
Abstract
Background:
It is well-known that patients with chronic kidney disease and end-stage renal disease are at increased risk of pulmonary embolism than patients with normal kidney function. However, the data on trends, outcomes, and predictors of mortality in pulmonary embolism patients with chronic kidney disease and end-stage renal disease in the United States are limited.
Methods:
We queried the National Inpatient Sample database from 2010 to 2014. International Classification of Diseases-Ninth Revision-Clinical Modification codes were used to identify patients with normal kidney function, chronic kidney disease, and end-stage renal disease. The frequency of pulmonary embolism, complications, in-hospital mortality, and length of stay were calculated for each cohort. Multivariable logistic regression models were constructed to determine the predictors of mortality.
Results:
In the study population (2010–2014), there were 766,176 pulmonary embolism hospitalizations with normal kidney function, 79,824 with chronic kidney disease, and 9147 with end-stage renal disease. Among the study cohorts, the mortality rate was 2.7% in normal kidney function, 4.5% in chronic kidney disease, and 6.8% in end-stage renal disease hospitalizations. Median length of stay was highest in the end-stage renal disease cohort and lowest in the normal kidney function cohort. After adjusting for confounders, pulmonary embolism patients with chronic kidney disease died 1.15 times more often than those with normal kidney function and pulmonary embolism patients with end-stage renal disease died 4.2 times more often than those with normal kidney function.
Conclusion:
The mortality rate and length of stay in pulmonary embolism patients with chronic kidney disease and end-stage renal disease were significantly higher than those in pulmonary embolism patients with normal kidney function. Also, pulmonary embolism patients with chronic kidney disease and end-stage renal disease were at higher risk of in-hospital mortality than those with normal kidney function. There was statistically significant higher risk of mortality in elderly and Black patients with pulmonary embolism and concurrent chronic kidney disease or end-stage renal disease.
Introduction
Previous studies have shown that chronic kidney disease (CKD) and end-stage renal disease (ESRD) patients are at an increased risk of venous thromboembolism (VTE) and pulmonary embolism (PE).1–3 The probable pathways leading to increased incidence of VTE in CKD and ESRD patients are discussed below: 4
Activation of procoagulants.
Decreased endogenous anticoagulants.
Decreased activity of fibrinolytic system.
Increased platelet activation and aggregation.
CKD is associated with an increased level of C-reactive protein (CRP),
According to a study by Tveit et al., 3 the overall incidence rate of PE was 149.9/100,000 dialysis patients compared with 24.6/100,000 normal kidney function (NKF) patients in the US population in 1996. Also, they noted that chronic dialysis patients had a high risk for developing PE, independent of comorbidity. Longitudinal Investigation of Thromboembolism Etiology (LITE) study evaluated VTE risk in the non-dialysis, non-transplant CKD population. 11 It found that CKD was associated with increased risk of future VTE, with progressive increase in incidence rates per 1000 person-years with worsening CKD stage. 11 Kumar et al. 1 studied outcomes of PE in CKD and ESRD patients using the National Inpatient Sample (NIS) database from the year 2007. They found that the annual frequency of PE was 527 per 100,000; 204 per 100,000; and 66 per 100,000 persons with ESRD, CKD, and NKF, respectively, in year 2007. Also, in-hospital mortality was significantly higher for patients with ESRD and CKD in comparison with NKF. However, multi-year data on PE incidence in CKD and ESRD patients from a nationally representative sample are lacking in the United States. Thus, we conducted this study. 1
Methods
Data source
Ours is a retrospective observational cohort study. We obtained data from the 2010 to 2014 NIS database files. The NIS files are published on a yearly basis by the Agency for Healthcare Research and Quality (AHRQ) under the Healthcare Cost and Utilization Project (HCUP). 12 In the United States, it is the largest publicly available all-payer inpatient database and contains approximately 20% sample of the discharges from the community hospitals in the United States.12,13 HCUP 14 provides discharge weights for each record, which are utilized to obtain national estimates.
