
Abstract
Objectives:
Measures of pregnancy associated deaths provide important guidance for public health initiatives. Record linkage studies have significantly improved identification of deaths associated with childbirth but relatively few have also examined deaths associated with pregnancy loss even though higher rates of maternal death have been associated with the latter. Following PRISMA guidelines we undertook a systematic review of record linkage studies examining the relative mortality risks associated with pregnancy loss to develop a narrative synthesis, a meta-analysis, and to identify research opportunities.
Methods:
MEDLINE and SCOPUS were searched in July 2015 using combinations of: mortality, maternal death, record linkage, linked records, pregnancy associated mortality, and pregnancy associated death to identify papers using linkage of death certificates to independent records identifying pregnancy outcomes. Additional studies were identified by examining all citations for relevant studies.
Results:
Of 989 studies, 11 studies from three countries reported mortality rates associated with termination of pregnancy, miscarriage or failed pregnancy. Within a year of their pregnancy outcomes, women experiencing a pregnancy loss are over twice as likely to die compared to women giving birth. The heightened risk is apparent within 180 days and remains elevated for many years. There is a dose effect, with exposure to each pregnancy loss associated with increasing risk of death. Higher rates of death from suicide, accidents, homicide and some natural causes, such as circulatory diseases, may be from elevated stress and risk taking behaviors.
Conclusions:
Both miscarriage and termination of pregnancy are markers for reduced life expectancy. This association should inform research and new public health initiatives including screening and interventions for patients exhibiting known risk factors.
Keywords
Introduction
Maternal deaths associated with pregnancy are a major public health concern. Death rate calculations based on death certificates alone, however, consistently miss cases due to the fact that registrars often lack information about the deceased’s woman’s complete pregnancy history. This problem can be alleviated in part by linking death certificates to birth certificates, fetal death records, termination of pregnancy (TOP) registries, and medical treatment records.
Without such record linkage only 26% of deaths during pregnancy or after live birth or stillbirth would have been identified from the death registry or death certificates alone, according to a Finnish study. 1 Using death certificates alone, only 12% of deaths following miscarriage or ectopic pregnancy and just 1% of deaths following termination of pregnancy (TOP) could be identified without record linkage. 1 The importance of systematically using record linkage to identify deaths associated with pregnancy losses (TOP, miscarriage, and ectopic pregnancies) is further demonstrated by the same study’s findings, which demonstrate that the mortality rate in the year following a pregnancy loss was two to four times higher than that of delivering women.
Record linkage studies are therefore clearly necessary to properly identify the effects of pregnancy on the health and longevity of women. This methodology is especially important to understanding mortality rates associated with TOP and natural pregnancy losses precisely because such deaths are (a) much more common than deaths during pregnancy or after delivery, and (b) less likely to be identified on death certificates alone. 1
Compared to women who deliver, those who miscarry or have TOP face significantly elevated rates of psychiatric disorders,2–10 substance use,5,6,10–13 suicidal behaviors,5,6,13–16 sleep disorders, 17 post-traumatic stress disorders,7,18,19 a decline in general health, 20 and elevated rates of recourse to medical treatments in general,21,22 most of which have been observed within the first through ten years following the pregnancy loss. Any and all of the aforementioned conditions may shorten longevity. It is therefore especially important from a public health and economic viewpoint to improve investigations regarding the mortality rates associated with pregnancy losses.
While the importance of research on maternal mortality is widely recognized, it has appeared increasingly evident to the authors that insufficient attention has been devoted to examining the subset of women’s deaths following pregnancy losses. Greater insight into this subset of deaths may help to guide and prioritize the development of proactive health initiatives that can save women’s lives and improve health.
Therefore, the authors identified the need for a systematic review which would provide (a) a description and synthesis of all the available qualifying literature, including proposals for research priorities and actionable interventions based on the best available evidence, and (b) a quantitative meta-analysis of the available evidence. To meet these goals, we determined that we should first seek to identify all record linkage studies examining mortality rates associated with pregnancy outcome regardless, without any limitation on time frame. This initial assessment would help us to identify any missed opportunities for examining pregnancy loss associated mortality. Second, we seek to identify all record linkage studies that have specifically examined death rates associated with pregnancy losses, including voluntary and therapeutic terminations. Using this subset of studies, we would then (a) develop a narrative synthesis of the common and specific findings of the relevant studies and (b) undertake a meta-analysis of any comparative mortality rates associated with different pregnancy outcomes which are appropriate to the methods of meta-analyses.
