
Abstract
Introduction:
Chagas disease (CD) is caused by Trypanosoma cruzi. When acquired, the disease develops in stages. For diagnosis, laboratory confirmation is required, and an extensive assessment of the patient’s health should be performed. Treatment consists of the administration of trypanocidal drugs, which may cause severe adverse effects. The objective of our systematic review was to analyze data contained in the CD published case reports to understand the challenges that patients and clinicians face worldwide.
Materials and methods:
We performed a systematic review following the PRISMA guidance. PubMed database was explored using the terms ‘American trypanosomiasis’ or ‘Chagas disease’. Results were limited to human case reports written in English or Spanish. A total of 258 reports (322 patients) were included in the analysis. Metadata was obtained from each article. Following this, it was analyzed to obtain descriptive measures.
Results:
From the sample, 56.2% were males and 43.8% were females. Most cases were from endemic countries (85.4%). The most common clinical manifestations were fever during the acute stage (70.0%), dyspnea during the chronic stage in its cardiac form (53.7%), and constipation during the chronic stage in its digestive form (73.7%). Most patients were diagnosed in the chronic stage (72.0%). Treatment was administered in 56.2% of cases. The mortality rate for the acute stage cases was 24.4%, while for the chronic stage this was 28.4%.
Discussion:
CD is a parasitic disease endemic to Latin America, with increasing importance due to human and vector migration. In this review, we report reasons for delays in diagnosis and treatment, and trends in medical practices. Community awareness must be increased to improve CD’s diagnoses; health professionals should be appropriately trained to detect and treat infected individuals. Furthermore, public health policies are needed to increase the availability of screening and diagnostic tools, trypanocidal drugs, and, eventually, vaccines.
Introduction
American trypanosomiasis, or Chagas disease (CD), is a parasitic disease caused by infection with the hemoflagellate protozoan Trypanosoma cruzi (T cruzi). 1 It is recognized by the World Health Organization (WHO) as a Neglected Tropical Disease (NTD). 2 NTDs are a group of infectious and non-infectious diseases that are prevalent in tropical and subtropical environments. They mainly affect poor and marginalized communities with low visibility and little political voice. 3 While endemic to Latin America, CD can now be found in immigrant populations worldwide. CD can be transmitted to humans by several different pathways; it poses a challenge to health professionals and health systems that are unprepared to diagnose and treat the disease. The objective of our systematic review was to analyze the data contained in the CD published case reports to understand the challenges that CD patients experience and the practices of CD clinicians worldwide.
Materials and methods
Search strategies
A systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidance. 4 The PubMed database was explored using the search terms ‘American trypanosomiasis’ or ‘Chagas disease.’ The results were filtered to include full-text case reports of humans with CD, written in English or Spanish. A total of 456 records were obtained during the initial search. Two reviewers screened the titles and abstracts to determine if they met the inclusion criteria. During the screening, 35 records were excluded: 19 that could not be accessed or tracked, 14 that were not a case report, and 2 that were duplicated. A total of 421 records proceeded to the full-text assessment. Four reviewers assessed the content of the case reports to determine if they had enough information about the patients and their disease. During the assessment, 163 records were excluded: 74 that did not contain enough information of the patients, 65 that did not mention CD at all (Chagas was the surname of an author, or part of the name of its workplace), 22 that mentioned CD as a possible diagnosis, and 2 that only mentioned CD as a comorbidity. A total of 258 records describing the information of 322 patients were included in the analysis (Table 1). For quality assurance, another pair of reviewers randomly selected 10% of the case reports and assessed their consistency. No other records were excluded. The complete selection process can be consulted in Figure 1.
Number of patients contained in each Chagas Disease case report.


PRISMA flow diagram of the systematic review.
Data extraction
Each case report was read and predefined variables were extracted, including:
A spreadsheet was built using Excel® from Microsoft Office 360® for data synthesis.
Statistical analysis
The Excel® from Microsoft Office 360® spreadsheet was exported to SPSS Statistics® software version 26 from IBM Corporation® to obtain descriptive measures of frequency, tendency, and dispersion, according to the characteristics of each variable.
Results
Demographic data
Of the 322 cases, 181 (56.2%) were males and 141 (43.8%) were females. The mean age of presentation was 37.7 years [+/− standard deviation (SD) 19.6].
Geographic data
A total of 275 (85.4%) cases were reported in endemic countries, while 47 (14.6%) were reported in non-endemic countries. From the endemic countries, Brazil had the most with 104 (32.3%) cases, followed by Argentina with 48 (14.9%), and Bolivia with 26 (8.1%). Of the non-endemic countries, the United States (US) had the most with 29 (9.0%) cases, followed by Spain with 8 (2.5%), and Canada with 4 (1.2%). The global distribution can be found in Figure 2.

