
Abstract
Urinary tract infections (UTIs) and chronic kidney disease (CKD) contribute to a substantial global health issue that is closely intertwined. Research has demonstrated that CKD increases the likelihood of individuals experiencing frequent, severe, and often antibiotic-resistant UTIs, which can accelerate the diminution of kidney function and result in end-stage kidney disease. The inherent structural, metabolic, and immunological disruptions linked to CKD create a suitable environment for uropathogens to grow in the urinary tract. This risk is further heightened by ongoing exposure to antibiotics, which facilitates the emergence of multidrug-resistant (MDR) organisms, complicating treatment options. This review discusses the existing literature on the clinical and microbiological relationship between CKD and UTIs, particularly highlighting the increased vulnerability of CKD patients to MDR pathogens supported by recent studies. It also addresses the disparity in the burden of these conditions in lower-income countries where access to renal replacement therapies is limited, as illustrated by the ISN-Global Kidney Health Atlas analysis. This review emphasizes the bidirectional challenge presented by CKD, which increases the risk of significant UTIs, while UTIs can worsen kidney damage. This damaging cycle is further intensified by factors such as weakened immunity, microbiota, and rising antibiotic resistance, creating a substantial clinical issue. To effectively manage antibiotic treatment, it is necessary to transition toward a proactive, integrative strategy. Key components include early screening for CKD in high-risk populations, maintaining optimal urogenital hygiene, and implementing strong antibiotic stewardship to enhance treatment effectiveness. Additionally, this review explores promising non-antibiotic prophylactic methods, including vaccines, antimicrobial peptides, and lifestyle changes, which are critical for breaking the cycle of infection and renal decline. A comprehensive approach that incorporates preventive measures, judicious use of antimicrobials, and addressing underlying renal issues is essential for improving long-term outcomes in this vulnerable patient demographic.
Plain language summary
Urinary Tract Infections (UTIs) and Chronic Kidney Disease (CKD) are serious health problems that often occur together and make each other worse. People with CKD are more likely to get frequent and severe UTIs, which are often harder to treat because the bacteria may resist antibiotics. These repeated infections can damage the kidneys further, speeding up the loss of kidney function and leading to End-Stage Kidney Disease (ESKD). CKD weakens the body’s defenses and changes the kidney’s structure and function, making it easier for harmful bacteria to grow. At the same time, frequent use of antibiotics in these patients increases the chance of antibiotic resistance, which limits treatment options. This problem is especially severe in low-income countries, where advanced kidney treatments are less available. This review explains the two-way relationship between CKD and UTIs and highlights how antibiotic resistance adds to the challenge. It suggests that a more proactive approach is needed, including early screening for kidney disease in people at risk, better hygiene practices, and careful use of antibiotics. New strategies such as vaccines, natural antimicrobial agents, and lifestyle changes also offer hope in preventing infections without relying only on antibiotics. By combining prevention, responsible antibiotic use, and treatment of underlying kidney problems, we can improve the long-term health and quality of life for people living with CKD.
Keywords
Introduction
Urinary tract infections (UTIs) and chronic kidney disease (CKD) are two of the most prevalent and clinically significant health disorders that simultaneously impose a considerable burden on the global health burden. The term UTI refers to an infection, typically of bacterial origin, developing anywhere throughout the urinary system, ranging from the urethral meatus to the perinephric fascia. 1 Consequently, CKD is characterized by anomalies either in kidney function or structure that persist longer than 3 months, with health concerns that affect an estimated of about 850 million people worldwide and are associated with increased morbidity, mortality, and healthcare costs.2,3 As per the National Kidney Foundation, criteria for CKD include structural abnormalities, namely, imaging-detected changes, histological lesions, or other markers of kidney damage (e.g., persistent albuminuria, urinary-sediment abnormalities, tubular or glomerular lesions) and even when estimated glomerular filtration rate (eGFR) remains <60 mL/min/1.73 m2 as well. 4 Emerging evidence indicates that the association between CKD and UTI can be bidirectional, where each condition can predispose, aggravate, or worsen the other.
Structural and immunological alterations in the urinary tract are the most common and major outcomes of CKD, along with metabolic derangements that contribute to creating a favorable environment for recurrent and often antibiotic-resistant UTIs. Conversely, repeated or poorly managed UTIs may lead to renal parenchymal injury and fibrosis, thus accelerating the progression of CKD. Thus, it forms a bidirectional connection which can be even further complicated by a rising concerning risk factor, namely antimicrobial resistance (AMR), which is particularly pronounced in patients with CKD due to the need for frequent hospitalization, repetitive antibiotic use, and resultant immunosuppression. 5 Moreover, individuals suffering from CKD are inherently more susceptible to UTIs due to the structural and functional changes and comorbidities such as diabetes mellitus (DM) on top of the compromised immune function.
This review provides a comprehensive overview on the possibility of worsening UTI and CKD occurrences and chances of creating even more burdensome conditions by including prevalence and incidence data of CKD and kidney failure as well as availability of peritoneal dialysis in four World Bank income groups—low, lower–middle, upper–middle, and high, from the most recent data of 2023 from the ISN-Global Kidney Health Atlas. 6
This review aims to explore the complex and bidirectional relationship between UTI and CKD, particularly emphasizing on susceptibility, recurrence, antibiotic resistance, and clinical outcomes for both the aforementioned diseases. It also addresses key pharmacological, molecular, and immunological aspects influencing this interdependence as well as bringing out the critical requirement for integrated diagnostic, therapeutic, and preventive approaches.
Methodology
This study was conducted as a narrative review of the relevant scientific and clinical literature. The comprehensive search was conducted manually. Searches on PubMed, Google Scholar, and Scopus were conducted to uncover evidence in the form of systematic review papers, meta-analyses, peer-reviewed research articles, clinical trial reports, and guidelines from nephrology and infectious disease societies. The search utilized keyword combinations such as UTI, CKD, antibiotic resistance, multidrug resistance (MDR), pyelonephritis, renal failure, uropathogens, adverse CKD progression, antibiotic stewardship, and non-antibiotic prevention. In addition to synthesizing a broader narrative, this review provides a thorough analysis of three observational studies conducted in South India, Bangladesh, and Romania. The chosen investigations are intentionally selected as diverse, practical examples that illuminate the key themes discussed, namely the characterization of microbiological profiles, the prevalence of MDR, and the risk factors contributing to the occurrence of CKD in patients suffering from UTIs. Relevant data were extracted from each study, including the most common pathogens, antibiotic resistance patterns, and statistically significant risk factors related to MDR UTI. These findings support the conclusions of the review by demonstrating the applicability of real-world evidence. Although publication dates were considered important, emphasis was placed on literature from 2010 to 2025 to ensure relevance. Data from global health organizations, such as the International Society of Nephrology (ISN) Global Kidney Health Atlas, 6 were incorporated to provide an epidemiological context. The information was organized into themes, covering the pathophysiology of the two conditions, their interrelationship, mechanisms, clinical implications of antibiotic resistance, and a comprehensive approach to prevention and management strategies.