The importance of this investigation is underscored by numerous studies which have found that that parity and the exposure to various pregnancy outcomes has significant effects on life expectancy.23–25 Record linkage studies examining pregnancy associated life expectancy are needed to help to identify how the number of pregnancies, number of deliveries, and types of pregnancy outcomes may affect the health and longevity of women. These findings, in turn, may then contribute to better screening to identify the subsets of women who may most benefit from interventions to ameliorate any harmful effects and/or to enhance any beneficial effects associated with pregnancy and pregnancy management.
Definitions
Pregnancy loss, as used herein, includes all pregnancy outcomes that do not end in a live birth. 2
Natural loss is a subset that includes all pregnancy losses except TOP. While the vast majority of natural losses are miscarriages, it should be noted that some researchers have chosen to report only on miscarriages while others have included ectopic pregnancies, still births and other natural losses together. Still other investigators have grouped women who had stillbirths with women who had live births since these pregnancies continued to term or near term. 1
Pregnancy associated death, has been defined by the American College of Obstetricians and Gynecologists (ACOG) and the United States’ Centers for Disease Control (CDC) to include all deaths during pregnancy or within one year of a pregnancy outcome regardless of presumed cause of death. 26 The identification of pregnancy associated deaths has been recognized is an important precursor to efforts to identify maternal deaths, which are defined to include only those deaths for which there is a medical opinion that some aspect of the pregnancy or pregnancy management was a contributing cause of death. 26
Pregnancy associated long-term mortality is defined to include all deaths following one or more pregnancy outcomes without an imposed time limit. While the time limits used in each study reporting pregnancy associated long-term mortality should always be noted, this definition avoids establishing any arbitrary time limits and prepares the way toward calculating pregnancy associated mortality and life expectancy rates relative to variables such as gravidity, parity, live births, and exposure to pregnancy losses.
Abortion related deaths are defined by the CDC as any “death from a direct complication of an [induced] abortion (legal or illegal), an indirect complication caused by a chain of events initiated by an abortion, or an aggravation of a preexisting condition by the physiologic or psychologic effects of abortion.” 27 The deliberate choice to place no time limit on the definition of TOP related deaths reflects the fact that there is no clear temporal limit on physiological and psychological effects that may contribute to subsequent death.
TOP associated deaths (or abortion associated deaths) are herein defined as the subset of pregnancy associated deaths which are within one year of a TOP. The one year limit corresponds to that for “pregnancy associated deaths.”
TOP associated long-term mortality is an extension of the CDC’s “abortion related deaths” and include all deaths among women with a history of TOP without regard to time. Just as the systematic identification of early and late maternal deaths must be preceded by a systematic identification of pregnancy history, so the identification of abortion related deaths should be preceded by the systematic identification of TOP history without a predefined time limit.
Materials and methods
PRISMA guidelines were consulted and employed where appropriate in the development and writing of this review.
Eligibility criteria
The first level of predefined eligibility criteria were: (1) the study was available in English; (2) the study examined mortality rates of women relative to one or more pregnancy outcomes; and (3) the study included systematic linking of death certificates to independent records used to identify if the deceased had one or more pregnancy outcomes within a year of her death. The independent records might be one of the following: birth certificates, fetal death certificates, TOP registries, paid insurance claims, or comprehensive hospital or medical records documenting treatments related to pregnancy.
The second level of eligibility criteria was to identify all publications meeting the first level of inclusion criteria which reported on death rates associated with any form of pregnancy loss (miscarriage, legal TOP, ectopic pregnancy, still birth, or any other failed pregnancy) as identified through records independent of the death certificates. This step eliminated studies that examined only mortality rates associated with childbirth, or which failed to distinguish between deaths associated with childbirth and pregnancy loss. This step helped to both identify missed research opportunities and to identify the eligible studies which do have information regarding mortality rates associated with pregnancy loss but failed to report this data.
The third step was to identify studies eligible for inclusion in a meta-analysis. This subset was drawn from the list of studies meeting the second level of eligibility. This third level of eligible studies included only those that (a) report mortality rates within one year for all three pregnancy outcomes of interest (childbirth, natural losses, and TOP) and (b) provided the most recently relevant data, thereby excluding duplication of results when the same population of women were examined in more than one study.
