
Abstract
Background:
Pregnancy in women over the age of 35 years is considered advanced maternal age. The relationship between advanced maternal age and the risk of perinatal mortality is still controversial. As a result, this systematic review and meta-analysis were carried out to clarify the relationship between advanced maternal age and perinatal mortality in Ethiopia.
Methods:
The following electronic databases were used for this systematic review and meta-analysis: PubMed, Web of Science, Scopus, Science Direct, Google Scholar, HINARI, and African Journals Online up to March 2022. Addis Ababa, Gondor, and Jimma University research repositories were also searched. A random-effects model was used to pool study-specific odds ratios.
Results:
A total of 18 articles, including a total of 45,541 participants, were included in the meta-analysis. A total of 11 cross-sectional, 2 case-control, and 5 cohort studies were included. The overall pooled estimate indicates that women with advanced maternal age had a 1.58 higher risk of perinatal mortality compared to women in the younger age group (odds ratio = 1.58; 95% Confidence Interval: 1.13–2.03). The subgroup analysis also revealed that there were differences in the effect size as the geographical region differed. The result showed that the odd of perinatal mortality was highest in the Oromia region and lowest in the Southern Nations Nationalities and Peoples’ Region.
Conclusion:
The overall pooled estimate indicates that women with advanced maternal age had a 1.58-fold higher risk of perinatal mortality. Even though this risk could also be increased with other comorbid diseases, it is important for healthcare providers and other concerned stakeholders to be aware of the increased risks associated with advanced maternal age and provide different intervention programs designed to create awareness and provide counseling services to couples who seek to have a child in their later ages about the risks of advanced maternal age pregnancy on perinatal mortality and other adverse pregnancy outcomes.
Background
According to the International Federation of Gynecology and Obstetrics, advanced maternal age (AMA) is defined as age of 35 years or older at the time of delivery. 1 Despite reports of declining birth rates across the majority of age groups in various nations, older women are now giving birth at higher rates specially in developed countries.2,3 In the United States, 9% of first births were to women over 35 years of age, a 23% rise from 2000. 3 In England and Wales, 59.8 out of every 1000 live births in 2020 were to women over 35 years of age, up from 41.4 out of every 1000 live births in 2000. 4 The prevalence of AMA among pregnant women was 12.3% in a study undertaken in 359 health institutions from 29 countries, including Africa, Asia, Latin America, and the Middle East. 5
Due to an increase in the number of women aged 35–45, later marriage, second marriage, and the availability of better contraceptive options, births at later maternal ages are on the rise. Before considering getting pregnant, women have also stated that they want to achieve their professional, educational, financial, and personal goals, as well as the stability of their marriages.6,7
Numerous adverse neonatal outcomes, including perinatal mortality, are associated with pregnancy at AMA.2,5 The World Health Organization (WHO) defines perinatal mortality as pregnancy losses occurring after 28 weeks of gestation (stillbirths) and deaths of live births within the first 7 days after birth (early neonatal deaths). 8 While some obstetric problems in older women appear to be predominantly brought on by coexisting conditions, including multiple gestations, higher parity, and chronic illnesses, other complications appear to be primarily brought on by aging. Both could contribute to elder women experiencing increased maternal morbidity due to pregnancy.9,10–12
AMA has been linked to a number of pregnancy issues, including gestational diabetes, preeclampsia, Cesarean delivery, and placental abruption, according to a number of epidemiological studies. Delaying conception till later in life increases the risk of negative perinatal outcomes such as fetal growth restriction, preterm birth, low birth weight, birth asphyxia, prolonged stay in the Neonatal Intensive Care Unit, poor 5th min APGAR score, and perinatal mortality.2,5,12–16
Antenatal care and delivery in a healthcare facility are important factors in reducing perinatal mortality. However, in Ethiopia, the rates of receiving care from healthcare providers during pregnancy and giving birth in health facilities are relatively low. Only 43% of women receive care from healthcare providers during pregnancy, and only 48% give birth in health facilities. 17 Additionally, child mortality rates in Ethiopia remain high, with neonatal mortality accounting for approximately 30 per 1000 live births. Although there has been a slight decrease from 2005 when neonatal mortality was 39 per 1000 live births, the rates are still concerning.17,18 Studies have revealed that perinatal mortality is associated with variety of factors, including pregnancy occurring at AMA.19–23 A vast majority of studies conducted in Ethiopia have also indicated AMA as an independent risk factor for neonatal mortality.20,22–38 However, the results of some studies conducted in the southern part of the country showed that AMA does not increase the risk of perinatal mortality,29,33 showing inconsistency among the studies. As a result, the aim of this systematic review and meta-analysis was to assess the relationship between AMA and perinatal mortality in Ethiopia. The synthesis of the influence of AMA on perinatal mortality is critical for policymakers and program evaluators concerned with improving perinatal health. It is also used as an input for counseling women who are thinking about delaying pregnancy or who are pregnant but are worried about difficulties owing to their age.