Pathophysiology of UTIs
UTIs are one of the most widespread bacterial infections worldwide, with a range of clinical symptoms, and are broadly classified into uncomplicated and complicated infections. The primary cause is bacteria, though occasionally reports of fungi and viruses are also made. Although MDR does not increase the incidence of UTIs, the rising prevalence of MDR uropathogens has significantly complicated treatment and contributed to therapeutic failure and economic burden. 7 The prevalence of difficult-to-treat geriatric UTIs has increased due to the global expansion of MDR bacteria. When broad-spectrum antibiotics are misused or overused in elderly patients with UTIs, bacterial isolates resistant to the most commonly prescribed antibiotics can form. 8
They may arise in a complicated host situation, when the patient’s genitourinary tract has an underlying anatomical or functional problem, or in an uncomplicated host setting, where neither exists. 9 The most recurrent causes of UTIs are Uropathogenic Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Enterococcus faecalis, and Staphylococcus saprophyticus. 10 Compared to men, women are more prone to a UTI. It can cause pain and discomfort if the infection is restricted to the bladder. Common symptoms include pelvic or lower abdominal pain, a burning feeling when urinating (dysuria), an intense need to urinate even when the bladder is not full, and occasionally murky or strong-smelling urine. The infection causes an inflammatory reaction that makes the lining of the bladder sensitive and painful, which is the cause of this irritation and discomfort. 11 Uropathogenic bacteria multiply and release a variety of toxins and enzymes, such as hemolysins and proteases, which aid in tissue damage and host immune response evasion. This increases bacterial survival and pathogenicity within the urinary tract and accelerates the progression of infections. 12
UTIs are also classified as either localized (i.e., Cystitis) or systemic (e.g., pyelonephritis, prostatitis, etc.) based on the presence of clinical signs and symptoms by the European Association of Urology’s (EAU) guideline panel on urological infections. 13 Accordingly, prostatitis is considered systemic only when accompanied by systemic symptoms such as fever or chills, while otherwise it represents a localized infection. Risk factors that could put patients at risk for a severe clinical course or treatment failure must be taken into account. Urinary tract anomalies, the use of urinary catheters, prior antibiotic therapy, and underlying medical diseases can all have a substantial impact on the course of UTIs. 14
In complicated UTIs, catheterization can induce local urothelial injury and inflammation, resulting in the deposition of host-derived proteins such as fibrinogen on the catheter surface, which facilitates bacterial adherence and biofilm formation. Bacterial virulence factors—including adhesins, toxins, and biofilm-forming ability—interact with host defenses to determine disease severity, irrespective of the specific pathogen involved. 7 Due to biofilm protection, bacteria proliferate, and if treatment is not received, the infection may worsen and lead to bacteremia and pyelonephritis. 7 Multiple intrinsic and acquired variables, including vulvovaginal atrophy, vesicoureteral reflux, prostate gland enlargement, increased post-void residual urine volume, urinary catheterization, and behavioral factors, including having multiple sexual partners, family history all are risk factors for UTIs. The use of spermicide may also make women more susceptible to UTIs.15,16
However, a UTI that spreads to the kidneys can cause major health issues. 17 The existence of bacterial L forms, inadequate urothelial resistance, greater medication resistance of pathogens, and longer human lifespans could all contribute to the higher frequency of UTI. Re-infections are responsible for about 95% of the repetition of infections. E. coli is the most prevalent uropathogen, whereas Pseudomonas is the most virulent. 18 UTIs occur more frequently among sexually active women due to bacterial translocation from the vaginal or anal region to the urethra and bladder. According to studies, sexual activity is a recognized risk factor for UTIs, particularly in women, with risk further increased among individuals with multiple sexual partners. 19 UTIs can be confusing for both diagnosis and treatment. UTIs in adult males are less common than in females but may present in various forms, including cystitis, prostatitis, pyelonephritis, and catheter-associated infections. Management strategies depend on the site of infection, disease severity, and underlying risk factors. 20
The structural and functional integrity of the urinary tract plays a crucial role in preventing infection. The kidney, ureter, bladder, and urethra make up the urinary system by removing water-soluble waste and reabsorbing elements such as glucose, amino acids, and water, as we know the kidneys serve as the body’s natural filters. The ureters transport urine from the kidneys to the urinary bladder, from which it is subsequently eliminated through the urethra during micturition. When bacteria enter the urinary tract, infections such as cystitis and pyelonephritis may develop, potentially leading to renal damage if left untreated.21,22 The three ways bacteria can enter the body and produce UTIs are ascending, hematogenous, and lymphatic; the ascending route is the most common. Because of their shorter urethras, hormonal changes, and close contact with the anus, women are more prone to UTIs than men. 12 Once bacteria enter the urethra, they can rapidly colonize the bladder if host defense mechanisms fail, causing cystitis. They can also ascend to the kidneys, resulting in pyelonephritis. It is unknown what causes these infections, particularly when spermicidal medications or urinary catheters are used.7,23 The hematogenous (descending) route, which is mostly caused by Streptococcus or Staphylococcus species, is responsible for <5% of UTIs and usually affects those with ureteral obstructions or immunocompromised state. Bacteremia from severe and complex UTIs may spread to other organs or tissues, including lymph nodes. This isn’t the direct path of UTI progression, though. Conditions such as severe bowel infections and retroperitoneal abscesses are linked to lymphatic channels. 24
The characteristics of microorganisms commonly associated with UTIs are evolving, particularly due to antibiotic resistance. Age, diabetes, spinal cord damage, and catheterization are examples of underlying host variables that might worsen UTI and have an impact on its etiology. As a result, the causes of complicated UTI are more varied than those of uncomplicated UTI. 25 While community-acquired and nosocomial UTIs have become more resistant to antibiotics, uncomplicated UTIs have stayed stable over the last 20 years. Uncomplicated UTI symptoms usually include suprapubic pain or discomfort, bladder spasms, presence of blood in the urine (hematuria), hesitancy (difficulty initiating the urine stream), urgency (sudden desire to urinate), and pain during urination (dysuria). 26 Because of host features, the etiology of complex UTIs is more varied. Bacterial virulence and host defense components frequently interact to create UTIs, with each species having its own pathogenic pathways. Colonization is influenced by fluids, sticky properties, and receptor repertoire; a major susceptibility determinant is the genotype of epithelial cell receptivity. 27
Antibiotic resistance mechanisms in uropathogens
Since antibiotics are used extensively in urology to meet the demands of modern medicine, urologists are becoming increasingly concerned about antibiotic resistance. Empirical antibiotic therapy should be guided by local antimicrobial resistance patterns. There can be significant regional and temporal variations in the bacterial spectrum of UTIs and the rates of resistance for both simple community-acquired and complex nosocomially-acquired uropathogens. It is noteworthy that enterobacteria are becoming more resistant to fluoroquinolones. 28
Every year, over 150 million individuals suffer from acute or chronic UTIs. 29 According to estimates, 12% of men and 40% of women may experience at least one symptomatic UTI in their lifetime. Furthermore, between 27% and 48% of impacted women experience recurring UTIs.30,31
Over the past few years, bacterial infections such as UTIs have frighteningly increased their resistance to antibiotics through a variety of routes. 32
As was previously indicated, because of our decisions about antimicrobial therapy, urinary bacteria are showing signs of developing resistance to antibiotics. Target variation, reduced drug accumulation, and drug modification are the most typical causes of it. 33 Consequently, plasmid-mediated AmpC beta-lactamases, carbapenemases, extended-spectrum beta-lactamases (ESBL), and decreased susceptibility to fluoroquinolones as a result of qnr gene acquisition are the most relevant resistance indicators identified among UTIs.33,34 In 1983, SHV-2, the first ESBL, was identified in Klebsiella oxytoca in Germany. 35 After that discovery, ESBL-positive Enterobacteriaceae proliferated, first in Europe and then globally. They have been observed in community isolates of Enterobacteriaceae, although they are now more common in hospital isolates of K. pneumoniae and E. coli. 36 Most ESBLs are members of three families: cefotaximase (CTX-M), sulfhydryl variable (SHV), and temoneira (TEM). The majority of hospital isolates had TEM and SHV variations, whereas community isolates typically have CTX-M mutations. 33 Furthermore, mutations of the ancestral broad spectrum TEM-1, TEM-2, and SHV-1 beta-lactamases result in TEM and SHV variants. 36 A novel class of plasmid-encoded ESBLs known as CTX-M beta-lactamases hydrolyzes cefotaxime more selectively than other ESBLs. Although they are not directly linked, TEM and SHV beta-lactamases are both common members of Ambler’s class A, which is derived from the Gram-negative bacterial genus Kluyvera. 37 CTX-M enzymes have an inherent extended-spectrum profile, unlike TEM and SHV beta-lactamases, which depend on amino acid changes to expand their substrate profile. 38 Moreover, CTX-M are primarily isolated from community-acquired infections, in contrast to TEM and SHV enzymes, which are typically linked to hospital pathogens. 39 Some rare varieties of ESBLs include VEB, PER, and IBC. The genes that encode an accessible plasmid, which frequently includes genes for resistance to aminoglycosides, tetracyclines, sulphonamides, and fluoroquinolones, is nearly invariably where ESBLs are found. 36
Because of their multiresistant character, ESBL-producing Enterobacteriaceae strains can lead to hospital-acquired infection outbreaks that are challenging to contain.40–42 The chromosomal beta-lactamase of bacteria from the genera Enterobacter, Serratia, Citrobacter, Pseudomonas, and Acinetobacter are the source of plasmid-mediated AmpC beta-lactamases once the chromosomal gene escapes to a plasmid.33,37 They preserve fourth-generation cephalosporins and carbapenems while hydrolyzing monobactams, cephamycins, and third-generation cephalosporins. They are resistant to inhibition by clavulanic acid, sulbactam, or tazobactam, in contrast to ESBLs. 43
