
Abstract
Objectives:
To study neonatal outcomes following buprenorphine/naloxone and methadone exposure during pregnancy.
Methods:
This study is a retrospective review of clinical and demographic information of 58 infants whose mothers were treated with buprenorphine/naloxone and 92 infants whose mothers were treated with methadone for opioid dependence during pregnancy.
Results:
Gestational age, birth weight, prematurity, admission to neonatal intensive care unit, and length of stay were similar between both groups of infants. Neonatal abstinence syndrome occurred less frequently among infants of mothers treated with buprenorphine/naloxone than those treated with methadone (64% and 80%, respectively, p = 0.03). All infants with neonatal abstinence syndrome were treated postnatally with methadone. There was a trend toward shorter duration of treatment and lower cumulative dosages of methadone among the buprenorphine/naloxone–exposed infants.
Conclusions:
No apparent significant adverse neonatal outcomes were detected following treatment with either maintenance medication; however, further prospective research is necessary to examine the safety and efficacy of buprenorphine/naloxone in pregnancy and its effects on the neonate.
Introduction
Opioid dependence is an increasingly common problem during pregnancy.1–5 A 2010 national survey on drug use demonstrated that approximately 5% of pregnant women aged 15–44 years are illicit drug users.3,4,6–8 Over a 10-year time period, opioid use during pregnancy has increased approximately fivefold, while the rate of neonatal abstinence syndrome (NAS) has increased threefold.9,10 In the last 5 years, our institution has noted a 375% increase in the number of women seeking treatment for opioid dependency during pregnancy.
Withdrawal from opioids during pregnancy may result in preterm labor, fetal distress, and intrauterine fetal demise prompting American College of Obstetricians and Gynecologists (ACOG) and the American Academy of Pediatrics (AAP) to recommend maintenance pharmacotherapy during this period.3,4 Methadone has long been considered the gold standard for treatment during pregnancy.3,4,8,11 However, even this controlled approach can have serious consequences for the passively dependent infant. The reported incidence of NAS is highly variable; however, it has been estimated that up to 95% of infants exposed to opioids in utero experience withdrawal and that 50% require treatment, leading to prolonged hospital lengths of stay (LOS).1,4,5
Buprenorphine is an effective treatment for opioid dependence in the nonpregnant adult. 12 Multiple reports suggest that infants exposed to buprenorphine in utero are likely to experience a milder form of NAS compared to methadone-exposed infants.3,13–15 Recently, centers treating patients with opiate dependency have begun to use a combination buprenorphine/naloxone sublingual film (Suboxone™, Reckitt Benckiser Pharmaceuticals, Hull, United Kingdom) that may limit abuse potential. 12 The increased use and availability of this medication are likely to involve women of reproductive age. Unfortunately, there is limited data on the use of this medication during pregnancy and its effect on the neonate.16,17
Objective
The objective was to evaluate neonatal outcomes following in utero exposure to buprenorphine/naloxone or methadone for maternal opioid dependence. The primary outcome was to evaluate the number of neonates requiring NAS treatment. Secondary outcomes included duration of NAS treatment and the total cumulative dosage of methadone required.
Materials and methods
This study was a retrospective chart review of pregnant, opioid-dependent women and their neonates delivered at The Ohio State University Wexner Medical Center, between 1 January 2010 and 14 October 14 2011. The study was approved by The Ohio State University Institutional Review Board.