Study population
We did not use any calculation for obtaining a particular sample size for our study. The sample size for each year’s NIS data set is predetermined by HCUP. 12 Figure 1 depicts the sequential derivation of our study population. We used International Classification of Diseases-Ninth Revision-Clinical Modification (ICD-9-CM) codes 415.11 and 415.19 to identify hospitalizations with a primary discharge diagnosis of PE. We excluded hospitalizations with age less than 18 years. We also excluded patients with renal transplant (ICD-9-CM codes: V42.0 and 996.81) from our study cohort. We then used ICD-9-CM codes to classify each patient as having CKD, ESRD, or NKF. We identified CKD patients using codes 585.1–585.5 and 585.9. This estimated glomerular filtration rate (eGFR)-based staging of CKD diagnosis is according to 2002 guidelines established by the National Kidney Foundation (NKF) 15 Kidney Disease Outcomes Quality Initiative (KDOQI). We identified patients as having ESRD if they had diagnosis code for CKD requiring long-term hemodialysis (585.6) or the procedure codes for hemodialysis (39.95) or peritoneal dialysis (54.98). We excluded persons undergoing dialysis for acute kidney injury (AKI) (codes 584.5–584.9). Patients without CKD or ESRD were assigned to the no NKF group. This methodology has been previously used to correctly identify patients with CKD or ESRD from the NIS database.1,16,17 ICD-9-CM codes for chronic renal insufficiency have a sensitivity of 81.9%, specificity of 98.6%, positive predictive value (PPV) of 71.2%, and negative predictive value (NPV) of 99.2% when used for administrative databases.16,18

Study population.
Patient and hospital characteristics
Baseline patient-level characteristics were demographics (age, sex, and race) and relevant comorbidities (cancer, chronic obstructive pulmonary disease (COPD), cirrhosis, congestive heart failure, coronary artery disease, diabetes mellitus, hypercoagulable state, hypertension, morbid obesity, and smoking). We have included a list of ICD-9-CM, Clinical Classification Software (CCS) codes, and procedural codes used to identify the disease cohorts and comorbidities in Supplement 1.
Statistical analysis
Baseline patient-level characteristics of patients with CKD or ESRD were compared to those with NKF using the chi-square test for categorical variables and Student’s t test for continuous variables. After adjusting for confounding factors, multivariable logistic regression models were compiled to determine the predictors of mortality among the three cohorts, using the NKF group as the reference. Categorical variables were denoted in terms of frequency/percentage and continuous variables were denoted in terms of mean ± SD or median (interquartile range). Odds ratios (ORs) and 95% confidence intervals (CIs) were used to report the findings of regression models. P value less than 0.05 was considered statistically significant. We utilized SAS 9.3 (SAS Institute, Cary, NC, USA) for the analysis. Given that NIS is a publicly available limited data set, this study was exempt from a review by an institutional review board (IRB). 19
Endpoints
Primary outcomes were frequency of PE, length of stay (LOS), all-cause in-hospital mortality, disposition status in patients surviving the hospitalization, and complications (respiratory failure requiring mechanical ventilation and cardiac arrest). Secondary outcomes were predictors of mortality.
Results
Patient and hospital characteristics
Out of 859,335 adult hospitalizations with PE, 766,176 had NKF (89.1%), 79,824 had CKD (9.3%), and 9147 had ESRD (1%). PE patients with CKD were more likely to be older when compared with ESRD patients (mean age 73.2 ± 12.9 years versus 59.3 ± 17.0 years). Patients with ESRD were more likely to be males and of African American descent when compared to patients with CKD. Cancer, COPD, coronary artery disease, morbid obesity, and smoking were more prevalent in patients with CKD, whereas cirrhosis, congestive heart failure, diabetes mellitus, and hypertension were more prevalent in patients with ESRD. Hypercoagulable state and smoking were prevalent more in NKF patients than in CKD/ESRD patients. Charlson-Deyo’s comorbidity index (CCI) score of ⩾3 was more common in CKD/ESRD patients, whereas score of ⩽2 was more common in NKF patients (Table 1).
Baseline characteristics of PE hospitalizations with NKF, CKD, or ESRD.

NKF: normal kidney function; CKD: chronic kidney disease; ESRD: end-stage renal disease; COPD: chronic obstructive pulmonary disease; CCI: Charlson-Deyo’s comorbidity index.
In-hospital outcomes
Median LOS was higher in ESRD patients than in CKD patients (6 days versus 5 days). Median LOS was lowest in NKF patients. Most patients from all the groups were discharged to home. CKD patients were more likely to be discharged to nursing home than ESRD patients (22.9% versus 17.9%). Also, CKD patients were more likely to require home health care (HHC) than ESRD patients. The mortality rate was higher in ESRD patients (6.8%). ESRD patients with PE were more likely to require mechanical ventilation than CKD patients with PE (8.8% versus 7.7%). NKF patients with PE were least likely to require mechanical ventilation (4%). Rate of cardiac arrest was higher in ESRD patients than in CKD patients (2.7% versus 1.2%) (Table 2).