Carbapenems are frequently regarded as “the last resort antibiotics” for the management of serious infections brought on by ESBLs or Gram-negative bacteria that produce AmpC. Prior to recently, acquired carbapenem resistance was uncommon. 44 The majority of beta-lactamase-mediated resistance to carbapenems is caused by the expression of class A KPC beta-lactamases, which are inhibited by clavulanic acid; class B metallo-beta-lactamases of the IMP, VIM, or NDM series; or OXA-48 beta-lactamase, which is a member of class D beta-lactamases and is not inhibited by clavulanic acid, tazobactam, or sulbactam. As a result, the producing isolates are resistant to combinations of beta-lactam inhibitors.45,46
The pathophysiological and clinical landscape of CKD
CKD is a condition characterized by ongoing changes in kidney structure, function, or both, which have consequences for the individual’s health. 47 CKD is generally characterized by a decline in kidney function, defined as an eGFR of under 60 mL/min per 1.73 m2, or the presence of some compromised kidney markers such as albuminuria, hematuria, or abnormalities identified through lab tests or imaging that persist for not fewer than 3 months. The impact of CKD is substantially growing worldwide: roughly 10% of adults worldwide suffer from some type of CKD, leading to 1.2 million fatalities and 28.0 million years of life lost annually. By the year 2040, CKD is projected to rank as the fifth leading cause of death globally, representing one of the most notable anticipated increases among major causes of mortality. 48 The rates of incidence and prevalence for end-stage kidney disease (ESKD) vary significantly between different countries and regions. It is estimated that over 80% of individuals undergoing treatment for ESKD reside in wealthy nations that have a large elderly demographic and accessible healthcare for all. In developed nations and several developing areas, the primary factors leading to CKD are diabetes and hypertension (HTN); however, in many Asian and sub-Saharan African countries, glomerulonephritis and unidentified causes are more frequently observed. 49
Pathophysiology
A variety of elements can result in the development of CKD, such as low birthweight, pregnancy, obesity, diabetes, and aging. These situations introduce various factors that result in and intensify nephron loss, fostering cycles of injury that ultimately lead to CKD. 47 CKD develops through two main mechanisms: a primary trigger and a sustaining mechanism. The initial cause can be a pre-existing kidney problem (whether due to developmental abnormalities or injuries sustained over time), an inflammatory or immune-mediated issue, or exposure to toxins. This damage is then sustained by hyperfiltration and the enlargement of remaining nephrons through hormonal, cytokine, and growth-factor pathways, leading to increased intraglomerular pressure and structural alterations. 50 Hypertension ranks as the second most prevalent cause of end-stage renal disease (ESRD). It leads to a nephrosclerosis glomerulopathy, which is characterized by (i) renal vasculopathy that affects preglomerular arteries and arterioles, primarily resulting from atherosclerosis, endothelial breakdown, thickening of the walls, and fibrosis; (ii) microvascular damage to the glomerular tuft capillaries; (iii) diffuse glomerulosclerosis, and less frequently, focal and segmental glomerulosclerosis (FSGS), which involves harm to the constituents of the filtration barrier (podocytes, mesangial cells, and basement membranes); and (iv) interstitial fibrosis. As a result of arteriolar vasculopathy, vascular obstruction, and a reduction in vascular density, there is an overall decline in renal blood flow. 51 The observation of an enlarged glomerular size in moderately corpulent individuals (with a body mass index (BMI) within a range from 30 to 35 kg/m2) who are otherwise healthy indicates an elevated single-nephron glomerular filtration rate (GFR). 74 Generally, the link between obesity and adverse kidney outcomes continues to hold even after accounting for higher blood pressure (BP) and diabetes, implying that the hyperfiltration of glomeruli driven by obesity plays a direct role in nephron loss. Additionally, various hormones produced by fat tissue, along with inflammation associated with obesity, may also play a part in this process. 47 The traditional characterization of diabetic nephropathy involves a gradual and progressive rise in albumin levels in the urine, followed later by a decline in the eGFR to <60 mL/min/1.73 m2, which may ultimately result in ESRD. The initial phase of diabetic nephropathy is marked by hyperfiltration, during which the GFR is markedly elevated compared to normal levels. Persistent albuminuria is regarded as the first clinical indicator of diabetic nephropathy. In the beginning, small quantities of albumin seep into the urine, remaining below the detection threshold of a urine dipstick. This phase is known as “microalbuminuria.” 52 In the early stages, hyperglycemia elevates the expression of endothelial nitric oxide synthase (eNOS) in the afferent arterioles and glomerular capillaries, leading to vasodilation and an increase in the GFR. Over time, the expansion of the glomeruli results in endothelial dysfunction and changes in hemodynamics, alongside a loss of the electric charge of the glomerular basement membrane (GBM) and thickening of the GBM. This process, along with a reduced number of podocytes, the elimination of foot processes, and the expansion of mesangial cells, underpins the initial damage to the glomeruli that ultimately results in glomerulosclerosis. Podocyte injury is recognized as a pivotal event, supporting the concept that diabetic nephropathy fundamentally involves podocyte loss. In addition to the direct impacts of hyperglycemia on tubular cells, damage to the glomeruli also inflicts injury on the tubules, leading to cell death, epithelial to mesenchymal transition (EMT), cellular infiltration, degeneration of tubules, and fibrosis in the interstitial tissue through various mechanisms. Two main pathological pathways have been identified in the total degeneration of nephrons. In pathway I, the collapse of glomeruli occurs prior to or simultaneously with tubular degeneration, while in pathway II, tubular atrophy occurs beforehand to glomerular degeneration. 51
Diagnosis parameter
CKD is categorized by its etiology, GFR category, and albuminuria category, which is termed as the CGA classification. The cause of CKD is determined by whether there is a systemic disease present and by the specific area of the kidney where pathological or anatomical abnormalities are observed or assumed. The estimated risk for accompanying complications and future outcomes can be forecasted by utilizing GFR categories and the degree of albuminuria. 50 The eGFR is a formula utilized to assess the efficiency of your kidneys in filtering specific substances produced by your body, including creatinine (a byproduct resulting from regular muscle degradation) and cystatin C (a protein that impedes the degradation of other protein cells). eGFR tests are commonly accessible, cost-effective, and take less time to administer. 53
The classification known as CKD staging reveals a clear pattern regarding the progression of CKD. This staging divides the disease into five main stages, with stage 3 further divided into 3a and 3b to facilitate a more precise assessment of moderate impairments. The stages correlate directly with the eGFR, the primary quantitative indicator of kidney function, recorded in mL/min/1.73 m2—this reflects the blood volume filtered by the kidneys each minute, adjusted for a standard body surface area. As the disease progresses, its severity escalates from stage 1 to stage 5, with eGFR values decreasing in accordance with the kidneys’ reduced ability to filter blood. The staging begins at stage 1, where kidney functions may remain normal or even optimal despite the presence of structural damage, and continues to represent increasingly significant functional losses. The final stage, stage 5, referred to as ESRD, signifies kidney failure, a condition when the kidneys are no longer capable of meeting physiological demands without medical intervention such as dialysis or transplantation (Table 1).
Staging of chronic kidney disease based on eGFR. 53 .

eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease.
The eGFR is valuable for evaluating long-term changes in kidney function, but it is not appropriate for use in cases where kidney function is undergoing rapid changes. A swift loss in kidney function is known as acute kidney injury (AKI). AKI can arise alongside nearly any acute systemic condition, particularly those that result in low BP or a decrease in intravascular volume. 52
Prevalence of CKD: Global data according to World Bank income group
Kidney failure, also termed as ESKD, represents one of the most severe and life-threatening outcomes of CKD. Its global burden is escalating rapidly, with higher impacts in low-income and lower-middle-income countries (LMICs). While advancements and availability in dialysis and transplantation have significantly improved in high-income countries (HICs), access to these life-saving therapies remains limited in lower-income settings and eventually contributes to higher prevalence of CKD and kidney failure. According to most recent data of 2023 from the ISN-Global Kidney Health Atlas, 6 the vast majority of individuals in low-income (LIC) and LMICs who develop kidney failure are either untreated or die prematurely due to the lack of affordable and available kidney replacement therapy (KRT). This section highlights the burden of kidney failure across the four World Bank income groups—low, lower-middle, upper-middle, and high—by comparing key metrics such as prevalence of CKD and kidney failure, availability of peritoneal dialysis collected from the most recent ISN-GKHA data of 2023.
The estimations of the kidney disease-associated prevalences for the four World Bank income groups were conducted ensuring the participation of at least 70% of the countries in that region. The term prevalence of CKD is indicated for the percentage of patients suffering from CKD. Meanwhile, the terms incidence of kidney failure and prevalence of kidney failure describes annual number of new kidney failure cases per million population and total number of existing kidney failure cases per million population. The percentage of prevalence of CKD is observed to be progressively rising with the ascending economic status of the countries from low income toward high income, as the low-income countries have 3.6% of prevalence whereas it rises to 11.2% in high-income countries, with lower-middle-income countries having 6.4% and upper-middle-income countries having 10.5% prevalence in general. The statistics of prevalence of kidney failure with already existing kidney failure cases show disproportionate increase in the total number of occurrences. A drastic rise in the availability of peritoneal dialysis between the four different economy groups is observed, with 17.6% availability in low-income countries, 67.5% in lower-middle income economies, 89.2% in upper-middle-income countries and nearly 100%, 96.9%, in high-income countries. This greater availability aids in the management of CKD occurrence and recurrence in the high-income economy groups than the lower-income economy groups (Figures 1–4).