Women ≥18 years of age with a history of opioid dependence currently enrolled in a treatment program and stabilized on buprenorphine/naloxone or methadone were eligible for inclusion in the study. Selection of medical treatment with either medication was based on patient preference after consultation by an interdisciplinary medical team, including obstetricians (M.R.P.), clinical pharmacists (K.M.G., K.J.L., or D.K.G.), and social workers. Obesity was defined by a pre-pregnant body mass index (BMI) of 30–34.9 kg/m2 and morbid obesity by a BMI of ≥35 kg/m2. Upon arrival to labor and delivery, women’s feeding preference for their infants (breastfeeding (BF), formula feeding, or undecided) was ascertained by the nurse. Mothers were deemed eligible for BF if they had a negative urine toxicology screen for illicit substances at the time of delivery, no evidence of illicit drug use during the last trimester, and were HIV negative. BF was considered initiated if at the time of discharge from the hospital ≥50% of the infants’ feedings were direct from the breast or by expressed breast milk. 18 Maternal maintenance dosage was defined as the total daily dosage of buprenorphine/naloxone or methadone taken by the mother prior to delivery. Compliance with the prescribed treatment was measured by positive urine drug screen for that substance at the time of delivery. Urine drug screening for illicit substances (amphetamines, barbiturates, benzodiazepines, cocaine, nonprescribed methadone, other opiates, and marijuana) was also performed. Neither the patients acknowledged nor their medical or social history documented alcohol abuse during the pregnancy.
After delivery, neonates were evaluated for NAS based on a modified version of the Finnegan scale by trained neonatal nursing staff. 5 Regardless of the type of opioid medication prescribed during pregnancy, all infants who needed pharmacologic treatment for NAS received methadone. Treatment was initiated by 3 scores ≥8 or 2 scores ≥12 in a 24-h period. 19 Phenobarbital was the adjunctive medication of choice. Inpatient management was similar among all infants over the study period; however, a subgroup of infants were treated using a combined inpatient/outpatient NAS weaning protocol. 19 Cumulative methadone dose was defined as the total number of milligrams (mg) of methadone the infant received during inpatient hospitalization and if applicable, inpatient–outpatient combined treatment. Methadone to morphine equivalency was calculated based on previously published dosing recommendations. 20 Hospital LOS was calculated as the difference between day of admission (day of birth) and the day of hospital discharge.
Statistical analysis
Descriptive statistics were used to characterize maternal and infant populations. Comparisons between groups and subgroups of patients were made with Student’s t-test for continuous variables and chi square or Fisher’s Exact tests for categorical variables. Medians were compared using Wilcoxon rank sum. Significance was established at a p-value of ≤0.05.
Results
Our study population consisted of 150 women receiving maintenance treatment for opioid dependence (58 treated with buprenorphine/naloxone and 92 with methadone) and their infants. One hundred forty-five (97%) of the women were (white), 4 (3%) African American, and 1 (1%) Hispanic. Educational levels varied and were reported to be as follows: 48 (32%) ≤11th grade, 58 (32%) completed high school, and 38 (30%) had some college experience. In the study, 99% of the pregnancies were singletons. The one twin pregnancy was dichorionic–diamniotic. While 23% of the women were obese, 15% were morbidly obese. A total of 39 persons had hepatitis C, 1 had hepatitis B, and 1 was HIV positive. In all, 12 (8%) women had history of asthma and 7 (5%) had herpes simplex virus (HSV) infection. Depression, the most common psychiatric condition, affected 24 (16%) patients. Upon arrival to labor and delivery, 59 (39%) of the 150 women intended to breastfeed, 76 (51%) intended to feed formula, whereas the remaining 15 (10%) were undecided. Of the 150 deliveries, 40 (26%) were cesarean, of which 22 (55%) were repeat operations. Common indications for the 18 primary cesarean deliveries included failure of labor to progress, breech presentation, and fetal distress. All mothers and their infants survived.