Information sources and search terms
In July of 2015, a SCOPUS search was conducted using the search ( ( ( TITLE-ABS-KEY ( maternal mortality ) OR TITLE-ABS-KEY ( maternal death ) ) ) AND ( ( TITLE-ABS-KEY ( record linkage ) OR TITLE-ABS-KEY ( linked records ) ) ) ) OR ( ( ( TITLE-ABS-KEY ( pregnancy associated mortality ) OR TITLE-ABS-KEY ( pregnancy associated death ) ) ) AND ( ( TITLE-ABS-KEY ( record linkage ) OR TITLE-ABS-KEY ( linked records ) ) ) ). A total of 458 records of potential interest was returned.
A MEDLINE search was conducted using the search ((“pregnancy associated mortality” OR “pregnancy associated death”) AND (“record linkage” OR “linked records”)) OR ((“record linkage” OR “linked records”) AND (“maternal mortality” OR “maternal death”)). This search returned 20 references.
Additional candidates were identified using the “snowball method,” the review of all references cited by eligible papers plus citations from other maternal mortality reviews.
Study selection
After elimination of duplicates, all titles and abstracts were examined to identify publications with a prospect for meeting the predefined inclusion criteria. Those deemed candidates for inclusion were retrieved for full text review and studied to determine which articles met the pre-determined inclusion criteria. Assessments of those studies qualifying for both levels of inclusion criteria were conducted by two reviewers, with disagreements resolved by discussion.
Risk of bias
Studies qualifying for both levels of inclusion were scored for bias using the Newcastle-Ottawa Quality Assessment Scale (NOQAS) for cohort studies.
Data collection for descriptive summary of literature
Each study meeting the second level of eligibility was entered into a table identifying the source, population size, time period examined, types of pregnancy outcomes examined, means of identifying deaths and pregnancy outcomes, any confounding variables that were examined in the study, NOQAS score, and a summary of major findings. The table was completed by two reviewers, with disagreements resolved by discussion.
Data collection for meta analysis
To calculate the age adjusted number of deaths in the first year for each subgroup’s population for our meta-analysis we extracted data relative to the reported age adjusted risk of death during the first year following the pregnancy outcome from each country. To avoid duplication of cases, only the most recent study for each country was used in the meta-analysis. Using the age adjusted mortality rate of delivering women as the control in each case, odds ratios and confidence limits for each subgroup (TOP vs birth, and natural losses vs birth) and for each study were calculated using EpiInfo 7’s StatCalc. These results were then entered into the Comprehensive Meta Analysis software package to produce results using the fixed effects model.
Results
After removal of duplicates, a total of 989 titles were identified by the combination of search terms and review of additional references (Figure 1). Review of abstracts eliminated 904 references. At the second level of review, 14 more were eliminated after full text review because they did not identify pregnancy history using record linkage. Three non-English studies were also identified, but their abstracts indicated that none included data on pregnancy loss associated mortality so English translations were not sought. Thus, a total of 17 studies were eliminated at this stage.

Flow chart of search results, reasons for exclusion, and three levels of inclusion.
A total of 68 studies examining populations in 11 countries met the criteria for the first level of eligibility. All of the studies identified significantly more maternal deaths than would have been identified by reliance on death certificates alone.
Of the 68 studies identified, 57 included record linkage of only birth and death records. In other words, they lacked any data on deaths associated with pregnancy losses. The distribution by country of these studies was as follows: one in Bangladesh, 28 one in Brazil, 29 two in Canada,30,31 one in Denmark, 32 one in Italy, 33 three in Netherlands,34–36 four in Sweden,37–39 one in Taiwan, 40 six in the United Kingdom,41–46 thirty-four in the United States including Puerto Rico,47–79 and three reporting data from multiple countries for which at least one country’s data used record linkage which met our criteria for inclusion.80–82
The remaining 11 studies met the criteria for the second level of eligibility: reporting results of linkage of death certificates to independent records of pregnancy loss. These included seven studies from Finland,1,83–88 two from Denmark,89,90 and two from the United States.91,92 Two of these investigated only deaths in the year following TOP.88,91 The remainder investigated pregnancy associated deaths and/or pregnancy associated long-term mortality relative to both birth and pregnancy loss.
Details of the eleven studies are summarized in Table 1. The column labelled “Confounding Variables Examined” identifies factors which were either (a) controlled for statistically, such as was commonly done in regard to age of the woman, or (b) controlled for by study design, such as restriction of the population to only the lowest economic class, or exclusion of women with prior psychiatric history, or (c) controlled for by showing segregated results for discrete groups, such as married and unmarried. The NOQAS assessment revealed that quality of these studies was very high, with low risk of bias. With a possible range from 0-9, (high corresponding to the highest quality) only the one very earliest study scored below 8.