Methods
Protocol and registration
This review protocol has been registered with the National Institute for Health Research’s PROSPERO international prospective register of systematic reviews under the registration number CRD42022327824, which can be found at https://www.crd.york.ac.uk/prospero/#recordDetails.
Identification and study selection
To determine the impact of AMA on perinatal mortality in Ethiopia, a systematic review and meta-analysis of the published and unpublished research were done. The databases, including PubMed, Web of Science, Scopus, Science Direct, Google Scholar, HINARI, and African Journals Online were retrieved. The research repositories of Addis Ababa, Gondor, and Jimma Universities were also searched. The following Medical Subject Headings search terms were used in the search: AMA, Delayed child bearing, Perinatal mortality, Perinatal death, Stillbirth, Neonatal death, Neonatal mortality, Fetal death, Fetal death, Neonatal loss, Intrauterine fetal death, Intrauterine fetal death, adverse birth outcome, adverse pregnancy outcome, and Ethiopia. Within each axis, keywords were combined with the OR operator and then linked the search techniques for the two axes to the AND operator (Supplemental Appendix 1). All published and unpublished studies in Ethiopia up to May 25, 2022 were extracted and evaluated for inclusion in this review. This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 39
Eligibility criteria
Inclusion criteria
In Ethiopia, articles describing the relationship between AMA and perinatal death were included. Only English-language full-text reports were included. Moreover, all observational studies (cross-sectional, case-control, and cohort studies) with original data on the relationship between AMA and perinatal death in Ethiopia were appraised.
Exclusion criteria
Non-accessible studies that have not been published, cannot be found online, or did not get email responses from the respective authors were excluded. In addition, after analyzing all texts, studies that did not provide the desired outcome were also excluded by three authors (GGB, EYR, and DNG).
Population/participants
The studies showing the association between perinatal mortality and maternal age were included.
Exposure and outcome
AMA is regarded as exposure, and perinatal mortality is the outcome.
Publication condition
Both published articles and unpublished research were considered.
Data abstraction
Four authors (GGB, ATY, DBF, and WDK) created a clear data extraction form in Microsoft Excel that was used to extract all of the necessary data. The study’s first author, the area in which it was conducted, the year it was published, the measure of association (either the risk ratio (RR) or adjusted odds ratio (AOR)), the sample size, the lower confidence interval, and the upper confidence interval for the target group were all taken into consideration when creating the data extraction format.
Outcome measurements
This systematic review and meta-analysis have one main outcome. The primary outcome was perinatal mortality. In this review, WHO’s definition of perinatal mortality was used to measure the outcome of the study.
Quality assessment
The researchers (GGB, EYR, DNG, ATY, DBF, and WDK) used the Newcastle-Ottawa Scale (NOS) adjusted for assessing the quality of the studies included in this review. 40 The NOS included three categories, each of which may be scored up to nine points. Each study’s quality was evaluated using the following scoring criteria: a score of 7 was deemed good quality, a score of 3 to 6 was deemed fair quality, and a score of 3 was deemed poor quality. Therefore, only primary articles of high quality were included in this systematic review to increase the validity of its findings. 41 The quality score of the articles included in this study is more than 7 (Supplemental Appendix 2).