A summarized visualization of the metrics associated with CKD contributing to the burden of kidney failure, according to estimations from the ISN-Global Kidney Health Atlas in the year 2023 for low-income countries (according to World Bank Income Group). 6

A summarized visualization of the metrics associated with CKD contributing to the burden of kidney failure, according to estimations from the ISN-Global Kidney Health Atlas in the year 2023 for lower-middle-income countries (according to World Bank Income Group). 6

A summarized visualization of the metrics associated with CKD contributing to the burden of kidney failure, according to estimations from the ISN-Global Kidney Health Atlas in the year 2023 for upper-middle-income countries (according to World Bank Income Group). 6

A summarized visualization of the metrics associated with CKD contributing to the burden of kidney failure, according to estimations from the ISN-Global Kidney Health Atlas in the year 2023 for high-income countries (according to World Bank Income Group). 6
A bidirectional burden: How CKD and UTI accelerate each other’s progression
UTI is a pathological condition due to invasion of microbial in the urinary tract. It is among the most prevalent infections that both patients in hospitals and the general population deal with. 54 While UTIs can affect individuals across the general population, their clinical course, recurrence rate, and resistance patterns are notably more severe and complex in CKD patients. It is considered that approximately 5% of men and 40% to 50% of women may experience the occurrence of UTI at least once during their lifetime. 55 A combination of CKD causes urinary tract dysfunction, impaired immunity, antibiotic overexposure, and comorbidities (such as DM, HTN, etc.) contributes to more vulnerability and susceptibility toward UTI. 54
The connection between UTIs and the development of CKD is complex; instances of isolated uncomplicated cystitis and asymptomatic bacteriuria in individuals with mild or moderate CKD and without other urinary tract anomalies seldom lead to a significant decline in eGFR. Conversely, recurrent UTIs greatly enhance the risk of progressing to ESKD. Within these recurrences, complicating factors can render such incidents particularly detrimental, especially in cases of acute pyelonephritis or uroseptic syndrome, in patients under influence of dialysis, those with structural urinary tract dysfunction, polycystic kidney disease, or in situations involving urolithiasis, severe DM, or metabolic instability affecting renal perfusion. These conditions create the potential for an acute injury to be compounded by a gradual worsening of renal function. Similarly, obstructive nephropathy diminishes the risks associated with UTIs by leading to structural damage through papillary necrosis and the leakage of tissue debris into the lumen, which are often observed in ischemic, diabetic, or analgesic nephropathy. 56
The influence of genetic factors on the likelihood of UTIs and the extent of resulting renal damage is crucial. Numerous polymorphisms that modify the expression of toll-like receptors (TLR), which are vital in the innate immune response to urinary pathogens, can hinder or enhance this response. The three primary receptors are TLR2, TLR4, and TLR5, each significantly contributing to UTI prevention. For instance, certain TLR4 polymorphisms negatively impact its function, thus encouraging asymptomatic bacteriuria (ASB). A recent decrease in vascular endothelial growth factor A (VEGFA) and transforming growth factor beta 1 (TGFβ1) has also been linked to kidney scarring following UTIs and the progression toward CKD, particularly in patients with vesico-ureteral reflux. Additionally, alterations in CXC chemokines and their receptors, especially the interleukin 8-receptor (CXCR1 and CXCR2) that guide neutrophil movement, are associated with the onset of UTI. 55
Dialysis, also known as renal replacement therapy (RRT), is a therapy employed for the treatment of renal failure, in both ESRD and severe AKI to remove metabolic waste, excess fluid, and toxins from the blood. 57 Patients with stage 2 to 5 CKD and those who are on chronic dialysis treatment are at elevated risk of UTI and urosepsis. 58 In individuals reliant on dialysis urine output may decrease significantly which can reduce mechanical flushing of the urinary tract, thereby facilitating bacterial colonization. The result from a study conducted by Yamashita et al. on dialysis-dependent ESRD patients shows that the rate of UTI in those individuals was 20% and 32%, respectively, in male patients and female patients. Additionally, it presented the presence of a higher proportion of resistant bacteria in the causative organisms of UTI among the dialysis-dependent ESRD patients. 59 Another contributing factor is the reduced production of innate urinary defense molecules, for example, uromodulin which aids in neutralizing uropathogens are observed in patients with impaired kidney function, including those undergoing dialysis. This reduction accelerates increased UTI susceptibility in that population. 56 Moreover, dialysis patients may have to frequently experience antibiotic courses and urological interventions likely catheterization, which may elevate the incidence of UTIs caused by resistant organisms accentuated by their immune dysregulation. 59
Initially, CKD may appear as a disease that can be readily diagnosed, however, without active screening initiatives, patients are often evaluated when they have already progressed to a stage of moderate, or even advanced CKD, and thereby leading to associated complications. The dysfunction of the innate and adaptive immune responses due to chronic renal disease elevates patients’ susceptibility to infections. CKD comprises a range of immunological and metabolic abnormalities that increase vulnerability toward UTIs, for example, elevated apoptosis of lymphocytes, increased levels of tumor necrosis factor α (TNFα) and interleukin 6 resulting in reduced function of neutrophils and increase in uremic toxins levels, which interfere with the migration and adherence of leukocytes to the sites of injury. 55 Through the epigenetic modifications in hematopoietic stem cells, it causes a shift from lymphoid to myeloid cell lineage, which may be underlying cause of uremia-associated immunological senescence, which is unable to be reversed by renal replacement therapy, including kidney transplantation. 60 A study conducted by Ishigami in 2019 analyzed the epidemiology of infectious diseases in CKD and highlighted that the risk of hospitalization with infections was increased by 50% in stage G3 of CKD and by 2 to 3 times in stages G4 and G5 compared to stage G2 of CKD. 61 Proteinuria, which is commonly found in CKD-affected individuals and being the most important predictor factor of ESKD for over a decade, is a particular risk factor regarding infectious diseases. 55
CKD also contributes to UTI by interfering with urinary microbiome. A study conducted by Modena et al. in which healthy individuals were compared with patients who have undergone renal transplantation as well as patients who experienced cellular rejection after undergoing transplantation and individuals with interstitial fibrosis and tubular atrophy shows that, Streptococcus (the dominant genus in healthy male population) was reduced in transplanted patients and even more in patients with interstitial fibrosis and tubular atrophy. 62 Furthermore, the wide variation of the microbiome was identified to be significant in case of eGFR, neurogenic dysfunction of the bladder, interstitial cystitis and urgency urinary incontinence. 55
Antibiotic resistance, one of the major healthcare problems rising worldwide, has become another underlying risk factor for UTI occurrence in patients with CKD. Antibiotic-resistant patients contribute as host reservoir for the transmission of MDR bacteria. High treatment failure rates attributed to UTIs have led to the emergence of antibiotic resistance and, later, MDR. Certain virulent bacteria have evolved to an extent that they can develop MDR to antimicrobials. For instance, E. coli is a gram-negative bacterium that can produce vast amount of beta-lactam enzymes, proactively making them ineffective against the majority of beta-lactam antibiotics. 63 A study by Sumon et al. shows that patients with the history of UTI occurrence, patients with diabetic CKD and those who have taken antibiotics within the last 6 months were found to be significantly (p < 0.05) associated with the development of MDR UTI. Alongside, antibiotics of Penicillin, Quinolone, and Aminoglycoside groups are resistant to most of the gram-negative and gram-positive bacterial isolates. Linezolid, Vancomycin, Cefoxitin, Polymyxin B, and Colistin Sulphate showed the most sensitivity to bacterial UTIs, accompanied by Meropenem and Nitrofurantoin. 63 Furthermore, antibiotic pharmacokinetics and pharmacodynamics are significantly altered in CKD due to changes in drug clearance, protein binding, and tissue distribution. This often leads to subtherapeutic levels or accumulation of toxic metabolites, which not only impairs efficacy but also may promote bacterial persistence and resistance 64 (Figure 5).