Outcomes in PE hospitalizations with NKF, CKD, or ESRD.

PE: pulmonary embolism; NKF: normal kidney function; CKD: chronic kidney disease; ESRD: end-stage renal disease; LOS: length of stay; HHC: home health care; AMA: against medical advice; MV: mechanical ventilation; NIV: non-invasive ventilation.
Predictors of mortality
After adjusting for confounders in PE patients, CKD patients were at 1.15 times higher risk of mortality than NKF patients (OR 1.15; CI 1.05–1.26; P = 0.002) and ESRD patients were at 4.2 times higher risk of mortality than NKF patients (OR 4.22; CI 3.65–4.88; P < 0.0001). When compared to the age group 18–44 years, all other age groups had higher odds of mortality. PE hospitalizations with age above 75 years were at highest risk of death (OR 3.17; CI 2.78–3.63; P < 0.0001). There was no significant association of risk of mortality with the sex of patients. When compared to Whites, African Americans (OR 1.25; CI 1.15–1.35; P < 0.0001), Hispanics (OR 1.15; CI 1.01–1.31; P = 0.04), and Asians (OR 1.62; CI 1.17–1.69; P = 0.0003) were at higher risk of mortality (Table 3). Based on univariate and multivariate analyses, we found that the odds of mortality increased significantly with successive increase in the CCI score for CKD patients (Tables 4 and 5). However, this effect was not observed in ESRD patients (Tables 4 and 5).
Predictors of mortality in PE hospitalizations with CKD or ESRD.

PE: pulmonary embolism; NKF: normal kidney function; CKD: chronic kidney disease; ESRD: end-stage renal disease; COPD: chronic obstructive pulmonary disease.
Univariate analysis for predictors of mortality in PE hospitalizations with CKD or ESRD based on CCI.
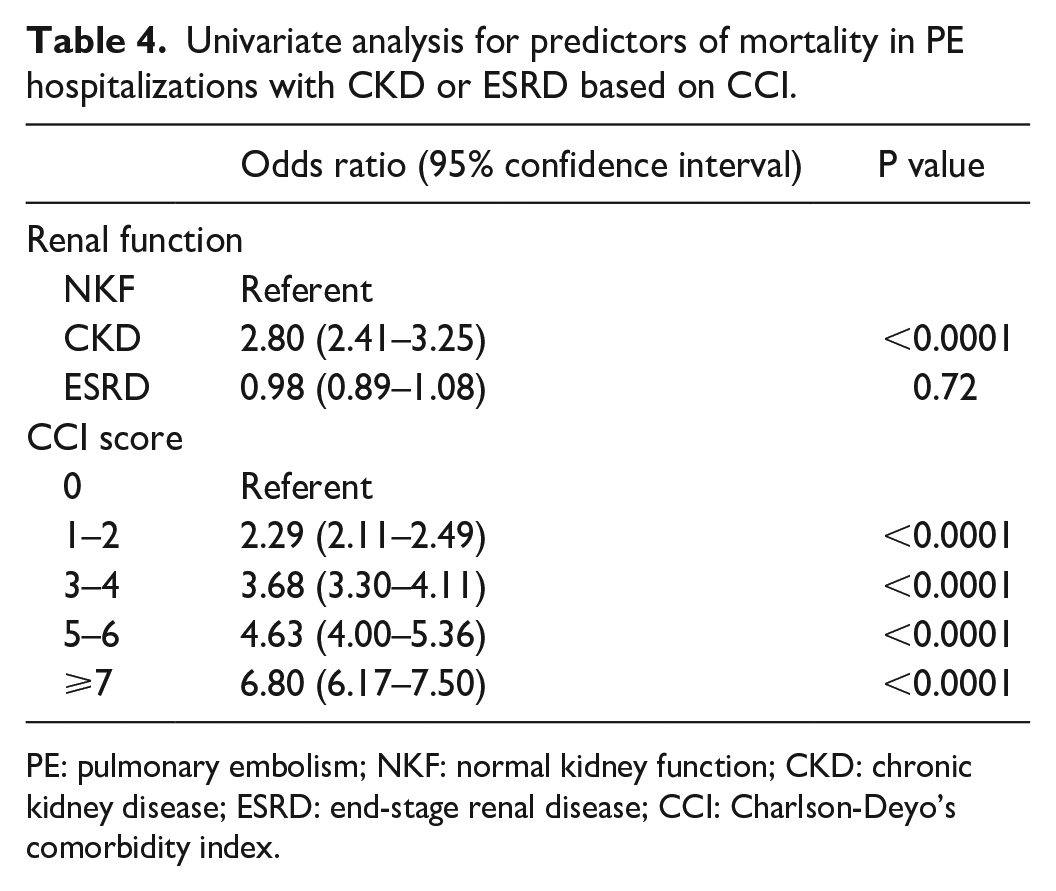
PE: pulmonary embolism; NKF: normal kidney function; CKD: chronic kidney disease; ESRD: end-stage renal disease; CCI: Charlson-Deyo’s comorbidity index.