Statistical analysis
The required information was gathered in Microsoft Excel format, and STATA Version 16.0 (StataCorp LLC, TX, USA) was used for analysis. Tables and forest plots were used to describe the original findings. Cochran Q statistics, Higgins I2, and p-value were used to test for heterogeneity between the included studies. These statistical analyses mentioned above indicated that there was significant heterogeneity between the studies (X2 = 82.1, df = 17, I2 = 79.3%, p-value 0.001). The heterogeneity was classified as low, moderate, or severe using cut-offs of 25%, 50%, and 75%, respectively.42,43 These statistical analyses mentioned above indicated that there was significant heterogeneity between the studies (X2 = 82.1, df = 17, I2 = 79.3%, p-value 0.001). Therefore, to determine the combined association between AMA and perinatal mortality, the Der Simonian and Laird random effect meta-analysis approach was used. 41
The funnel plot, Egger, and Begg tests were used to objectively test for possible publication bias at the 5% significant level.44–46 The statistical study found that there was no publication bias. To reduce the random differences between the point estimates from the original research, subgroup analysis was performed based on the region in which the original studies were conducted and the study design.
Results
Search results
Searching databases such as PubMed, Web of Science, Scopus, Science Direct, Google Scholar, HINARI, and African Journals Online yielded a total of 181 articles studying the relationship between AMA and perinatal death. The research repositories of Addis Ababa, Gondor, and Jimma Universities were also searched. Due to duplication, 60 articles were omitted from these preliminary records. Twenty articles were removed from the remaining 60 because their titles and abstracts were determined to be inapplicable. The remaining 40 full-text articles were then obtained and assessed for eligibility using the preset criteria, resulting in the exclusion of 22 articles, primarily due to the non-eligibility of the study population and outcome of interest. The quality scores of each study reviewed varied from 7 to 9 out of 10 points; hence, no studies were excluded based on this criterion. Finally, this meta-analysis included 18 studies (Figure 1) (Supplemental Appendix 3).