Record linkage studies examining deaths associated with one or more types of pregnancy loss with notes regarding key findings.
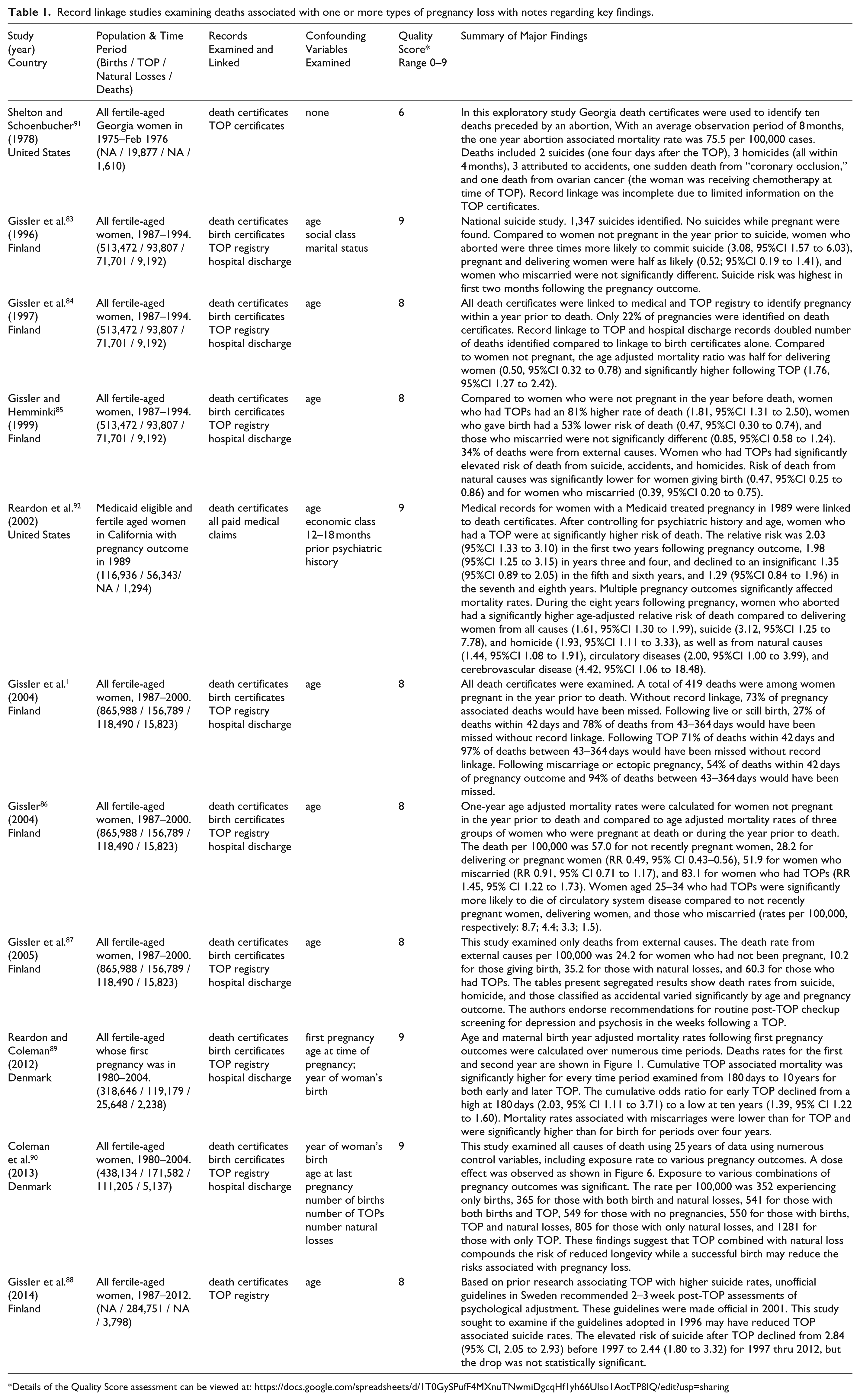
Details of the Quality Score assessment can be viewed at: https://docs.google.com/spreadsheets/d/1T0GySPufF4MXnuTNwmiDgcqHf1yh66Ulso1AotTP8IQ/edit?usp=sharing
Figure 2 shows the mortality rate per 100,000 person years for each outcome reported by the latest studies from each of Finland, Denmark, and the United States, showing cumulative mortality rates for both one year and two years. The graph illustrates that mortality rates remain elevated after pregnancy loss beyond one year. Notably, the mortality rate over two years, comparing results from Denmark and California, suggest that low income women are at higher risk but that socioeconomic effects do not fully explain the results. Alternatively, the difference may be due to only first pregnancies being examined in the Denmark study.