Comparison of the clinical and demographic characteristics of the women treated with buprenorphine/naloxone and methadone are presented in Table 1. Both groups of women were similar except that a higher percentage of women in the buprenorphine/naloxone group reported nicotine use (86% vs 75%, respectively, p = 0.02) and benzodiazepine use (9% vs 1%, respectively, p = 0.03). The mean maintenance dose at the time of delivery in methadone equivalents was 125 ± 45 mg for the buprenorphine/naloxone group versus 101 ± 41 mg for the methadone group (p = 0.01). Duration of treatment prior to delivery was similar between groups, with a median of 4 months in the buprenorphine/naloxone group (range = 1–27) and 4 months in the methadone group (range = 1–15) (p = 0.57). Based on urine toxicology data, compliance with the prescribed medication was high for those on buprenorphine/naloxone (86%) and almost universal for those on methadone (99%). The number of urine tests positive for illicit substances was higher for women treated with buprenorphine/naloxone than for those treated with methadone (47% vs 22%, respectively, p = 0.01). Among women treated with buprenorphine/naloxone, 6 tested positive for benzodiazepines, 5 for marijuana, 4 for opiates, 2 for amphetamines, 1 for cocaine, and 2 for multiple substances. Similarly, for women treated with methadone, 4 tested positive for benzodiazepines, 3 for marijuana, 6 for opiates, 1 for cocaine, and 3 for multiple substances.
Maternal demographic and clinical characteristics.
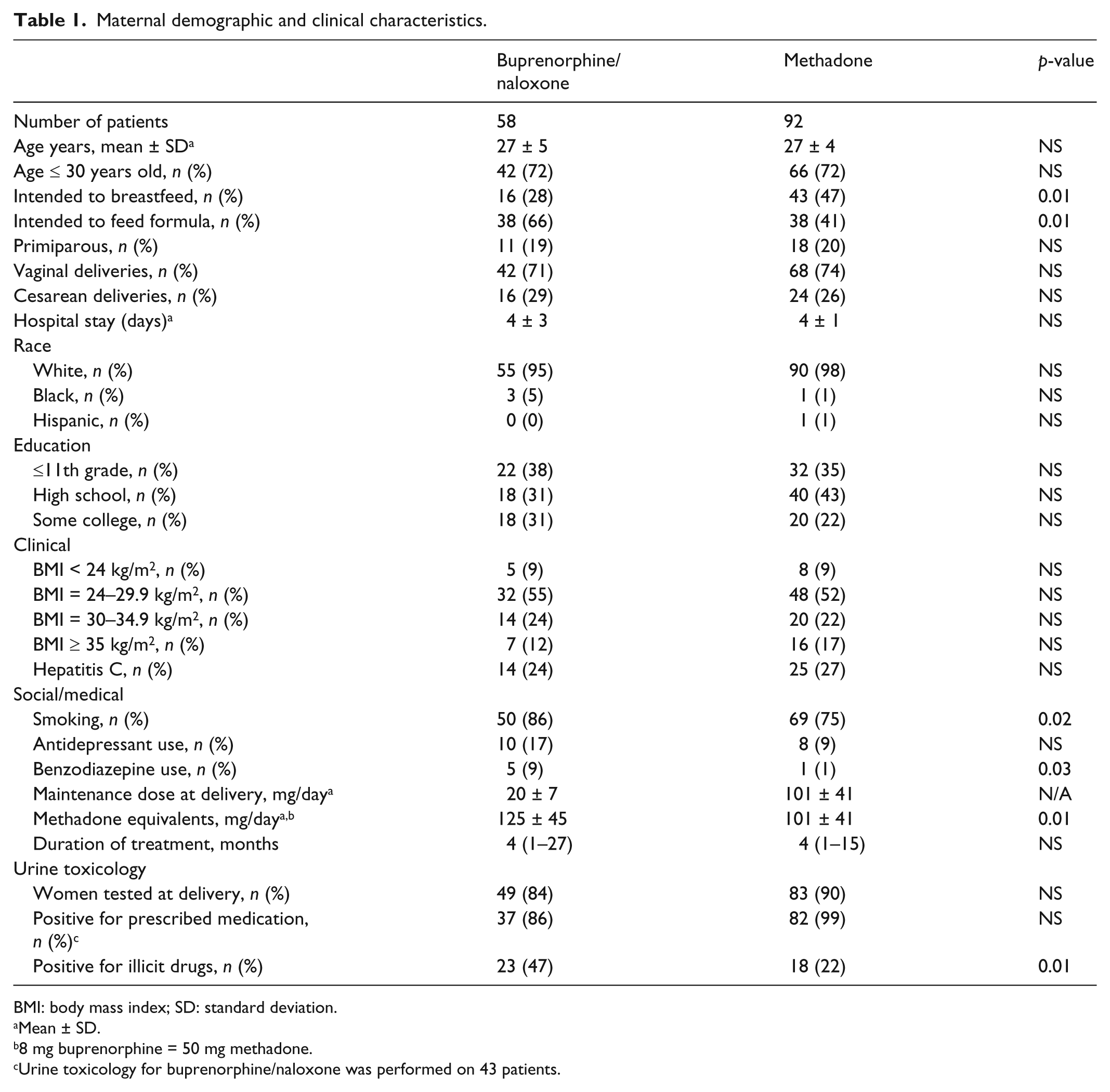
BMI: body mass index; SD: standard deviation.