Multivariate analysis for predictors of mortality in PE hospitalizations with CKD or ESRD based on CCI.

PE: pulmonary embolism; NKF: normal kidney function; CKD: chronic kidney disease; ESRD: end-stage renal disease; CCI: Charlson-Deyo’s comorbidity index.
Discussion
Our study found that significant proportion of patients hospitalized with PE have impaired kidney function (CKD and ESRD), which can be explained physiologically by procoagulant state in patients with CKD secondary to increase in fibrinogen, von Willebrand factor, VIIa and XIIa, and decrease in plasminogen activator inhibitor-1 (PAI-1).20,21 Use of erythropoietin is common in ESRD which increases thrombosis risk. 22 In addition, hyperhomocysteinemia in ESRD due to uremia causes endothelial dysfunction which leads to alteration of Virchow’s triad. 23 The increased thrombophilic state has been found to be reversed after kidney transplantation in patients with CKD stage-5. 24
We found that hypercoagulable state and smoking were more common in NKF patients than in CKD/ESRD patients. There are several reasons for these findings. ESRD patients receive heparin during their dialysis sessions. We believe that this is the likely reason behind lower prevalence of hypercoagulable state in ESRD patients. Also, CKD patients are more likely to be on anti-platelet agents and anti-coagulant agents due to their co-existing comorbidities than NKF patients. ESRD patients are not considered transplant candidates if they are actively smoking. Thus, they are more likely to quit smoking than NKF patients. ESRD and CKD patients get reinforcement for smoking cessation during dialysis visits and nephrology office visits.
In our study, CKD patients with PE were more likely to be discharged to nursing home than ESRD patients. This may be because of lesser availability of nursing homes equipped with hemodialysis facilities. CKD patients were more likely to require HHC than ESRD patients. ESRD patients visit their dialysis centers thrice a week and get comprehensive care from a team of physicians, nurses, social workers, and case managers. This is the likely cause for ESRD patients not requiring HHC as much as CKD patients.
In 2020, a meta-analysis involving more than 225,000 patients found that renal insufficiency is a predictor of short-term and long-term mortality and adverse outcomes in acute PE patients. 25 Another 2020 study by Goto et al. 26 noted that moderate to severe CKD was associated with increased risk of mortality, VTE recurrence, and major bleeding compared with the presence of mild to no CKD. In our study, patients with CKD and ESRD were found to have 1.15 and 4.2 times higher risk of in-hospital mortality, respectively, when compared to patients with NKF. Patients with ESRD also had a high rate of complications like the need for mechanical ventilation and cardiac arrest. Our findings are in alignment with previous NIS study by Kumar et al. 1 where the mortality rate of PE among patients with NKF was 3.2% compared to 6.7% for patients with CKD and ESRD. In contrast, one of the studies done in Italy showed that hospital mortality of patients with PE among NKF, CKD, or ESRD was not statistically different. Instead, it was independently related to age and gender, and comorbidities like hypertension, diabetes mellitus, dementia, peripheral vascular disease, and cancer. 27 It is possible that this finding could have been confounded by the associated comorbidities. Undoubtedly, there are also other independent predictors for mortality from PE. We found that the odds of mortality increased significantly with successive increase in the CCI score for CKD patients but not for ESRD patients. The explanation behind these findings is not well understood. Pulmonary Embolism Severity Index (PESI) score is used for prediction of outcome for PE which includes age, sex, underlying heart failure, lung disease with clinical parameters of hypotension, tachypnea, and hypoxia. 28 From a multicenter Brazilian cohort study, hospitalized PE patients with age more than 65 years were seen to have increased risk of death. 29 Similarly, in our study, PE patients with CKD and ESRD older than 75 years were at the highest risk of death. In our study, Blacks were found to be at higher risk of death from PE when compared to Whites. This finding co-relates with 40% higher age-adjusted VTE incidence among Black population.30,31 Analysis of out-of-hospital PE data shows that Black population had the highest mortality but Hispanics and Asians had low mortality compared to Whites, whereas in a study of in-hospital data from New Jersey state, there was no statistical difference in mortality in PE patients in the Black and White population.32,33 Both, in general population and CKD/ESRD population, this finding can be blurred by availability to treatment, time of presentation, modality of treatment, and associated comorbidities.
