS: American Society of Anesthesiologists–physical status; NYHA: New York Heart Association; IBD: inflammatory bowel disease; OGIB: obscure gastrointestinal bleeding.
Examination characteristics in MDZ group and DEX group after propensity score matching.

MDZ: midazolam; DEX: dexmedetomidine.
Comparison of adverse events in MDZ group and DEX group after propensity score matching.

MDZ: midazolam; DEX: dexmedetomidine.
Assessment of sedation
Most of the patients and endoscopists considered the state of sedation as satisfactory, but 16 (18%) patients rated it as unsatisfactory (Table 9). The patients’ scores were lower in those who had a recollection of the procedure (p < 0.001) (Table 10). The significant factors associated with endoscopists’ scores were histories of surgery (p = 0.042) and scale of body movement during DBE (p = 0.018) (Table 11).
Assessment of sedation using a 5-point Likert scale.

Analysis of patients’ satisfaction for sedation in DEX group.

MDZ: midazolam; DEX: dexmedetomidine; BMI: body mass index; CI: confidence interval.
Analysis of doctors’ satisfaction for sedation in DEX group.
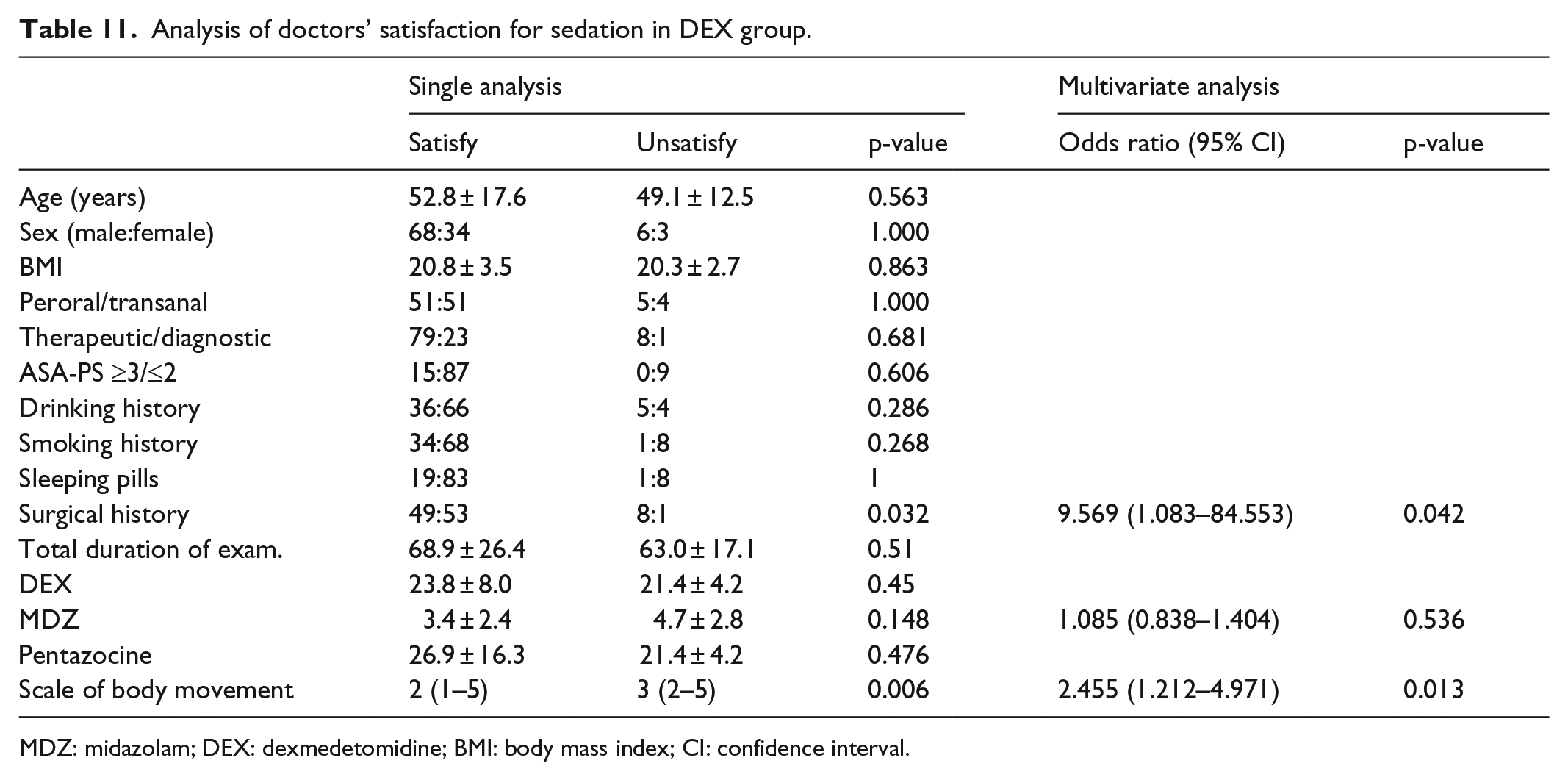
MDZ: midazolam; DEX: dexmedetomidine; BMI: body mass index; CI: confidence interval.
Discussion
The sedative action of DEX, which is an α2-adrenergic agonist, is through the inhibition of firing of the locus ceruleus of the brain stem, whereas MDZ and propofol are γ-aminobutyric acid (GABA) receptor agonist medications in central nerves system. This unique sedative activity is thus unlikely to cause restlessness or respiratory suppression such as that seen with GABA receptor agonists; however, excessive use of DEX has been reported to cause hypotension and bradycardia. 14 Although DEX cannot be used for bolus injection, when more rapid deep sedation is needed, another sedative such as MDZ and propofol are needed.
In this study, there were significantly less body motion and respiratory depression in the DEX group than in the MDZ group, but hypotension and bradycardia were not significantly different in the two groups. We used body motion as the primary endpoint because it might cause severe adverse events such as perforations. In fact, three patients in the MDZ group who had perforations had violent body motions during DBE. Therefore, sedation using DEX can contribute to a safer DBE procedure with reduction in body motion and respiratory depression.
In our hospital, the average MDZ dose in the MDZ group was 15.6 ± 5.8 mg, which was higher than that used in another study. 15 Among the patients who underwent DBE in our hospital, around 40% had CD, more than half had a history of surgery, and the median age was 52 years (Table 2). However, in the study of Möschler et al., 15 most of the patients had suspected obscure gastrointestinal bleeding (OGIB), 11% had a history of surgery, and the median age was 64 years. MDZ clearance decreased with increasing age. 16 Insertion of DBE was significantly influenced by a history of abdominopelvic surgery. 17 These might affect the MDZ dose.