Mean ± SD.
8 mg buprenorphine = 50 mg methadone.
Urine toxicology for buprenorphine/naloxone was performed on 43 patients.
Baseline neonatal characteristics are outlined in Table 2. Except for BF initiation, there were no significant differences between the groups. A total of 25% of the buprenorphine/naloxone–exposed infants and 20% of the methadone-exposed cohort were admitted to the neonatal intensive care unit (NICU), whereas the remaining infants were admitted to the well baby nursery (WBN) for observation and/or treatment. The most common diagnosis on NICU admission was respiratory distress, which affected 23 of the 33 (75%) infants. One infant was mechanically ventilated for 2 days, while the remaining 22 (all diagnosed with transient tachypnea of the newborn) required nasal continuous positive airway pressure (CPAP) and/or oxygen for a short time. A total of 7 infants were admitted to NICU due to problems related to prematurity, and the remaining 3 infants due to miscellaneous causes. On arrival to labor and delivery, 16 of 58 (28%) women treated with buprenorphine/naloxone and 43 of 92 (47%) treated with methadone intended to breastfeed. At the time of their infant’s discharge, only 17% and 45%, respectively, had initiated BF. All these differences were statistically significant.
Neonatal baseline characteristics.

GA: Gestational age; NICU: neonatal intensive care unit; SD: standard deviation.
Mean ± SD.
Clinical outcomes of neonates according to maternal treatment are presented in Table 3. A total of 90 of the 117 (77%) infants originally admitted to the WBN and 21 of the 33 (64%) admitted to NICU required treatment for NAS. The number of infants requiring treatment for NAS was lower in the buprenorphine/naloxone–exposed group as compared to those exposed to methadone prenatally (64% vs. 80%, respectively, p = 0.03). Infants exposed to buprenorphine/naloxone had a lower oral morphine equivalent requirement than the infants exposed to methadone in utero (21 ± 14 mg vs. 28 ± 14 mg). Duration of NAS treatment was 6 days shorter in the buprenorphine/naloxone group at 32 ± 21 days as compared to 38 ± 21 days in the methadone group. Although not statistically significant, there was a trend toward shorter treatment duration and lower cumulative methadone levels in the buprenorphine/naloxone–exposed group. Also, 7% of infants in the buprenorphine/naloxone group required phenobarbital compared to 5% in the methadone group. A similar number of infants in both groups were treated using a combined inpatient/outpatient NAS weaning protocol. One patient in the buprenorphine/naloxone group had to be readmitted to the hospital for treatment of withdrawal.
Neonatal outcomes as related to mothers opiate maintenance medications.

NAS: neonatal abstinence syndrome; SD: standard deviation.
Mean ± SD.