Gender disparities have always been of special interest. Although incidence of PE has always been higher in female, results in terms of mortality outcome have been variable. Agarwal et al. 34 showed higher mortality in female (OR 1.09; 95% CI 1.03–1.15) in addition to higher rate of complications including the need for blood transfusion and occurrence of shock. Panigada et al. 35 found that there was no statistical difference for in-hospital mortality based on gender. We did not find gender-based differences in mortality risk for PE patients with CKD/ESRD.
With respect to in-hospital outcomes, LOS was highest in ESRD patients followed by CKD, with lowest LOS for patient with NKF. CCI is a method of predicting mortality within 1 year after hospital admission by classifying or weighting comorbid conditions. 36 It was noted to be higher with ESRD/CKD patients compared to patients with NKF. 37
Administration of contrast for diagnosis of PE with angiography adds to nephrotoxicity in CKD patients. Despite anticoagulants being indicated for management of PE, there is a lack of consistent evidence for safety and efficacy of anticoagulants in patients with GFR <30. Anticoagulant dose adjustment is necessary based on kidney function, and sometimes, there can be increased bleeding risk. A combination of the above-mentioned factors often creates a dilemma regarding anticoagulation management in these patients, which might itself prolong the hospitalization, mortality, and cost. Given the higher risk of mortality due to PE in CKD and ESRD patients, formulation of strategies for prevention of PE and risk–benefit analysis on its early treatment is essential.
Our study has several limitations. ICD-9 coding is unable to provide information regarding various stages of CKD to precisely estimate the mortality trends in each stage. NIS includes discharge-level data; thus, data from readmission of the same individual cannot be assessed which might have skewed the results. Since the data include admission with primary diagnosis of PE, patient who develops PE during hospitalization for other primary diagnosis is not included in the study. Due to the nature of the data, we were not able to study causal relationship of each predictor with inpatient mortality. Although potential confounding factors were controlled by multivariable regression, residual bias secondary to unmeasured severity of comorbidities is a possibility.
Conclusion
Our study is the first study with multi-year data on nationally representative sample looking into outcomes of hospitalized PE patients with CKD and ESRD. We found statistically significant higher mortality in ESRD and CKD patients when compared to patients with NKF. Similarly, there was statistically significant high risk of mortality in elderly and Black patients in PE patients with CKD and ESRD. There were no gender-based differences in mortality risk for PE patients with CKD and ESRD. LOS and mortality within 1 year after hospital admission were higher in CKD and ESRD patients with PE than in NKF patients with PE. Given that there is a lack of evidence for safety of anticoagulants in patients with GFR <30, prospective clinical studies are needed to identify appropriate type and dose of anticoagulants for PE patients with underlying CKD and ESRD. Future practice should focus on diagnosing, treating, and most importantly preventing PE among CKD and ESRD patients.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211022996 – Supplemental material for Pulmonary embolism in chronic kidney disease and end-stage renal disease hospitalizations: Trends, outcomes, and predictors of mortality in the United States
Supplemental material, sj-pdf-1-smo-10.1177_20503121211022996 for Pulmonary embolism in chronic kidney disease and end-stage renal disease hospitalizations: Trends, outcomes, and predictors of mortality in the United States by Jagmeet Singh, Sushmita Khadka, Dhanshree Solanki, Asim Kichloo, Harshil Shah, Manasee J Vyas, Savneek Chugh, Neil Patel and Shantanu Solanki in SAGE Open Medicine
Footnotes
Author contributions
S.S., J.S., and S.K. helped in conception and design. D.S. and J.S. provided administrative support. Provision, collection, and assembly of data were done by A.K. Data analysis and interpretation were performed by S.S., S.K., and A.K. All authors helped in manuscript writing and the final approval of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for this study because the Healthcare Cost and Utilization Project (HCUP) databases are limited data sets. HCUP databases conform to the definition of a limited data set. A limited data set is health care data in which 16 direct identifiers, specified in the privacy rule, have been removed. Under HIPAA, review by an institutional review board (IRB) is not required for use of limited data sets. Please see this weblink: ![]() . The authors ensure accuracy and integrity of their work.
. The authors ensure accuracy and integrity of their work.
Informed consent
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.