Cumulative Age Adjusted, All Cause Mortality Rates per 100,000 Women for One and Two Year Periods Following Pregnancy Outcome.
Figure 3 shows that the risk of death after pregnancy loss is most elevated in regard to deaths from external causes: suicide, homicide, and accidents compared to both delivering women and women who have not recently been pregnant.87,92 The implication that psychological effects associated with pregnancy loss may contribute to deaths resulting from self-destructive or risk taking behavior is further supported by a finding of higher rates of death attributed to mental illness (RR = 3.21, 94% CI 1.11–9.27) following TOP, even after controlling for prior psychiatric history. 92

Cumulative Age Adjusted, Violent Cause Mortality Rates per 100,000 Women for One and Two Year Periods Following Pregnancy Outcome.
As several the eleven studies undertook examined associations from a different perspective, a summary of their most important findings, including figures illustrating many of these findings, is provided below:
Pregnancy loss associated mortality may be over twice that of birth associated mortality. 1 TOP associated mortality is higher than miscarriage associated mortality, which is higher than pregnancy and delivery associated mortality. (Figure 2)
TOP associated mortality rates are higher than birth associated mortality during the first 180 days 89 and remains higher for six or more years.89,90,92 (Figure 4)
Differences in pregnancy associated life expectancy vary according to the type and number of exposures to various outcomes. Successful deliveries may mitigate some of the effects of pregnancy loss.90,92 (Figure 5)
There is a dose effect, whereby exposure to multiple pregnancy losses increases the negative effect on life expectancy whereas multiple births increases life expectancy. 90 (Figure 6)
The risk of death associated with pregnancy loss remains elevated even after controlling for psychological differences and economic class. 92 (Figure 2)
While the risk of death after pregnancy loss is most elevated in regard to deaths from violent causes,87,92 there is also evidence that when risk of death after pregnancy loss is tracked beyond one year a significant higher risk is also associated with specific causes of natural death, such as circulatory disease (RR = 2.87, 95% CI 1.68–4.89) 92

Death rates following first pregnancy outcome through 180 days and during each of the first through tenth years after pregnancy outcome.

Adjusted odds ratios for pregnancy associated long-term mortality by exposure to types of pregnancy outcomes. Adjusting for age at last pregnancy and number of pregnancies.

Adjusted Odds Ratios for Pregnancy Associated Long Term Mortality Rates by Frequency of Exposure to Each Pregnancy Outcome—Denmark 1980–2004.
The meta-analysis used age adjusted mortality rates for each pregnancy outcome reported in most recent studies of the population of Finland 86 and Denmark. 89 While the eleven studies included data on women in three countries, neither American study reported age adjusted mortality rates for the first year after pregnancy outcome.
Figure 7 shows results of the meta-analysis using the fixed effects model. It illustrates the comparative risk of death in the first year after TOP compared to delivery and for the first year after natural losses compared to delivery. The risk of death during pregnancy and one year after a delivery the age adjusted pregnancy associated risk of death was 170 percent higher following a TOP (RR = 2.705; 2.243 < 95% CI < 3.263), and 84 percent higher following natural losses (RR = 1.843; 1.420 < 95% CI < 2.392). For all pregnancy losses compared to delivery, the risk was 137% higher (RR = 2.374; 2.038 < 95% < 2.764; Q-value = 8.220, P = .042). The I 2 statistic indicates that about 63% of the variation in the overall results is due to heterogeneity rather than chance.

Meta-Analysis of Age Adjusted One Year Mortality Rates Associated with Comparative Pregnancy Outcomes.