1 mg methadone = 4 mg morphine sulfate. 20
Discussion
Methadone has been the preferred maintenance therapy for opioid dependence during pregnancy since the 1970s. Recently, however, many institutions have begun using buprenorphine for opioid maintenance due to reports of a milder NAS syndrome.2,13,14,21–24 A recent prospective, randomized controlled trial evaluating 131 infants exposed to buprenorphine or methadone found that 47% of buprenorphine-exposed infants required treatment for NAS compared to 57% of methadone-exposed infants (p = 0.26). Additionally, infants exposed to buprenorphine required significantly less oral morphine (1.1 mg vs. 10.4 mg, respectively, p < 0.01), and had a significantly shorter duration of NAS treatment (4.1 days vs. 9.9 days, respectively, p < 0.01) compared to methadone. 14 Based on mounting clinical evidence, experts recognized buprenorphine as a safe and effective alternative to methadone therapy for opioid dependence during pregnancy.13–15
At our institution, buprenorphine/naloxone are prescribed over the single-entity buprenorphine formulation. Like others, we believe the combination product offers multiple advantages, namely, the presence of the mu-opioid antagonist naloxone, which limits abuse potential.12,16,17 If taken parenterally, naloxone induces rapid withdrawal; however, if taken sublingually, naloxone has poor bioavailability. 25 Therefore, this combination product should not cause additional concerns during pregnancy compared to single-entity buprenorphine.25,26
This study evaluated neonatal outcomes following in utero exposure to buprenorphine/naloxone or methadone for maternal opioid dependence. We observed a lower incidence of NAS following buprenorphine/naloxone exposure compared to methadone exposure. Furthermore, there was a trend toward shorter treatment duration and lower cumulative methadone dose in those infants exposed to buprenorphine/naloxone despite higher illicit substance use measured by urine toxicology at the time of delivery in the group exposed to buprenorphine/naloxone. Unfortunately, there is no comparative data available since the only study reporting on infants exposed to buprenorphine/naloxone in utero involved only 10 mothers and their infants. 16 In that study, women received the combination product at a maximum dose of 16 mg buprenorphine component. None of the women in this cohort had positive drug screens for illicit substances at delivery. Four of the neonates (40%) required treatment for NAS with a mean dose of 3.5 mg oral morphine. NAS-associated hospitalization was approximately 7 days.16,17 The present report expands the number of infants exposed to this medication, and provides for the first time a comparison of neonatal outcomes with those of infants exposed in utero to methadone.
The incidence of NAS following methadone exposure reported here is somewhat higher than that reported by others.13–15 On the other hand, the occurrence of NAS among infants exposed to buprenorphine/naloxone is similar to that reported following exposure to buprenorphine alone.14–17 With regard to the treatment of NAS, like others, we noted a lower duration of treatment and consequently, a lower cumulative morphine equivalent dosage.13–17
Evidence suggests that maintenance therapy with buprenorphine or methadone at recommended doses results in a minimal amount of drug transfer via breast milk that poses no harm to the BF infant.25,27 BF initiation rates for the methadone-treated women observed here are similar to that reported elsewhere.19,27 Prior to our study, information regarding BF during buprenorphine/naloxone treatment was limited to three women reported by Debelak et al. 16 and Lund et al. 17 The low BF initiation rate among buprenorphine/naloxone–treated mothers seems to relate to the low intention to breastfeed declared by them upon arrival to labor and delivery. After all, intention to breastfeed is considered the strongest predictor of BF initiation. 18
In summary, this retrospective evaluation of neonatal outcomes following buprenorphine/naloxone and methadone therapy for opioid dependence during pregnancy demonstrated a lower incidence of NAS among infants exposed to buprenorphine/naloxone. Additionally, there was a trend toward decreased duration of NAS treatment and lower cumulative dose of morphine equivalents in the cohort exposed to buprenorphine/naloxone. Further research is needed to determine the safety and efficacy of buprenorphine/naloxone use in pregnancy and its effect on the neonate.
Footnotes
Declaration of conflicting interests
The authors report no conflict of interest.
Funding
No funding/financial support was provided for this work.