Country of origin of the patients included in the CD case reports.
Mechanism of transmission
The mechanism of transmission was known in 125 (38.8%) cases and unknown in 197 (61.2%). From the cases in which the mechanism of transmission was acknowledged, oral transmission was the most common route, with 31 (24.8%), followed by organ transplantation and vector-borne transmission with 29 (23.2%), congenital transmission with 23 (18.4%), blood transfusion with 9 (7.2%), and accidental exposure with 4 (3.2%).
Additional information regarding the mechanism of transmission was obtained for:
Clinical manifestations
The most common clinical manifestations by stage and substage of the disease were:
The complete list of clinical manifestations, sorted into clusters and presented according to each stage and substage of the disease, can be consulted in Table 2.
Frequency of clinical manifestations described in the Chagas Disease case reports.
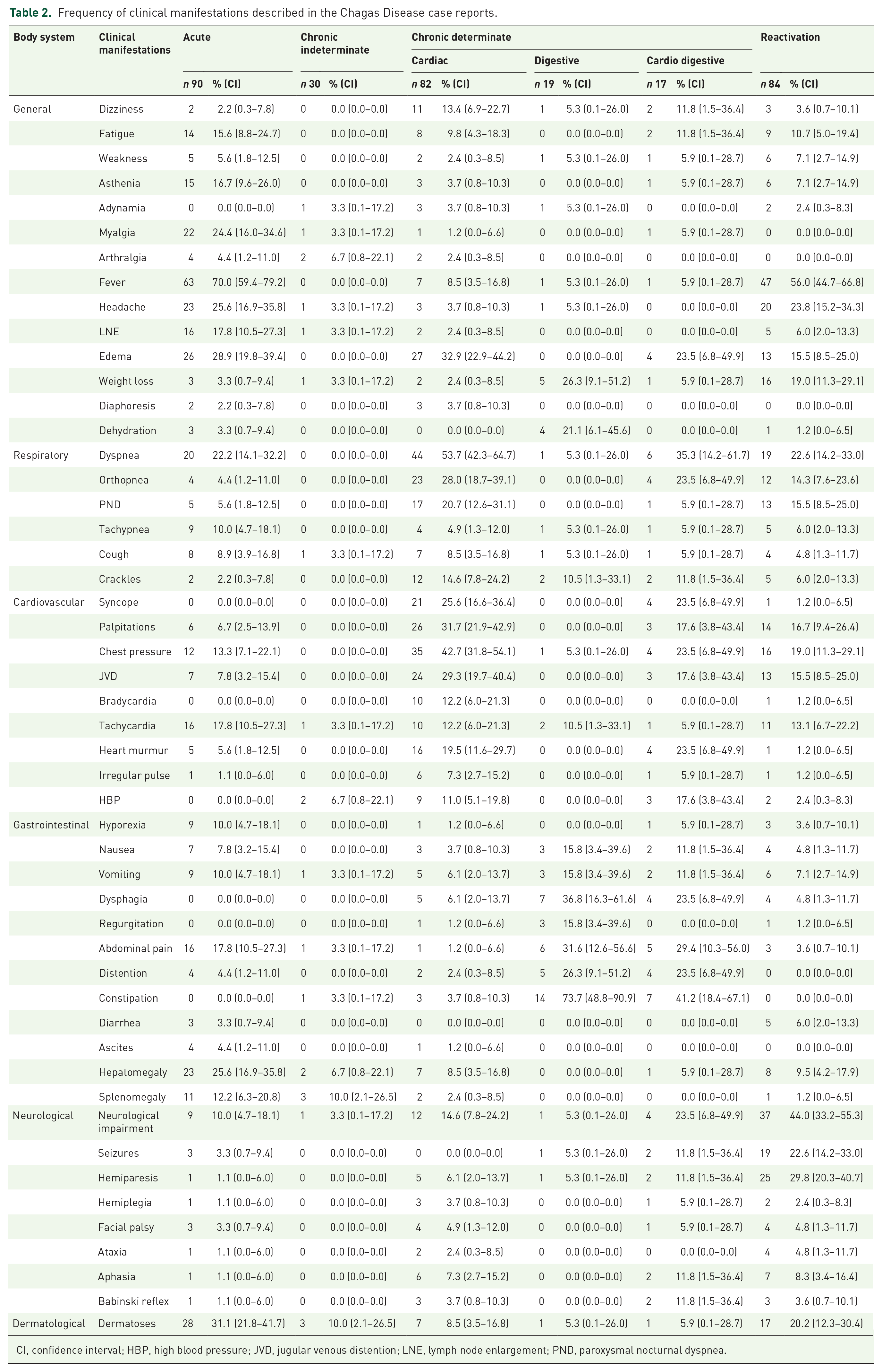
CI, confidence interval; HBP, high blood pressure; JVD, jugular venous distention; LNE, lymph node enlargement; PND, paroxysmal nocturnal dyspnea.
Laboratory tests
Diagnostic acute stage tests were performed in 187 (58.1%) cases, while diagnostic chronic stage tests were performed in 261 (81.1%).
The dataset was filtered to identify the most ordered diagnostic tests in each stage:

Results of the acute stage tests described in the CD case reports.

