
Abstract
Human hookworm infection is caused by the nematodes Necator americanus, Ancylostoma duodenale, and Ancylostoma ceylanicum. Iron deficiency anemia is the hallmark of chronic, moderate-to-heavy-intensity infections, promoting a vicious poverty cycle. Overt severe and acute life-threatening lower gastrointestinal hemorrhage is an extremely rare manifestation of hookworm infection, as well as finding multiple nematodes attached to the colonic mucosae. This rare hookworm presentation with hematochezia from the colon in a patient living with human immunodeficiency virus highlights the importance of physicians’ awareness of this neglected tropical disease responsible for high morbidity and burden in healthcare systems of endemic regions.
Introduction
The nematodes Necator americanus, Ancylostoma duodenale, and Ancylostoma ceylanicum are the etiologic agents of human hookworm infection.1,2 Elimination of hookworm infections has been achieved in most of the industrialized world due to improved sanitation and standards of living because of economic growth and urbanization. Nonetheless, hookworm infection continues to represent a significant burden in rural areas of tropical and subtropical regions of low and middle-income countries where poverty, poor sanitary infrastructure, and suitable soil and climate conditions coexist. Well-intended interventions such as mass drug administration (MDA) and the Water, Sanitation, and Hygiene (WASH) programs have failed to achieve the desired long-term impact on the intensity and prevalence of soil-transmitted helminthiasis (STH). Hookworm infection is considered one of the most important STH, accounting for close to 113 million cases and 540.20 thousand million lost disability-adjusted life years (DALYs) annually. 3
Iron deficiency anemia is the hallmark of chronic, moderate-to-heavy intensity infections, promoting a vicious poverty cycle due to higher rates of low birth weight in affected communities coupled with impaired cognitive and physical development of their children and decreased productivity of their adults. 1 In the Peruvian Amazon, the situation is especially critical. A study conducted in Iquitos showed that 47.2% of pregnant women were infected with hookworms, and only 9.31% were free of any STH. 4 A high prevalence of hookworm infection shortly after MDA has also been reported in this region. 5
Overt severe and acute gastrointestinal hemorrhage is an extremely rare manifestation of hookworm infection, as well as finding multiple nematodes in the colon. We followed the CARE case report guidelines 6 to describe these two rare presentations in a patient from a highly endemic area that required inpatient management causing high morbidity and a burden on the healthcare system.
Case
A 34-year-old male from Iquitos City, Department of Loreto in the Peruvian Amazon, presented with a 1-month history of excoriated pruritic lesions in the abdominal wall region that appeared after contact with sewage. Approximately 1 week after the appearance of the skin lesions, the patient developed a nonproductive cough of nocturnal predominance that lasted 8 days. Approximately 8 days before admission, he developed profuse diarrhea followed by hematochezia, for which he sought care at the Regional Hospital of Loreto, a major tertiary hospital.
His past medical history included human immunodeficiency virus (HIV) infection diagnosed 15 years ago (CD4 741 cells/mm3; undetectable viral load) on tenofovir disoproxil fumarate, lamivudine, and efavirenz. On physical examination, blood pressure was 100/60 mmHg, heart rate was 90 beats/min, respiratory rate was 24 breaths/min, and blood oxygen saturation was 96% on room air. The skin was pale with a yellowish hue. Hyperchromatic lesions were seen on the abdominal wall (Figure 1). The rest of the physical examination was unremarkable. Laboratory findings were significant for a white blood cell count of 15,810 cells/mm3 with 37% eosinophils (absolute: 5847 eosinophils/µL), a hemoglobin of 5.1 mg/dL with a mean corpuscular volume (MCV) of 73 fL, and a normal platelet count and coagulation parameters.

Hyperchromic lesions of linear shape, abdominal region.
The patient was treated with intravenous fluids and a transfusion of two units of packed red blood cells. Due to the persistent hematochezia, the patient underwent a lower endoscopy that showed a friable mucosa with diffuse ulcerations as well as numerous nematodes adhered to the rectal mucosa, sigmoid, and the descending and transverse colon (Figure 2(a) and (b)).