Some clinical investigations on the interrelationship between UTIs and CKD
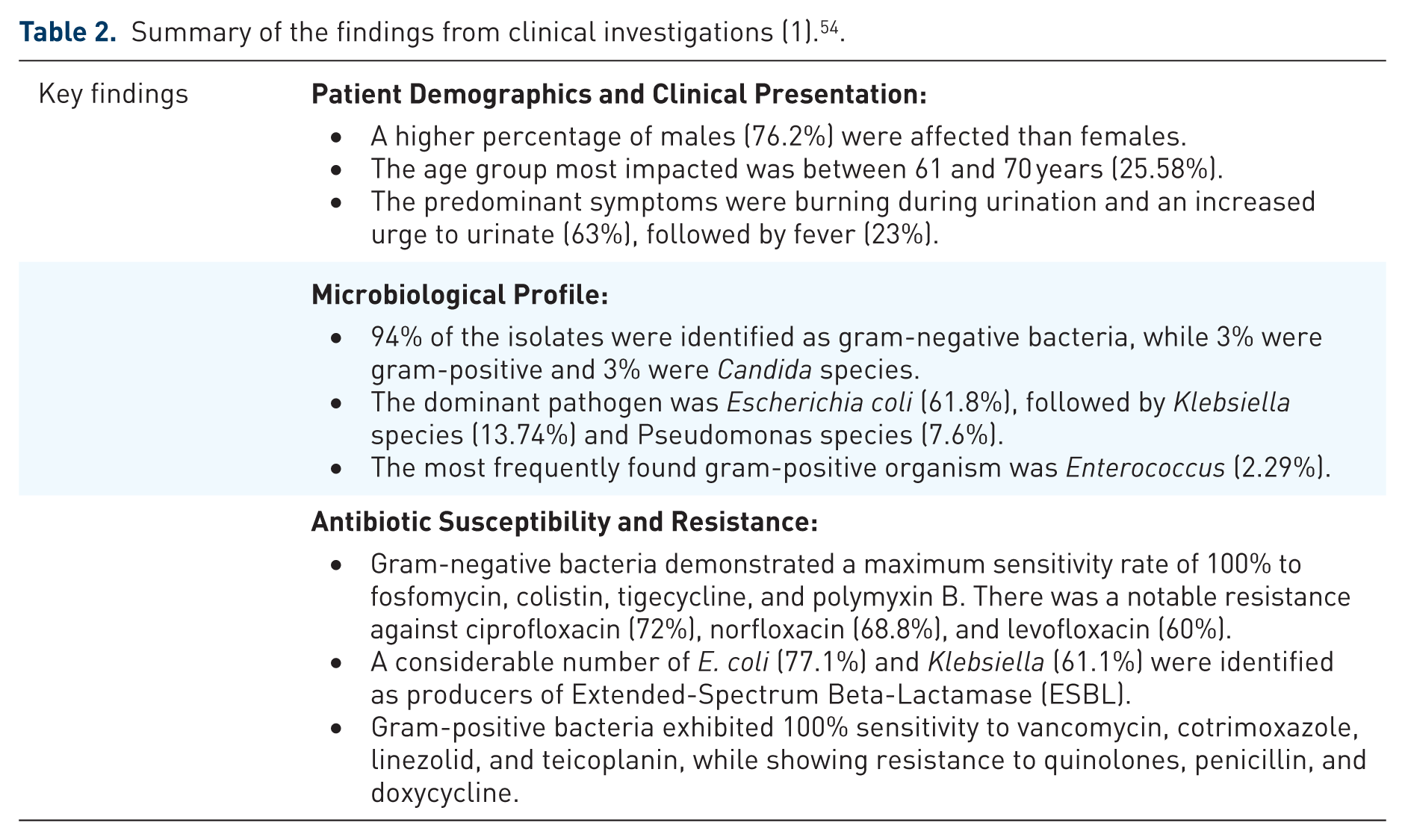
The objectives of this retrospective descriptive study were to elucidate the clinical and microbiological features of UTIs in individuals with CKD and to outline the susceptibility patterns of the isolated organisms. The research was conducted at a tertiary government-run referral hospital serving patients with renal problems named the Institute of Nephro-Urology in Bengaluru, South India, with the study taking place from January 2020 to June 2020. The sample included 129 adults with CKD (ranging from stage 1 to stage 5, including those on dialysis) who demonstrated UTIs confirmed by culture. Patients who had been administered antibiotics within 48 h prior to the collection of urine for culture or who had cultures from nonurinary sites were excluded from the analysis 54 (Table 2).
The present study seeks to elucidate the occurrence and epidemiological patterns of MDR UTIs in individuals with CKD and to characterize the antibacterial resistance features of the identified pathogens. This research was conducted in the Department of Nephrology at Bangabandhu Sheikh Mujib Medical University in Bangladesh as a cross-sectional observational study executed over a period from September 2019 to August 2020. Participants were selected through purposive sampling. Data were collected using semi-structured questionnaires, medical records, and laboratory tests, which included urine culture and sensitivity analysis. A total of 326 adult patients with CKD, aged 18 years and older, were included in the study. Among these, 60.1% were female, and 39.9% were male, with 75.2% being outpatients and 24.8% inpatients. The inclusion criteria required that CKD be confirmed alongside the presence of urine microscopy showing a significant amount of pus cells, specifically at least ten pus cells per high power field. Patients with polymicrobial infections, those with Candida species detected in their urine, pregnant individuals, and renal transplant recipients were excluded from the study 63 (Table 3).
This research is a single-center, retrospective observational study that explored risk factors associated with AMR, including MDR, in patients hospitalized with UTIs alongside their CKD. From January 2019 to December 2020 at the Sf. In Ioan Emergency Clinical Hospital in Bucharest, Romania, a total of 1103 patients were evaluated, leading to the selection of 564 adult inpatients with microbiologically confirmed UTIs for final analysis. The average age of the study population was 68.6 years, with 54.6% of the total being patients suffering from CKD 65 (Table 4).
Summary of the findings from clinical investigations (1). 54 .
Summary of the findings from clinical investigations (2). 63 .

CKD, chronic kidney disease; MDR, multidrug-resistant; UTI, urinary tract infection.
Summary of the findings from clinical investigations (3). 65 .

AMR, antimicrobial resistance; CKD, chronic kidney disease; MDR, multidrug-resistant; UTI, urinary tract infection.
Insights into preventive strategies for UTIs and CKD
Screening and early detection strategies
Chronic kidney disease
According to several guidelines, people with risk factors—specifically, DM, HTN, and a history of cardiovascular disease—should undergo screening for CKD at least once a year. Important evaluation techniques include calculating the albumin-to-creatinine ratio, assessing serum creatinine levels, determining the GFR using a creatinine-based formula, and doing a routine urinalysis. The spot urine albumin-to-creatinine ratio, derived from an early morning sample, is the preferred method for detecting proteinuria because it has higher sensitivity than the protein-to-creatinine ratio for detecting subclinical proteinuria. There are many kidney illnesses, and because of its high accuracy—especially when GFR is getting close to the reference range—the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation is generally accepted as the standard for determining GFR in ordinary clinical practice. Serum cystatin C is a newer filtration biomarker that offers a more precise estimation of GFR and aids in classifying CKD; it is particularly valuable in cases of gradual GFR decline that may not be clinically apparent, though false positives may still occur, making serum cystatin C-based GFR assessments particularly useful. 66 Stages one through three of CKD are often undiagnosed, therefore, failure to diagnose patients during these stages may result in a high incidence of preventable complications and progression to advanced kidney failure. As a result, primary care should be the first to refer patients for early consultation and referral to a nephrologist. This will increase the chances of effective dialysis while lowering hospitalization and mortality rates. 67 The National Kidney Foundation recommends using a kidney profile that includes measuring serum creatinine at the same time to calculate the urine albumin-to-creatinine ratio (ACR) and eGFR. An eGFR of <60 mL/min/1.73 m2 or albuminuria of 30 mg or more per 24 h are examples of structural or functional abnormalities that are indicative of CKD and will last for more than 3 months. People who have clinical risk factors, such as obesity, kidney stones, autoimmune diseases, recurrent UTIs, or reduced renal mass as a result of nephrectomy or low birth weight, could require routine testing. 68
Urinary tract infection
Timely identification and monitoring of UTIs are essential for effective treatment, primarily to prevent serious complications like sepsis and to reduce patient discomfort. While urine culture methods are regarded as the gold standard, they can delay diagnosis by 2 to 3 days. In contrast, alternatives to culture-based diagnostics, such as rapid near-patient urine tests, particularly urine dipsticks, allow for preliminary diagnosis by measuring biochemical indicators like nitrite and leukocyte esterase. Although dipsticks are easy to use, cost-effective, and provide results in just a few minutes, their clinical utility is limited due to low sensitivity and their inability to provide information on bacterial presence or concentration, as well as antimicrobial susceptibility. Consequently, various innovative techniques are being explored to identify uropathogens more quickly. Some of these techniques involve analyzing urine for volatile organic compounds using gas chromatography and mass spectrometry, as well as employing Raman and Surface-Enhanced Raman Spectroscopy, which can potentially quantify, identify, and assess antimicrobial sensitivity of bacteria present in urine. Additionally, impedance spectroscopy is being researched for the ultra-low detection and quantification of E. coli in urine. Despite the rapid nature of these technologies, they still do not provide comprehensive microbiological diagnoses or susceptibility data, which remains critically important for complicated UTIs. 69 A positive urine culture with both localized and systemic symptoms is typically part of the standard diagnostic criteria for a UTI. But in women with acute, uncomplicated cystitis, the diagnosis can frequently be made without a visit to the doctor or the collection of a urine sample. Having at least two known urine symptoms, such as urgency, frequency, or dysuria, without vaginal discharge, indicates a 90% chance of acute cystitis in women who visit outpatient clinics. Since the pretest probability is already very high in these situations, using a urine dipstick to detect leukocyte esterase usually only slightly improves the sensitivity and specificity of the diagnosis. 70 The process of identifying infectious diseases has been significantly sped up by recent developments in molecular diagnostic tools, especially the polymerase chain reaction (PCR). This rapid pathogen detection became particularly evident during the COVID-19 pandemic. At five valley urology, a private clinic in Missoula, Montana, PCR-based laboratory-developed tests (LDTs) are commonly employed to diagnose UTIs. The test is designed to detect 21 specific species of microorganisms along with 20 antibiotic-resistance markers in urine samples from patients displaying signs of a UTI. The process was created and validated internally because there aren’t any FDA-approved PCR assays specifically designed for this usage yet. A board-certified clinical chemist oversaw the extensive and rigorous validation process to ensure its suitability for clinical applications. Validation studies indicate that standard urine cultures can be time-intensive, often taking several days to yield results, and they are prone to false negatives, especially for difficult-to-culture organisms, frequently leading to incorrect reports of sterile urine in patients who exhibit clinical signs of infection. The introduction of the PCR test at the five valleys urology clinic has set a new standard for the rapid identification of microbes and resistance genes: utilizing samples from 350 patients who visited the clinic within 6 months in 2022, it was possible to confirm 196 cases of accurate identification of microbes and resistance genes. This swift and precise diagnosis facilitates timely and definitive therapeutic decisions. 71 A clinical evaluation of UTIs should initially assess whether the case is asymptomatic bacteriuria, an uncomplicated (simple) UTI, or a complicated UTI. These categories inform subsequent diagnostic processes, the care setting (either outpatient or inpatient), and the choice, dosage, and duration of antimicrobial treatment. Additionally, any recurrence can be categorized as either a reinfection occurring from a separate incident or a relapse resulting from the previous episode. 72
Urogenital hygiene and infection prevention among women