Discussion
Our systematic review found 68 studies employing record linkage of death certificates to independent records of pregnancy and pregnancy outcomes. In nearly every case, the authors reported that record linkage significantly improved the identification of maternal deaths and pregnancy associated deaths compared to reliance on death certificates alone. We concur with the opinion that the direct and indirect effects of pregnancy on women’s mortality rates cannot be accurately accessed without record linkage between death certificates and other medical records. 1
This systematic review also revealed that every record linkage study examining mortality rates relative to different pregnancy outcomes has revealed that pregnancy loss is associated with a higher risk of death than childbirth. These studies also show that this elevated mortality risk persists over many years, is multiplied by repeat exposure to pregnancy loss, and may be reduced by successful deliveries. The quality of these eleven studies is very high, with all but the one earliest attempt scoring 8 or above on the NCQAS (with a range 0–9).
Overall, the meta-analysis revealed that pregnancy loss associated mortality is more than double that of delivery associated mortality. Notably, the Danish data used in the meta-analysis included only first pregnancy outcomes while the Finnish data included all pregnancy outcomes. This may explain the higher pregnancy loss mortality rate observed in the Finnish data since a significant portion of the Finnish subjects would have been exposed to multiple pregnancy losses for which a dose effect of increased mortality risk has been observed. 90
A disproportionate share of pregnancy loss associated deaths are due to suicides, accidents, or homicide.83,86,87,92 In case study reports from mental health professionals and surveys of women struggling with pregnancy loss issues heightened risk taking and self-destructive behaviors are reported which may contribute to rates of accidents and homicide, in addition to suicide. 93 Risk of death from accidents and homicide may also be impacted by the elevated risk of substance abuse associated with TOP.10–12 This hypothesis is supported by one U.K. study of pregnancy associated deaths that reported that 1 a major portion of accidental deaths were due to drug overdose, and 2 of eight women who died after being struck by cars as pedestrians, seven were drug users. 43 These findings underscore the importance of record linkage as a precursor to efforts to evaluate “abortion related deaths,” as defined by the CDC. 27
Strengths and weaknesses
A strength of the narrative portion of this review is that while only 11 of 68 record linkage studies of mortality rates associated with pregnancy included examination of deaths associated with pregnancy losses, these eleven examined a variety of different time frames and confounding variables, including economic class, marital status, age, number and types of prior pregnancy outcomes, and prior psychiatric history. At the same time, however, it is also a weakness that all of these confounding variable were not addressed in every study. The fact that all of these studies, despite variations, showed a consistent trend in findings indicates that the trend is a real one and is likely to replicated if applied to other populations.
Clearly, a priority of future research should examine a broader number of confounding variables across more populations to better understand the direct and indirect pathways and co-occurring risk factors that may guide future interventions. Future studies should seek to control for potential confounders including: income inequality, psychiatric history, access to medical care including birth control, intimate partner violence, intentionality of pregnancy, and level of maternal attachment to the pregnancy.
A major weakness of our meta-analysis is that data on mortality rates in the first year following pregnancy losses were only available from two countries, which highlights the failure of most researchers to address this issue. In addition, a minor weakness is that the Danish study included stillbirths in the natural loss grouping while in the Finnish study stillbirths were included in delivery category. Since the number of stillbirths were not reported, we could not adjust for this difference. But given the expected low number of stillbirths, this difference in categorization is very unlikely to have a major impact on the results. Another inconsistency is that all the studies from Finland included deaths during pregnancy in with deaths following a delivery (live or stillbirth), potentially adding nine months mortality risk to the one-year post-delivery mortality rate. This would tend to inflate deaths associated with delivery. Reporting deaths during pregnancy as a separate item would be preferable. These points highlight why more consistent classification standards would be helpful in future research.
In our opinion, any pregnancy that fails to produce a live birth should be treated as a pregnancy loss since there may be grief issues impacting future health. Rare cases of multiple gestations including both live birth and fetal loss are confounding and should be excluded from more general analyses or treated as a separate group.
Future research and missed opportunities
Unfortunately, many opportunities to investigate pregnancy associated mortality and long-term mortality have been missed, to date. Our literature review found that only 11 of 68 record linkage studies (and only 2 of 37 studies in the United States) explored mortality rates associated with pregnancy loss.
This oversight can and should be corrected. Even in countries without central TOP registries, such as exist in Finland and Denmark, exposure to TOP and miscarriage can be identified through medical records and insurance claims, as shown by researchers in the United Kingdom, 15 Canada, 22 and in the United States.91,92 Unfortunately, except for these rare exceptions, most of the leading investigations into pregnancy associated deaths in Canada, the United Kingdom and the USA have failed to use these same techniques to investigate deaths associated with TOP or miscarriage.