Flow chart of selection for systematic review and meta-analysis on the effect of AMA on perinatal mortality in Ethiopia, 2022.
Characteristics of the included articles
This systematic review and meta-analysis comprised 18 articles that showed an association between AMA and perinatal death. The included studies were carried out between 2013 and 2021. There were 11 cross-sectional studies in total, 2 case-control studies, and 5 cohort studies. To estimate the risk of AMA on perinatal mortality, 45,541 participants were included in the study. The sample size of the studies included ranges from 219 pregnant women from the study conducted in three districts in North Showa Zone, Oromia Region, Ethiopia 24 to 12,560 pregnant women from a study in Tigray Region, Ethiopia. 27
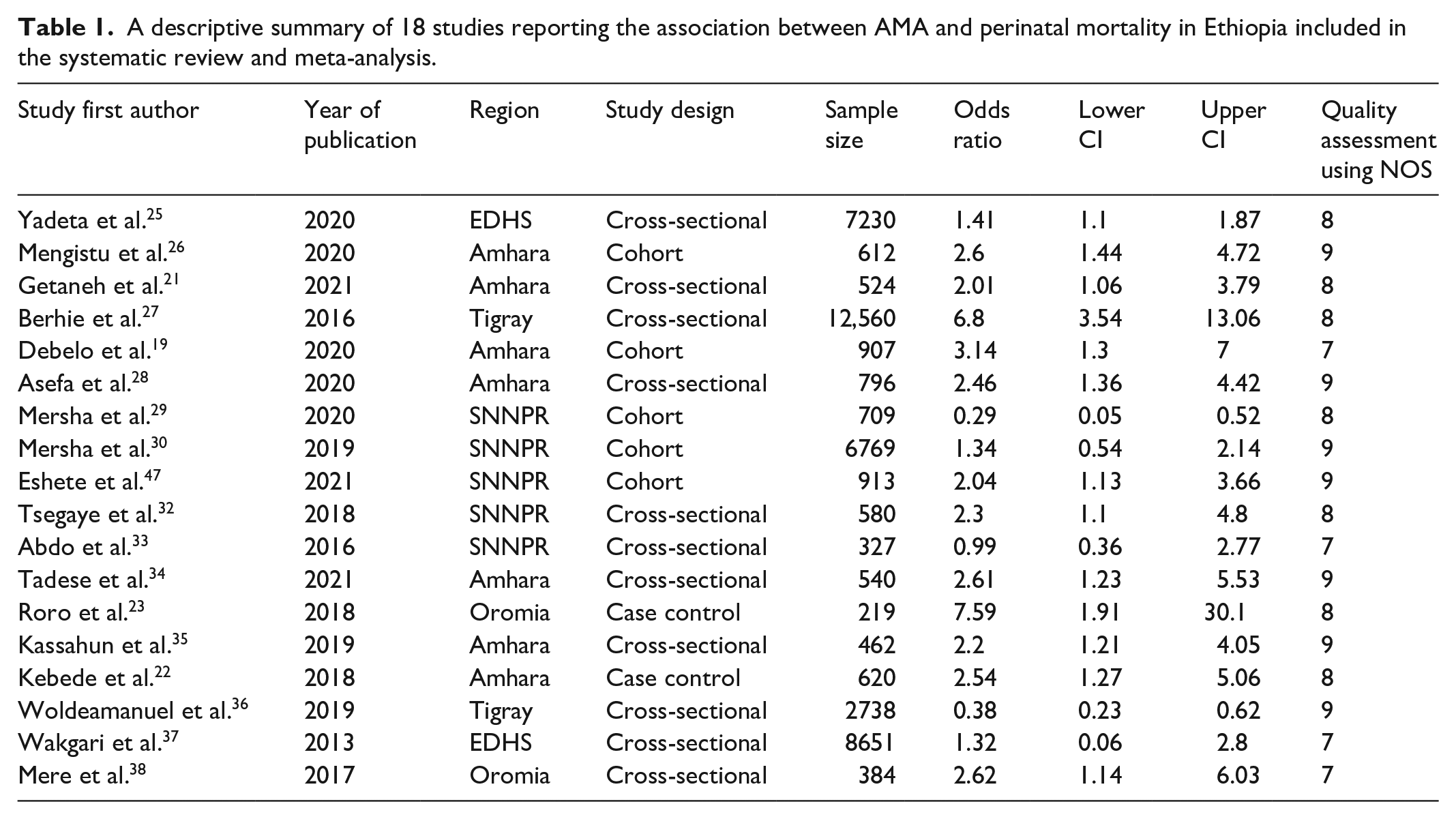
The majority of the included studies were from Amhara Regional State.20,21,23,26,28,34,35 Five studies were from the Southern Nations Nationalities and Peoples’ (SNNP) Region,30–33 two studies were from the Oromia region (OR),24,38 two studies were from the Tigray Region,27,36 and two studies were secondary data analyses using the Ethiopian Demographic and Health Survey24,25 (Table 1).
A descriptive summary of 18 studies reporting the association between AMA and perinatal mortality in Ethiopia included in the systematic review and meta-analysis.
The effects of AMA on perinatal mortality in Ethiopia
The pooled association between AMA and perinatal mortality by the random-effects model was statistically significant (Figure 2). The overall pooled estimate indicates that women with AMA had a 1.58-fold higher risk of perinatal mortality compared to women in the younger age group (OR = 1.58; 95% CI: 1.13–2.03). The test of heterogeneity for this study was (X2 = 82.1, df = 17, I2 = 79.3% and p = 0.001) showing the presence of substantial heterogeneity among studies.