UTIs are among the most common bacterial infections; by the median age of 40, one in three adult women will have had one. They frequently have high recurrence rates, which can result in renal failure and serious kidney damage. This condition impacts the female genital tract, which hosts a unique microbial reservoir consisting of indigenous flora, where intrinsic barrier mechanisms, such as vaginal secretions and an acidic environment, along with the resident microbial communities, work together to thwart microbial invasion. 73 Maintaining a vaginal pH of 4.5 is crucial for a functional vaginal immune barrier, and changes in pH or the normal vaginal microbiome, particularly the beneficial Lactobacilli, can lead to inflammatory lesions. Reproductive tract infections have been associated with intravaginal practices (such as douching and the insertion of external products like powders, creams, herbs, and traditional remedies). Furthermore, the combination of douching and penicillin has been shown to double the incidence of vaginal infections and heighten the likelihood of cervical infections. Similarly, a higher risk of Candida infections has been associated with the use of reusable absorbent materials, such as those used during menstruation. Additional risk factors, including inadequate drying of the genital area, using fabrics for drying, and poor hand hygiene, have all been connected to a rise in vaginal and genital infections. 74 Urogenital hygiene must be strictly adhered to when people with CKD have urine catheterization in order to prevent UTIs. Patients with indwelling catheters are especially susceptible to UTIs, a serious subset of healthcare-associated infections. Urinary catheter use on a daily basis has been shown to raise the intraluminal bacterial load by around 5%, which makes this population especially susceptible. General malaise, itching around the catheter site, and the development of murky urine are warning signs and symptoms that need to be watched for and treated. 75 Other notable factors linked to a history of UTIs include the occurrence of gynecological surgeries. This relationship may be explained by alterations in the vaginal microbiota and the modified mechanical environment that arises during surgical procedures aimed at the genital tract, which collectively can diminish the resistance of normal vaginal microbiota to pathogenic species, leading to colonization and increased instances of UTIs. 76 To ensure genital hygiene in females, several hygienic practices are recommended. First and foremost, undergarments should be dry and highly absorbent. Additionally, it is advisable to avoid using loose powder or frequent topical cleansers and antiseptic solutions. Given the recent surge in antimicrobial resistance, non-antibiotic treatment options for recurrent UTIs (rUTIs) are being favorably considered. 77 Methenamine hippurate is a urinary antiseptic used as a non-antibiotic prophylactic measure in those with rUTIs. Methenamine, an antiseptic agent primarily available in 1967, has re-surfaced as a potential prophylactic option for UTI in a number of populations, including renal transplant patients. Methenamine is hydrolyzed in the acidic pH of urine, producing ammonia and formaldehyde. The primary antiseptic mechanism is associated with the produced formaldehyde, which denatures the protein and nucleic acids within bacterial cell wall thus exhibiting non-specific antimicrobial activity. 78
Proper genital cleaning involves wiping from front to back, using clean water, and drying with a fresh tissue or cloth after urination or bowel movements. An overly moist pubic area fosters an ideal environment for the growth of microbes. Furthermore, wearing underwear that is too tight should be minimized, as it can disrupt the local pH balance. 75 Even though disposable pads can be used as a preventative measure, prolonged contact with the genital area can cause discomfort and raise the risk of genital infections in women who have urinary incontinence. When the kind and amount of absorbent materials alter during menstruation, the risk of infection increases. Studies show that prefabricated pads, as opposed to diapers, are linked to a decreased risk of genital infections; Nevertheless, continuous daily use of pads seems to elevate the risk of infection. Additionally, the entire pubic area should not be shaved, as soreness, cuts, and nicks can attract microbes. Hence, pubic hair provides a protective barrier, and if shaving is deemed necessary, using scissors is a safer choice than opting for razors or strong hair removal creams. 73
Novel and non-antibiotic preventive approaches in urinary tract protection
Antibiotics are commonly used to treat UTIs, which are among the most prevalent bacterial illnesses, particularly in women and children. The world’s capacity to cure diseases in the future is threatened by the alarming increase in antibiotic resistance. Therefore, there is an urgent need for new techniques. UTIs can be avoided with the help of the innate immune system. Innate immunity includes antimicrobial peptides as a key component. Produced by neutrophils and epithelial cells, they protect the urinary system from bacteria that invade it. 79
Antimicrobial peptides
All throughout the body, epithelial cells express antimicrobial peptides, but immune cells also create them. Their antimicrobial activity offers prompt protection against a range of diseases, even though they also contribute through immune-modulatory aspects or other activities against the pathogens. There are several AMPs found in the upper and lower urinary tract. 80 Although human β-defensins (hBDs) are known to be expressed in the urogenital tract, little is known about how they function during UTI. Numerous epithelia throughout the body constitutively express hBD1, with the kidney exhibiting the highest levels of expression and the bladder’s epithelial cells exhibiting the lowest levels. 81 Human patient studies indicate that hBD1 may be involved in acute pyelonephritis, but its function in lower urinary tract defense is less clear. In contrast to the constitutive expression pattern of hBD1, hBD2 is only expressed in response to inflammatory stimuli and has been detected in chronically infected kidneys. 82
The digestive tract has been the primary site of investigation for another class of defensins, known as the α-defensins. However, human α-defensin 5 has recently been shown to be present and active in the urinary tract as well. 83 Other peptides suppress bacteria by reducing nutrients, especially iron. Hepcidin is a crucial regulator of iron homeostasis and may also directly inhibit E. coli bacteria. 84 In response to infection, renal lipocalin 2 is increased and helps protect the lower urinary tract. The renal-specific protein called uromodulin, often referred to as Tamm-Horsfall protein, stops E. coli and other pathogens from sticking to the host cells in the lower urinary tract.85,86
The role of cathelicidin and interaction of LL-37 with bacterial biofilm in the urinary tract
Similar to other AMPs, human cathelicidin is produced as an inactive precursor that includes a signal peptide and the propeptide hCAP18. 87 Following cleavage, the 37-amino acid antimicrobially active peptide—which is known as LL-37—begins with two lysine residues. At various bodily locations, additional cleavage products with unique antibacterial properties may be produced. 88 At sub-inhibitory concentrations, LL-37 has been shown to influence the biofilm formation of several bacterial species. In certain instances, LL-37’s direct interaction with microbial surface structures could be the cause. 89 By affecting quorum-sensing systems, LL-37 decreased biofilm formation in Pseudomonas aeruginosa, resulting in elevated twitching motility and decreased bacterial attachment. 90 Through a direct interaction between the AMP and CsgA, the primary curli fiber subunit, LL-37 inhibits curli-dependent biofilm in E. coli. By binding to monomeric CsgA, LL-37 prevents polymerization, which in turn prevents curli from forming, which in turn lessens the formation of biofilms. 91 Nevertheless, the peptide’s bactericidal activity is neutralized when LL-37 binds to curli fimbriae that have already formed on the bacterial surface.
Prevention of colonization by estrogen
After menopause, only 25% to 30% of women have lactobacilli in their vagina. This percentage could increase to 60% or even 100% with estrogen replacement therapy. A study found that intravaginal estrogens significantly reduced the recurrent UTI incidence in postmenopausal women. The study found that after 1 month of treatment, 22 out of 36 women in the estrogen group had intravaginal lactobacilli, compared to zero in the placebo group. The percentage of women with Enterobacteriaceae colonization in their vaginas decreased from 67% to 31% in the estrogen group, and the vaginal pH decreased from 5.5 to 3.8. 92 In contrast to the placebo group, the estrogen group experienced fewer UTIs. Oral estrogens are associated with coronary heart disease, stroke, venous thromboembolism, and breast cancer; however, they did not lower the incidence of UTIs. Therefore, to prevent recurrent UTIs, postmenopausal women are not advised to use oral estrogens. 93
Prevention of adherence by cranberries
For many years, cranberries have been used to prevent UTIs. The exact mechanism of action has not yet been determined. According to in vitro studies, cranberries are thought to contain proanthocyanidins (PACs), which can stop P-fimbriated E. coli from attaching to the uroepithelial cell receptors. 94 It’s unknown what the ideal PAC formulation, dosage, and concentration are. Early research on cranberries did not standardize the chemical makeup of the items that were available, nor did it adequately characterize the dosage. Cranberry products that have been standardized by PAC have been used in more recent studies.