Another missed opportunity appears to have occurred in a study of Italian women 33 in which researchers report that they did, in fact, link death certificates to records of terminations and miscarriages, but unfortunately their published analyses failed to provide any breakdown of death rates relative to each pregnancy outcome. Our request for a breakdown of deaths associated with each type of pregnancy outcome was rejected.
The failure of so many studies to report on pregnancy loss associated deaths indicates that there may be a risk of reporting bias. For example, social, political, or academic sensitivities relative to efforts to promote legalization of safe abortion in developing countries may produce a bias against investigating and/or publishing findings that may show TOP is associated with an increase in mortality rates.94,95 On the other hand, even though such findings have been reported since at least 1997,83,84 there may also be lack of sufficient awareness among researchers regarding the elevated mortality rates associated with pregnancy loss. In either case, it is clear that in most countries where record linkage studies have been performed there are no structural obstacles to expanding record linkage studies to include pregnancy loss associated mortality. What is required is simply the academic and/or political will to undertake such investigations.
What is already sufficiently clear is that mortality rates and longevity are significantly affected by exposure to pregnancy losses, whether natural or induced. Therefore, in the interests of patients, future investigations into pregnancy associated mortality should all include efforts to identify and report on the comparative effects associated with prior exposure to TOP, miscarriage, and other natural losses. Such research is necessary to guide the development of better screening and treatment strategies for those subsets of women who may most benefit from targeted interventions.
Incidental or causal relationships?
As discussed above, termination of pregnancy remains a sensitive and politically charged issue, for both those who defend it as a fundamental woman’s right and those who oppose it for moral reasons. In our experience, these passions often inspire a hypercritical level of suspicion regarding any epidemiological findings which run counter to preconceived expectations.
For readers to access their own biases regarding this subject matter, simply imagine if our results were all reversed and the risk of death in the year following a TOP was half that associated with childbirth. Would the reader consider such reversed results more comfortable or more disturbing? Would such results provoke more confidence in the value of record linkage studies or more suspicion?
In either event, it is important to interpret these findings in as balanced a perspective as possible. Correlation does not prove causation. There may be common risk factors for pregnancy loss which explain the elevated risks. 96 Indeed, given the fact that a disproportionate number of deaths associated with prior pregnancy loss are due to suicide and accidents, it would appear that causal contribution would most likely be indirect and chiefly mediated by psychological effects which are known to occur among women who experience a pregnancy loss.2–10,17–19 Moreover, the finding that there pregnancy loss has a dose effect on increased risk of death 90 (Figure 6) strongly parallels the finding of pregnancy loss having a dose effect on increased risk of mental illness.2,5,13
But even if the elevated risks can be entirely explained by common risk factors, it is critically important to acknowledge that these findings are still clinically relevant and very useful. Why?
Because a history of pregnancy loss is at least a useful marker for identifying women who may need additional screening, counselling and care. Therefore, alert clinicians can and should screen for a history of pregnancy loss in order to use this actionable information as detailed in our clinical recommendations below. How this marker may be used to provide better screening and referrals will be discussed more fully in the next section.
Additional support for a causal interpretation is found in studies which have identified the first onset of psychological problems, such as sleep disorders 17 or substance abuse, 97 soon after a pregnancy loss among women who did not previously have these problems. 13 Another important study examined hospital admission rates for attempted suicide rates prior to pregnancy and after a TOP 15 and revealed a significant and dramatic shift from a “normal” rate of suicide attempts to an elevated rate after TOP, as seen in Figure 8. These findings led the researchers to conclude that “the increased risk of suicide after an induced abortion may therefore be a consequence of the procedure itself.”

Rate of treatments for attempted suicide before and after delivery or TOP.
Another factor to consider regarding the question of causality is that negative effects may be substantially limited to small subgroups of women who are at greater risk. For example, experts on “both sides” of the legal abortion controversy are actually in agreement regarding the evidence that women who feel coerced or pressured into unwanted TOP are at greater risk of serious complications, including elevated self-destructive tendencies. 98 If we were to hypothesize, then, that all of the elevated risk of death associated with TOP reported in the studies we examined are limited to cases of coerced TOP, it would then follow that the findings reported herein may be an indirect measure of the frequency of coerced TOP. Such a conclusion would only further underscore the importance of the clinical recommendations offered in the next section.