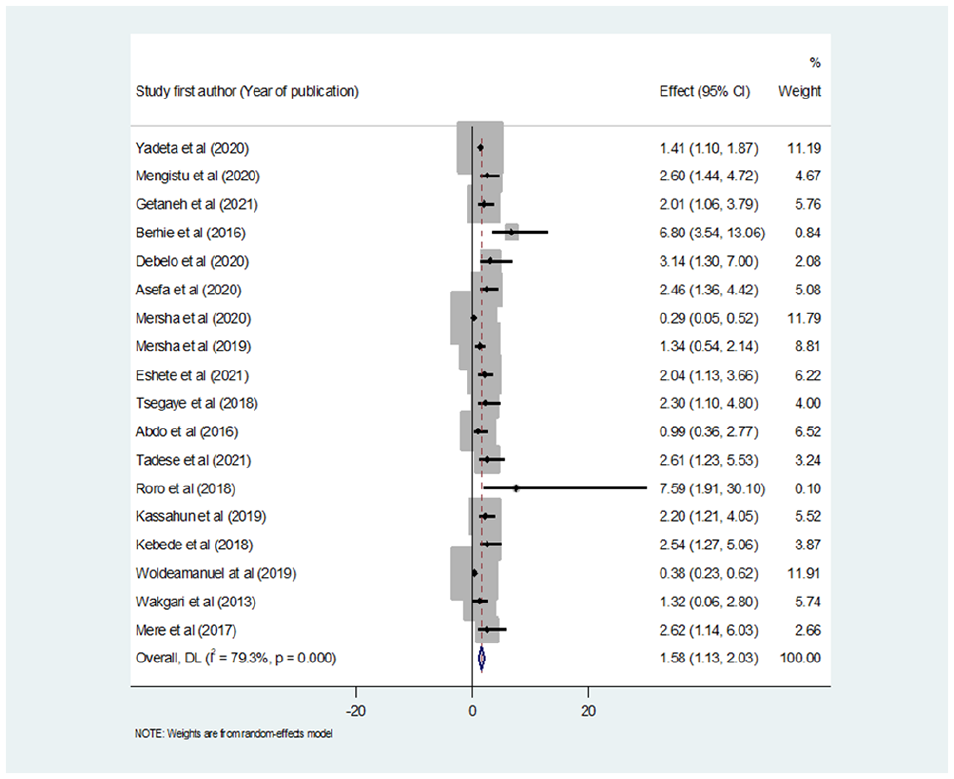
Forest plot showing the effect of AMA on perinatal mortality in Ethiopia.
Subgroup analysis
Subgroup analysis is based on region, where the original studies were conducted, and the pooled odds ratio in the majority of the regions remains statistically significant. The subgroup analysis also showed that the effect sizes varied depending on the geographical region. Moreover, the result showed that the odds of the perinatal mortality was at the highest in OR (OR = 15.88, 95% CI: 1.43–176.7, I2 = 0.0 and p-value = 0.496). Perinatal mortality related to AMA was the lowest in the SNNPR region (OR = 3.35, 95% CI: 1.46–7.67). Given this, the geographical differences are probably the causes of the heterogeneity among the included studies (Figure 3).

Subgroup analysis showing the pooled effect of AMA on perinatal mortality using regions in Ethiopia, 2022.
Subgroup analysis by study design was also performed, and the result revealed that there was the highest odd of perinatal mortality according to the study conducted using a case-control study design (OR = 13.87, 95% CI: 2.12–90.72, I2 = 0.0% and p-value 0.486), and the lowest risk of perinatal mortality was observed among the with cohort study design (RR = 4.77, 95% CI = 1.67–13.65, I2 = 82.3% and p-value 0.001) (Figure 4).

Subgroup analysis showing the pooled effect of AMA on perinatal mortality using the study design in Ethiopia, 2022.
Risk of publication bias
This systematic review and meta-analysis had heterogeneity in their results. To determine the cause of heterogeneity, publication bias was assessed. A visual analysis of the funnel plot figure revealed no indications of possible publishing bias (Figure 5). Furthermore, Egger’s test revealed no evidence of publication bias (p = 0.618).

Funnel plot presentation to assess publication bias for the effect of AMA on perinatal mortality in Ethiopia, 2022.
Discussion
This systematic review and meta-analysis include a thorough evaluation of the literature as well as quantitative estimations of the relationship between AMA and perinatal mortality. The study also aimed to determine the pooled effect of AMA on perinatal mortality.
Overall, the pooled effect size from this study revealed that AMA has an effect on perinatal mortality in Ethiopia (OR = 1.58; 95% CI: 1.13–2.03). This finding is congruent with most of the previous observational studies conducted in different parts of the world.5,48–51 Similarly, the result of one previous systematic review and meta-analysis regarding AMA and adverse pregnancy outcomes showed that the risk of perinatal mortality increased with AMA. 2
In the overall pooled effect size, the direction of association was clearly similar across all subgroup analyses. This provides additional evidence that AMA is associated with perinatal mortality.