In women with recurrent UTIs, when compared to placebo/control, cranberry products were observed to significantly reduce the incidence of UTIs at 12 months (RR 0.65, 95% CI 0.46–0.90). A more recent version of this Cochrane analysis, however, found that cranberry products did not significantly reduce the risk of symptomatic UTI in women with recurrent UTIs. This discrepancy results from their meta-analysis’s inclusion of two extra trials. 95 According to studies, eating cranberries can reduce the symptoms of UTIs rather than their recurrence rates. Two studies were conducted to investigate the effectiveness of cranberry extract and low-dose antibiotic prophylaxis. In avoiding recurrent UTIs in older women, the researchers discovered that TMP had a small advantage over cranberry extract, based on a study involving 137 women who had received antibiotic treatment for two or more UTIs in the preceding 12 months. 96 A more recent trial found that low-dose (480 mg) TMP-SMX is more effective than cranberry capsules in preventing recurrent UTIs in premenopausal women. However, cranberries did not cause the commensal flora to include more resistant microorganisms than low-dose TMP-SMX did. 97
Vaccination
Although most vaccines to prevent recurrent UTIs are still in the development stage, a number of them seem promising. In multiple studies, the oral vaccination MV140 has demonstrated good efficacy in preventing recurrent UTIs with minimal side effects and safety data. MV140, a polyvalent, bacterial, whole-cell-based sublingual vaccine, has been created. It is currently authorized for use in 26 countries and offered to specified patients. The systematic review identified five observational studies that evaluated the vaccine’s effectiveness in preventing rUTIs in women. Those who received the immunization had 32% to 90% UTI-free rates, according to the report. A total of 240 women with rUTI participated in a European trial that demonstrated the vaccine’s safety and effectiveness. During the 9-month effectiveness period, the vaccine drastically reduced the number of UTI episodes from a median of 3.0 to 0.0 when compared to the placebo. 98 It has recently shown efficacy over 9 years after the initial dose in a preliminary long-term investigation. The heat-inactivated strains of Proteus vulgaris, E. coli, K. pneumoniae, and E. faecalis included in MV140 alter the bladder’s local immune response and cause the development of host antibodies. The vaccine is currently accessible in some nations across the world, including Australia, Chile, the Dominican Republic, Lithuania, Mexico, the Netherlands, New Zealand, Norway, Portugal, Spain, Sweden, and the United Kingdom, despite not being authorized for use in the USA or Canada. 19
Preventive stewardship: Managing antibiotic use in CKD patients with UTI history
Globally, the prevalence of CKD is rising, and there is a greater chance that it may progress to ESKD. Patients with kidney allograft dysfunction, stage 2 to 5, and ongoing chronic dialysis treatment are more susceptible to sepsis and other infections, such as UTIs. These individuals have poor immunocompetence, persistent inflammation, and metabolic disturbances. Although other organisms may be implicated, E. coli is the most frequent cause of UTIs. Antimicrobial resistance is exacerbated by drugs, urological procedures, and catheterization. 58 The principles used to prevent UTIs in people with renal insufficiency are largely the same as those used for those with normal renal function. 99
Without recurrence or the emergence of resistant germs, UTIs should react quickly. Tubular secretion and reabsorption, glomerular blood flow and filtration, and antibiotic bioactivation and metabolism are all impacted by acute and chronic kidney disorders. Certain aspects of CKD, particularly hemo and peritoneal dialysis, might change drug absorption, bioavailability, protein binding, distribution volume, and nonrenal clearance (metabolism). 100
Most individuals with early CKD have normal or elevated urine volumes. Patients who receive dialysis for years often have oliguria, a condition in which the volume of urine that remains gradually decreases until (oligo-)anuria. However, in this case, oliguria is coupled with decreased urine concentration, which is also observed in polyureic acute renal failure (stage 3,4,5/K/DOQI staging system). Dialysis patients will not achieve adequate antibiotic concentrations even if they continue to produce urine. 101 Rare reports exist that intravenous antibiotic treatments (cephalosporins, aminoglycosides, carbapenems) for recurrent UTIs in anuric patients have been effective. 102
CKD patients can use antibiotic selection and indication based on their specific condition. Renal impairment may alter how some antibiotic medications work, particularly for treating UTIs. Proper antibiotic concentrations in the kidneys and urine are necessary for their therapy, but, as GFR declines, these concentrations may drop and become insufficient. For example, when treating UTIs in patients with CKD, sulfamethoxazole or nitrofurantoin monotherapy should be avoided because urine concentrations are too low. 103
When compared to Standard Practice (SPC), dosage regimens for patients with normal kidney function are frequently higher. Daptomycin dosages, for instance, range from 4 to 6 mg/kg/day for patients with normal renal function; when the GFR drops below 30 mL/min, the dosage is lowered by 50%. Regardless of the severity of the infection, these dosages are deemed insufficient. However, the majority of guidelines suggest dosages between 6 to 8 mg/kg and 10 to 12 mg/kg each day. 104 When the GFR falls below 30 mL/min, a rule of three could be used to reduce larger doses in CKD patients by 50%. However, safe and efficient use can only be guaranteed by clinical evidence from these particular patients. An antibiotic that works well at a lower dosage in one indication may become toxic or ineffective at a greater dosage in another due to the nonlinear nature of medication pharmacokinetics. According to studies, patients with CKD and dialysis should get 10 mg/kg every 48 h.
Certain antibiotics, such as tedizolid, don’t have any major pharmacokinetic alterations in CKD patients, so their dosage doesn’t need to be changed. 105 Ceftriaxone and doxycycline, however, can be taken at doses of up to 4 g per day without modification. With a significant risk of ineffectiveness from dose adjustments for renal function, overdosing is often advantageous. 106
To evaluate the efficacy and toxicity of all antibiotics, particularly those with a narrow therapeutic index, pharmacological therapeutic follow-up is necessary for CKD patients. This includes measuring plasma levels for each antibiotic. Considering the infection site, severity, bacteriological evidence, and ecological impact, non-nephrotoxic antibiotics without dose modification ought to be the preferred option. Antibiotics with a broad therapeutic index or known dose changes that are simple to monitor should be chosen if needed. Avoid using empirical prescriptions to prevent the dangerous side effects of either an excessive or insufficient dosage. Within 48 to 72 h, these suggestions should be reassessed in light of the patient’s clinical presentation and concomitant comorbidities. It is important to keep a careful eye on tolerance. 107
Genetic screening for infection susceptibility in renal patients in a preventive way
Genetics must be emphasized since UTIs, particularly recurrent UTIs, are known to frequently exhibit familial aggregation. 108 The innate immune system defends the urinary tract, and innate signaling pathways regulate the risk of UTIs. These pathways can be altered in certain people by various genetic polymorphisms. 108 These include genes that alter toll-like receptor (TLR) expression, which is essential for defending the urothelium against urinary pathogens by inducing the innate immune response.