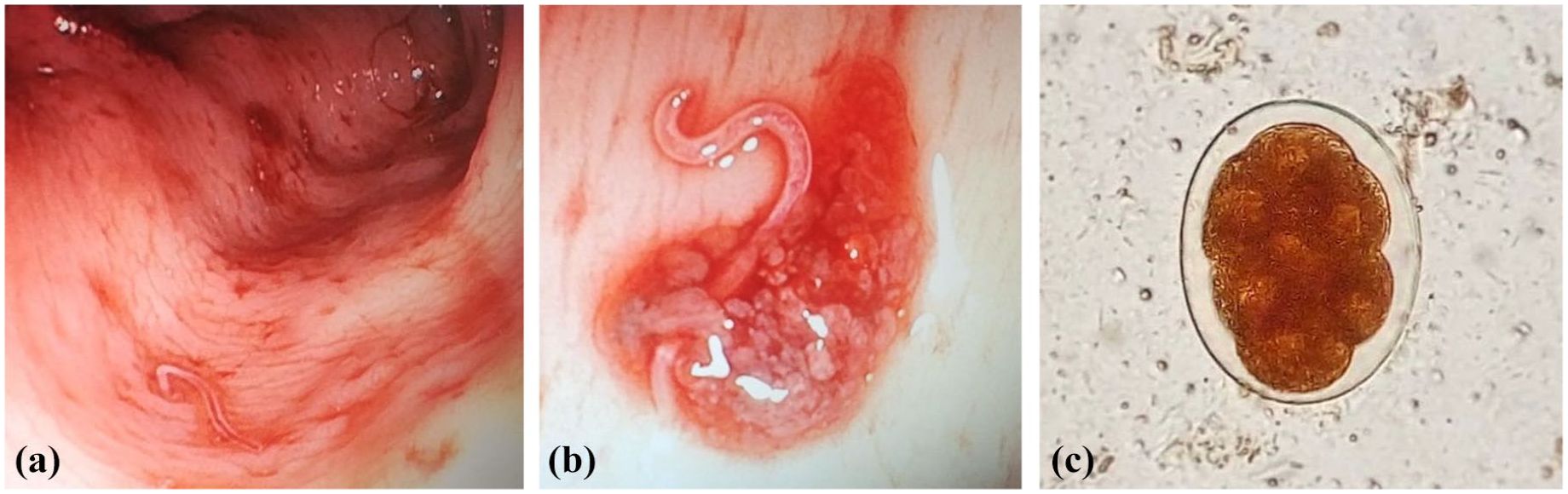
Lower endoscopy: (a) Transverse colon mucosa, with ulcerations and parasites anchored to the mucosa. (b) Note the parasite anchored to the colonic mucosa with perilesional reaction. (c) Hookworm egg recovered from the patient.
The diagnosis of severe hookworm infection was confirmed by detecting only hookworm eggs in the stool sample at a moderate intensity (Figure 2(c)). Unfortunately, we were unable to retrieve nematodes during the colonoscopy for species identification. The patient was treated with albendazole 400 mg orally daily for 3 days. After several days of hospitalization, the patient was discharged after demonstrating favorable clinical and laboratory improvement.
Discussion
Hookworm infection is a leading cause of iron deficiency anemia in low and middle-income countries. The degree of anemia is determined by factors such as iron intake and stores, the intensity and duration of infection, and the infecting species. 4 A. duodenale, for example, leads to a more significant amount of blood loss (>10 times) compared to N. americanus. 1 The WHO classifies hookworm infections as light (⩽1999 eggs per gram of stool), moderate (2000–3999 eggs per gram of stool), and heavy (⩾4000 eggs per gram of stool), with the severity of the anemia being directly proportional to the intensity of the infection. 7 Nevertheless, the egg count does not always accurately reflect the burden of the infection; this is especially true when only one stool sample is collected or when examination does not occur within 1 h of collection. 8
Blood loss is primarily due to leakage around the attachment site, as opposed to direct feeding by the adult worms. 1 Hookworms secrete nematode anticoagulant peptides (NAPs), inhibiting coagulation factors such as Xa, XIa, and VIIa/tissue factor complex. 9 The enhancement of the anticoagulant effect of these peptides might be responsible for the rare reports of potentially life-threatening hematochezia in patients taking systemic anticoagulants.10 –14 Hookworm infestation of the colon is an infrequent finding, first reported in India in 2006. 15 The occasional migration and maturation of larvae in ectopic locations (i.e., outside the small intestine) is not well understood. In our case, the severity of the gastrointestinal hemorrhage and the finding of adult hookworms in the colon is an extremely rare event (Table 1).
Reports of hookworms in the colon excluding Ancylostoma caninum and Ancylostoma ceylanicum.

A recent meta-analysis showed that patients living with HIV had higher odds of becoming infected with Strongyloides stercoralis but a lower chance of developing hookworm infection. 25 Furthermore, studies have shown that STH impairs the TH1 immune response, which is central in controlling viral replication; however, studies examining the effect of deworming on the natural history of HIV infection have been inconclusive. 26 Our patient had been virologically suppressed with a normal CD4 cell count for many years, making it unlikely for HIV to be responsible for the nature and severity of the hookworm infection.
An unusually severe acute infection due to a high larval load could not be excluded. The patient’s skin findings were suggestive of dermal itch, a reliable and universal sign indicative of larval skin penetration that can persist for 1–4 weeks. 27 His skin lesion is atypical because the pruritic erythematous rash of human hookworm infection does not commonly have the linear or serpiginous erythematous track characteristically seen with cutaneous larva migrans caused by animal hookworms.28,29
The time course of his symptomatology mirrors the life cycle of the helminth, further supported by the degree of eosinophilia, which typically peaks at the onset of gastrointestinal symptoms continuing until egg patency—about 6–12 weeks after infection.1,27 The respiratory complaints in hookworm infection correlate with the migration of the larvae through the respiratory tract (i.e., Löffler syndrome). 29 Nevertheless, experimental human hookworm infections have called into question the association between hookworm larval migration in the respiratory tract and Löffler syndrome.27,30
In conclusion, hookworm infection continues to be a major cause of morbidity and mortality, predominantly affecting neglected communities. Atypical presentations of hookworm infections should be considered in highly endemic areas. Although great advancements have been made in understanding the intricacies of the disease, its diagnosis, and treatment, eradicating hookworm infection is unlikely to be achieved without thoughtful and sustainable investments to improve the sanitary conditions of the affected communities.