The pooled subgroup analysis by region where original studies were conducted and study design (cross-sectional, case-control, and cohort study) also revealed that there was a positive association between AMA and perinatal mortality. The result of this analysis revealed that there were the highest odds of perinatal mortality among the studies conducted using the case-control study design (OR = 13.87, 95% CI: 2.12–90.72, I2 = 0.0%, and p-value 0.486), and the lowest risk of perinatal mortality was observed among the studies conducted with a cohort study design (RR = 4.77, 95% CI = 1.67–13.65, I2 = 82.3% and p-value 0.001). This variation might be related to the difference in study design, setting, period, and sample size.
Moreover, the odds of perinatal mortality were highest in the OR = 15.88, 95% CI: 1.43–176.7, I2 = 0.0 and p-value = 0.496) and the lowest in the SNNPR region (OR = 3.35, 95% CI: 1.46–7.67). This discrepancy’s likely causes include sociodemographic, cultural, and age-related differences in marriage, as well as communication gaps between couples on topics relevant to reproductive health, including when to start a family. Regarding the sociodemographic difference, for instance the contraceptive prevalence rate ranges from 3% in Somali up to 50% in both the Amhara Region and Addis Ababa. Contraceptive use increases with women’s education and household wealth. In OR it is about 41%. 52 There may also be differences in maternal education, the best indicators of contraceptive use, the timing of childbirth, and the spacing of children.53–55 The risk of prenatal mortality in the OR may also be enhanced by the fact that only two studies came from there, rather than by the real population difference. When compared to other studies, both have the smallest sample sizes of 219 and 384. For instance, the first study, conducted by Roro et al. with a sample size of 219, found that mothers aged 35 years and above had a greater risk of losing their newborn children to perinatal mortality than younger mothers (AOR 7.59, (95% CI, 1.91–30.10)). 24 Despite having the smallest sample size, it yielded the highest odds ratio of 7.85. Significant heterogeneity was observed among the included studies in this systematic review and meta-analysis. Geographical location and study design were two causes of variability, according to the subgroup analyses. It is challenging to infer a causal relationship between AMA and perinatal mortality from the results of observational studies, despite the fact that many studies and reports support the validity of these findings. Establishing temporality is essential for proving a causal connection. 56
Strengths and limitations of the study
The fact that this meta-analysis is the first of its kind in Ethiopia and that it seeks out both published and unpublished research, as well as using diverse perspectives to enrich the study, are its strengths. The majority of the included articles in this systematic review and meta-analysis, however, were cross-sectional in nature. As a result, it is impossible to establish the temporal correlations between the factors and the outcome variables. Furthermore, the different regions of the country might not be adequately represented, given that this meta-analysis only included accessible research data from four regions in Ethiopia.
Conclusion
This comprehensive review and meta-analysis of epidemiologic research revealed a positive correlation between AMA, and perinatal mortality. According to the study’s overall pooled estimate, women with AMA had a 1.58-fold higher risk of perinatal mortality. Therefore, various intervention programs should be developed to raise awareness of the dangers of AMA pregnancy on perinatal mortality and other unfavorable pregnancy outcomes and to offer counseling services to couples who desire to have children in their later years. To produce more robust data, interventional studies must also be encouraged in areas where there are not enough of them.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231201282 – Supplemental material for The effects of advanced maternal age on perinatal mortality in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121231201282 for The effects of advanced maternal age on perinatal mortality in Ethiopia: A systematic review and meta-analysis by Gemechu Gelan Bekele, Ephrem Yohannes Roga, Dajane Negesse Gonfa, Amare Tesfaye Yami, Daniel Belema Fekene and Wogene Daro Kabale in SAGE Open Medicine
Footnotes
Authors’ contribution
All authors GGB, EYR, DNG, ATY, DBF, and WDK—contributed significantly to the conception, conceptualization, and preparation of the text for this systematic review, as well as to the critical assessment, substantive feedback, and intellectual content of the study. The final article was read and approved by all authors.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Trial registration
Not applicable.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.