Numerous TLR polymorphisms can either enhance or decrease their functionality. Endothelial and epithelial cells are among the many antigen-presenting cells that contain TLRs, which are two-domain transmembrane protein molecules. TLRs identify pathogen-associated molecular patterns once the pathogen has entered the urinary system, which triggers a series of inflammatory reactions aimed at getting rid of the invader. 109 Consequently, pro-inflammatory molecules such as TNFα, interleukin 1β (IL-1β), and interleukin 12 (IL-12) are released in greater amounts. 110 However, when systemic infections with Gram-negative bacteria occur, this impact is not necessarily protective for the host. Due to TLR4’s recognition of the lipopolysaccharide on leukocytes and renal cells, TNFα and IL1 are released, which can accelerate the development of AKI and all of its consequences. 110 Humans’ defense against UTIs is mostly mediated by TLR2, TLR4, and TLR5. 109
Another interesting discovery is that polymorphisms related to VEGFA and TGFβ1 were associated with kidney scarring after UTIs and progressive kidney disease, namely Vesico-ureteral reflux. TGFβ1 and VEGFA are key players in tissue regeneration following various forms of injury, and polymorphisms such as the TGFβ1-promoter’s C-509 T allele or the VEGF gene’s −460 CC were more commonly linked to kidney scarring and UTIs. 111 However, since they don’t seem to be a risk factor for recurring UTIs either, we can conclude that, even in people with these genetic variants, preventing UTIs can lower the likelihood of progression. 112 Furthermore, the homozygosity of the VEGF-A gene’s C allele has been linked to hypodysplastic renal parenchymal lesions in children with UTIs. Last but not least, a local inflammatory response to UTIs is largely provided by CXC chemokines and their receptors. 113
UTIs, especially in children, can be connected to variations in the interleukin 8-receptor (CXCR1), a crucial chemokine receptor that is involved in neutrophil recruitment and, consequently, in the innate immune system’s efficient operation. 114 However, given the contradictory evidence, more investigation is required. Furthermore, it was discovered that, at least in premenopausal women, a low level of CXCR2 was linked to an increased risk for UTIs. 115
The hallmark of CKD is a persistent pro-inflammatory state that raises TNFα and IL-6 levels and increases CD4+ T cell death. There is no defense mechanism against uropathogens provided by these variables. TNFα and IL-6 have an impact on leukocytes, which results in decreased neutrophil activity, inhibited diapedesis, and altered endothelial function because of uremic toxins.58,116 These toxins have the ability to change endothelial function, which can lead to leukocyte migration to the wounded area and a loss of phagocytic function. The clearance of germs and viruses is further lowered by elevated TNFα and IL-6 levels, which similarly raise the threshold of reactive oxygen species and decrease macrophage recruitment. Research has indicated that hospitalization risk for severe infections, including UTIs, is closely associated with TNFα, IL-6, and C-reactive protein.117,118
The kidney and urinary tract’s inherent defense is a complicated, multifaceted process. A number of elements cooperate to stop and eradicate invasive diseases right away. There is still much to learn, even though a number of noteworthy mutations in known critical components have been found. To determine the whole innate defense milieu that could be targeted for innovative treatments in the prevention or treatment of UTIs, well-phenotyped cohorts of these illnesses and genome-wide studies are required. 119
Nutritional and lifestyle interventions to prevent infection-driven renal decline
Globally, CKD is becoming more prevalent; in 2019, it ranked as the 18th leading cause of disability-adjusted life years. 120 It’s critical to implement strategies that stop CKD from developing and getting worse. Despite advancements in identification and treatment, preventative care is still essential for kidney disease, where non-pharmacological therapies have demonstrated potential advantages, such as lifestyle modifications including exercise and food advice. 121 Lifestyle factors, including eating more vegetables, exercising more, consuming less salt, and drinking less alcohol, are associated with primary prevention of CKD. 122
The management of CKD heavily relies on measures that try to slow the disease’s course and lower disease-specific mortality. The importance of a balanced diet in the management of CKD was recognized by scientists in the late 1800s when they found that protein restriction decreased the signs and symptoms of uraemia. 123
DM and HTN are the two major risk factors for CKD -related conditions. Nephrotoxins, kidney stones, systemic diseases, and environmental factors are additional risk factors. 124
Lifestyle modifications: Physical activity, weight loss, and smoking
A retrospective cohort analysis discovered a strong association between a high body mass index (BMI) starting at 25.0 kg/m2 and the risk of ESRD. Additionally, CKD incidence is correlated with central (waist circumference) and overall obesity in a graded causative manner.125,126 Again, the Physical Activity Guidelines for Americans state that for major advantages, people should do at least 150 min of moderate-intensity physical activity or 75 min of strenuous exercise every week. In people with chronic kidney illness, physical activity was problematic since it may lead to increased proteinuria and reduced renal function. Conversely, low-intensity exercise enhances quality of life but has no effect on renal function. 127
Another prospective cohort study found that for individuals with stage 3 to 4 CKD, an additional 60 min of physical activity per week was linked to an estimated 0.5% slower annual decline in eGFR. The same study also found that patients who did not engage in leisure-time physical activity had a higher annual decline in GFR than patients who engaged in physical activity that was advised by guidelines; after controlling for sociodemographic factors and common diseases, the annual eGFR of patients who did not engage in leisure-time physical activity and those who engaged in at least 150 min per week of leisure-time physical activity decreased by 2.8%. 128 Walking was the favored form of exercise for most people with stage 3 to 5 CKD (mean age: 70 years). Regardless of patients’ age, renal function, or comorbidities, the study found that walking was associated with lower overall mortality and RRT rates. 129
In line with the findings of these research, physical activity may help older persons slow the rate at which their kidney function declines and reduce their chance of developing ESRD. The sub-distribution hazard ratio (SHR) for walking is 0.83, p = 0.04 for patients who walked 1 to 2 times per week, 0.72, p = 0.002 for patients who walked 3 to 4 times per week, and 0.41, p < 0.001 for those who walked ⩾7 times per week. These findings indicate that walking is linked to a dose-dependent risk of overall mortality. Furthermore, there is a dose-dependent reduction in renal replacement therapy due to walking (SHR: 0.81 for patients who walked 1–2 times per week and 0.56 for those who walked 5–6 times per week). Further study is required to establish the minimum level of physical activity required to slow the progression of CKD. 130
Another evaluation of the causes and effects of smoking is challenging. Smoking, however, is linked to a worse course of CKD in people who already have it. Three-year follow-up prospective cohort research conducted in Korea found that smoking is associated with a higher risk of CKD development. Benefits were mainly apparent in those with eGFRs below 45 mL/min/1.73 m2. 131
Nutritional interventions
Protein intake is one of the most talked-about topics in CKD diet therapy. It has been shown that kidney function is significantly impacted by a diet high in protein (defined as >1.2 g/kg/day). 132 For the treatment of patients with CKD, LPD provides a number of benefits by reducing intraglomerular pressure, which in turn reduces nitrogen waste products and renal strain. This safeguards the kidneys, particularly in people whose functioning nephron reserve is diminished. 133 On kidney physiology, LPD and renin-angiotensin-aldosterone system (RAAS) blockades have similar effects. A study found that blockades of RAAS and LPD had an additive anti-proteinuric effect. 134
For stable individuals with non-dialysis stage 3 to 5 CKD, the 2020 Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines propose 0.55 to 0.60 g/kg/day of protein. This can be reduced to 0.28 to 0.43 g/kg/day if they are fed with necessary amino acids and 7 to 15 g/day of keto-acid analogues (KA). When combined with KA supplementation, dietary protein restriction is likely to be beneficial for patients with stage 3 to 5 CKD overall. A moderate sodium restriction of 2.3 g per day should also be followed by CKD patients in addition to the current pharmaceutical strategies to improve volume control, lower BP, and lessen proteinuria. 135
Acidosis is a major risk factor for the development of CKD. According to a study, using fruits and vegetables as an oral alkali may lower the risk of HTN and volume retention associated with taking bicarbonate supplements. Dieticians for the study recommended eating two to four cups of fruits and vegetables every day. 136 A very low protein diet that was high in fruits and vegetables and supplemented with essential amino acids and KA of non-essential amino acids notably decreased net endogenous acid production by 53% at 6 months and 67% at 12 months, as well as potential renal acid load by 120% at 6 months and 138% at 12 months, according to another case-control study. 137
Limitations
It is important to take into account the various intrinsic limitations of the current narrative literature review when evaluating its results. Firstly, being a narrative review, it compiles available data rather than carrying out original empirical research, making its conclusions reliant on the quality, breadth, and potential biases of the primary studies included. Secondly, some associations may be influenced by publication bias, as studies yielding statistically significant or positive outcomes tend to have a higher likelihood of publication. Thirdly, the studies reviewed exhibit considerable diversity in their methodological approaches, including observational research, clinical trials, and laboratory studies conducted across various geographic locations and patient populations. This variation complicates the ability to make direct comparisons and perform quantitative analyses through meta-analysis, limiting the applicability of certain findings. Variations in methodology among the studies reviewed create challenges in making direct comparisons and hinder the potential for quantitative meta-analysis. This diversity has been validated by the three clinical studies summarized in section “Some clinical investigations on the interrelationship between urinary tract infections and chronic kidney disease.” These studies employ different designs (retrospective vs cross-sectional observational) and focus on varying patient populations across distinct geographic areas. While these factors contribute to a richer evidence base, certain parameters cannot be generalized to the entire CKD population worldwide, such as the prevalence of multidrug-resistant organisms or the most frequently encountered pathogens. Furthermore, even though these studies were selected for illustration purposes, they may not encompass all relevant reports on the topic. Consequently, the conclusions of the review depend on the quality of the primary studies utilized and the potential biases present in those studies. Although the bibliographic search aimed to be thorough, there remains a possibility of overlooking relevant studies, particularly those published in languages other than English or those that remain unpublished. Lastly, the field of non-antibiotic therapy and antimicrobial resistance is rapidly evolving; therefore, new findings may have emerged since the completion of this review that could alter some of the conclusions or recommendations presented here.
Conclusion
The slow advancement of UTIs to CKD, alongside the growing issue of antibiotic resistance, presents a critical and complex clinical challenge. There exists a structured relationship in which CKD makes patients more susceptible to severe and recurrent UTIs, while recurring infections further aggravate kidney decline. Patients with diminished immune function are especially vulnerable to multidrug-resistant uropathogens, leading to prolonged hospital stays and frequent exposure to antibiotics; this connection has been firmly linked to the frequency of treatment failures and the eventual progression to ESKD. Thus, effective management must involve a comprehensive and proactive strategy that goes beyond the traditional focus on antibiotics. Prevention plays a key role, which can be enhanced through educational initiatives regarding urogenital hygiene and lifestyle changes to bolster systemic resilience, as well as by integrating speculative, non-antibiotic preventative strategies such as vaccines and antimicrobial peptides. When a UTI occurs, strong antibiotic stewardship is crucial: selecting an effective and non-nephrotoxic agent, adjusting the dosage for renal impairment, and promptly de-escalating treatment once culture results are available. Addressing UTIs in CKD and conducting early systematic screening for CKD among high-risk populations are vital for facilitating timely treatment. Future prevention efforts may also include genetic testing to identify individuals more susceptible to infections or the development of renal scarring. Breaking the harmful cycle of UTI and CKD will require a collaborative effort among clinicians, researchers, and patients committed to preserving kidney function and enhancing the long-term prognosis for this vulnerable population.