Perhaps the most powerful evidence that pregnancy loss contributes directly to mental health problems is the frequency with which self-aware, introspective women specifically attribute the onset or worsening of substance use, depression, flashbacks, sexual dysfunction, self-destructive tendencies and other issues to their pregnancy loss experiences.93,99,100 These self-assessments are further validated by therapists treating women for pregnancy loss related issues.101,102 Additionally, evidence that post-abortion counselling programs reduce symptoms of psychological illness 103 also support the hypothesis that TOP can trigger or exacerbate psychological illness; after all, an effective treatment is evidence for an accurate diagnosis.
We are not asserting that pregnancy loss is the sole cause of the elevated risk of death identified in these studies, but rather that there is ample evidence to believe pregnancy loss can be a contributing cause. The discussion above is therefore intended to emphasize the importance of research designed to better understand the causal pathways and co-occurring risk factors which can then be used to better identify women who may benefit from appropriate interventions.
Clinical recommendations
Clinician’s should be alert to the fact that a history of any pregnancy loss may impact many aspects of women’s lives. Prior pregnancy losses, voluntary or involuntary, are also sensitive issues for many women which they may hesitate to dicuss. Therefore, it is highly recommended that as a standard intake question, or in periodic updating with patients, clinicians should make a gentle, non-judgmental query: “Have you had any pregnancy losses, like a miscarriage, abortion, or still birth?” This query, which non-judgmentally names each type of pregnancy loss, gives women permission to discuss any sensitive feelings regarding past pregnancy losses and also opens up opportunities to discuss any lingering or intermittent concerns.
When women do report a prior pregnancy loss, or for women considering a termination of pregnancy, we recommend that clinicians should then investigate if additional risk factors are present. Especially useful in this regard, at least 15 risk factors for more severe reactions following TOP which have been identified by American Psychological Association Task Force on Mental Health and Abortion. 104 With slight modification, these risk factors can also be applied to miscarriage and other natural losses. They are:
terminating a pregnancy that is wanted or meaningful
perceived pressure from others to terminate a pregnancy
perceived opposition to the abortion from partners, family, and/or friends
lack of perceived social support from others
various personality traits (e.g., low self-esteem, a pessimistic outlook, low-perceived control over life)
a history of mental health problems prior to the pregnancy
feelings of stigma; perceived need for secrecy
exposure to antiabortion picketing
use of avoidance and denial coping strategies
feelings of commitment to the pregnancy
ambivalence about the abortion decision
low perceived ability to cope with the abortion
history of prior abortion
late term abortion.
These risk factors can and should be used to identify women who may need more counselling and other services. Given the dose effects observed, screening for a history of pregnancy loss is especially important in preparing treatment plans for women in all subsequent pregnancies. Therefore, we recommend the APA identified screening criteria should be used on at least four occasions: (a) when women seeking mental health care report any history of pregnancy loss, (b) when women are seeking care in anticipation of becoming pregnant, (c) upon diagnosis of a pregnancy, and (d) before termination of a pregnancy.
Summary
Deaths associated with pregnancy, both within the first year and beyond, are significantly different relative to pregnancy outcome. Births have a positive effect on longevity while pregnancy losses have a negative effect, with negative effect of TOP being greater than that of natural losses. Multiple pregnancy losses are especially problematic. Pregnancy loss is at least a marker for adverse maternal outcomes, but is most likely a contributing risk factor driven by psychological stresses related to pregnancy loss.2–22
Many opportunities to investigate pregnancy loss associated long-term mortality rates have been missed. Future investigations into maternal mortality and pregnancy associated mortality should include systematic record linkage to medical and insurance records to identify pregnancy losses so that these patterns and risk factors can be better understood.
Screening for a history of pregnancy loss (induced or natural) is highly recommended as a means of identifying women who may benefit from additional counselling and interventions. Screening for risk factors associated with more psychological maladjustments following TOP, as identified by the APA, 104 is also highly recommended.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No grants or outside funding were used. David Reardon’s efforts were funded as part of his regular duties as Director of Research with the Elliot Institute. John Thorp’s efforts were not funded.
Ethical approval
Ethical approval was not sought for the present study because it is a literature review and does involve any original research using human or animal subjects.
Informed consent
Informed consent was not sought for the present study because it is a literature review and does not involve any original research using human subjects.
Supplemental files submitted
Prisma Checklist. Spreadsheet of Newcastle - Ottawa Quality Assessment Scale: Cohort Studies.
Trial registration
This was not a randomized clinical trial therefore it was not registered as such.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.