We used moderate-to-deep sedation during peroral and transanal DBEs, but opinions differ on the optimum depth of sedation. Peroral DBEs sometimes require deep sedation or general anesthesia to avoid or control pain.3,18 To avoid the gag reflex, which often causes body motions, deeper sedation may be given.
Most of the patients were satisfied with the level of sedation. However, because DEX has no amnesic action, patients often had recollection of any discomfort associated with the examination. 19 In fact, 15 (93.8%) of the 16 unsatisfied patients had recollection of the procedure. Amnesic action may be an advantage in patients undergoing painful surgery. 20 To improve patient satisfaction, the dose of benzodiazepine, which has amnesic action, should be increased.
However, this study has some limitations. First, the propensity score matching does not account for unmeasured confounders, unlike in a randomized controlled clinical trial. In this study, the propensity score was adjusted by the significant factors of each adverse event in each group. These factors were also reported by the other articles as risk factors.21–23 However, other articles reported on other risk factors, such as diabetes, which were not significant factors in this study. 24
Second, there was a difference in the measurement of anesthetic depth between the MDZ and the DEX groups. Although both RSS levels 3–5 (used in the MDZ group) and BIS 60-80 are equivalent to moderate or deep sedation, there are no reports that they are equal.11,25 BIS monitoring leads to higher patient and endoscopist satisfaction scores; thus, less adverse events in the DEX group might have been affected by BIS monitoring. 26 Finally, the criterion additional sedatives and analgesic differs between the MDZ and the DEX groups. This could have possibly led to the administration of a higher pentazocine dose in the DEX group. Sedation with DEX is effective for pain control and contributes to the lesser need for additional analgesic.27,28 A higher induction dose of pentazocine had led to stronger pain control in the DEX group, which might have caused less body motions. However, the amount of pentazocine was one of the main outcomes; therefore, it was impossible to match with propensity score matching. Regarding the number of times that additional administration of drugs was required in both groups, pentazocine was given on 1.0 ± 1.1 (median 1: 0–4) times and MDZ was given on 2.6 ± 1.4 (median 3: 0–7) times in DEX group. The exact additional amount of MDZ and the number of times for additional administration of drugs in MDZ group was unknown because of retrospective review.
Conclusion
DEX for conscious sedation in DBE may reduce body motion and respiratory depression compared to our previous records. Therefore, a prospective, randomized control trial using the same additional sedatives should be performed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the ethics committee of participating institution and was registered with a registry approved by the International Committee of Medical Journal Editors (UMIN ID000015785)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
The observational study on the safety of dexmedetomidine during double-balloon endoscopy was approved as 2014-0414 in research ethics committee of Nagoya University Graduate School of Medicine.