Results of the chronic stage tests described in the CD case reports.
Imaging studies
The most common imaging studies by stage and substage of the disease were:
The list of abnormal findings described in chest X-rays (Table S1), ECGs (Table S2), echocardiograms (Table S3), abdominal X-rays (Table S4), barium swallows (Table S5), barium enemas (Table S6), abdominal ultrasounds (Table S7), abdominal CTs (Table S8), endoscopies (Table S9), colonoscopies (Table S10), and head CTs (Table S11) by stage and substage of the disease can be consulted in the supplementary material.
Stages of the disease
Of the 322 cases, 90 (28.0%) were diagnosed during the acute stage of the disease while 232 (72.0%) were diagnosed during the chronic stage. Of the chronic stage cases, 30 (9.3%) had the chronic indeterminate stage, 118 (36.6%) the chronic determinate stage, and 84 (26.1%) had a reactivation of the disease. From the cases that had the chronic determinate stage, 82 (25.5%) developed the cardiac form, 19 (5.9%) the digestive form, and 17 (5.3%) the cardiodigestive form.
Management of the disease
Trypanocidal drug treatment was administered in 182 (56.2%) cases, and it was deferred, not offered, or rejected in 140 (43.8%). From the cases who received a trypanocidal drug, 140 (76.9%) received benznidazole, 41 (22.5%) received nifurtimox, and in 1 (0.6%) case, the trypanocidal drug was not specified. Trypanocidal drug treatment was started during the acute stage of the disease in 71 (39.0%) cases and during the chronic stage in 111 (60.9%). Surgery was performed in 70 (21.7%) cases to treat complications of the disease.
Histopathologic studies
Histopathology was performed in 126 (39.1%) cases and not performed in 196 (60.9%). When performed, the presence of amastigotes was detected in 81 (64.3%) of the cases and it was undetected in 45 (35.7%). When detected, 73 (90.1%) cases had the presence of amastigotes in one organ, 5 (6.2%) in two organs, and 3 (3.7%) in three organs. In total, amastigotes were identified in 92 (73.0%) different histopathologic specimens, from which 29 (31.5%) were from the heart, 26 (28.3%) from the brain, 16 (17.4%) from the skin, 6 (7.5%) from the esophagus, 4 (4.3%) from the colon and placenta, 2 (2.2%) from the larynx, and 1 (1.1%) from the bone marrow, eyes, stomach, kidneys, and cervix.
Outcome
From the 322 cases, 88 (27.3%) [confidence interval (CI) 95% (22.5–32.5)] patients died. Of them, 22 (25.0%) (16.4–35.4) were in the acute stage of the disease, and 66 (75.0%) (64.6–83.6) in the chronic stage. The mortality rate was 24.4% (16.0–34.6) for the acute stage cases, and 28.4% (22.7–34.7) for the chronic stage cases. From the cases that were at the chronic stage, 2 (3.0%) (0.4–10.5) had the chronic indeterminate stage, 21 (31.8%) (20.9–44.4) the chronic determinate stage, and 43 (65.2%) (52.4–76.5) had a reactivation of the disease. The mortality rate was 6.7% (0.8–22.1) for the chronic indeterminate cases, 27.1% (19.3–36.1) for the chronic determinate cases, and 51.2% (40.0–62.3) for the cases that had a reactivation of the disease. Of those who were in the chronic determinate stage, 16 (76.2%) (52.8–91.8) had the cardiac form, 1 (4.8%) (0.1–23.8) the digestive form, and 4 (19.0%) (5.4–41.9) had the cardio digestive form. The mortality rate was 19.5% (11.6–29.7) for the cardiac form, 5.3% (0.1–26.0) for the digestive form, and 23.5% (6.8–49.9) for the cardio digestive form.
The most common causes of death by stage and substage of the disease can be found in Table 3.
Causes of death as described in the Chagas Disease case reports.

CI, confidence interval.
Discussion
Epidemiology
The WHO has estimated that between 6 and 8 million people live with CD and that there are between 65 and 100 million people at risk of acquiring the disease. 5 Each year, approximately 30,000 new cases and nearly 12,000 deaths are reported in the Americas. 6 The Global Burden of Disease Study 2019 estimated that it is responsible for 275,000 disability-adjusted life years due to its substantial morbidity and premature mortality. 7 CD is endemic to 21 Latin American countries. 8 However, globalization has led to subsequent migration of infected individuals and vectors to non-endemic countries. 9 According to our review, most of the individuals who acquired the disease came from endemic countries. Despite this, several of them were diagnosed in non-endemic countries. This situation highlights the problem of patients traveling around the globe without knowing their health status. Interestingly, the autochthonous transmission has been reported in non-endemic countries, including the US, which now has native triatomines throughout the southern states. 1 CD is becoming a worldwide health problem.
Mechanism of transmission
CD is caused by a parasite named T. cruzi, an obligate, intracellular protozoan with high genetic and phenotypic diversity. CD is primarily a vector-borne disease, but it can also be transmitted through blood transfusions, bone marrow, or organ transplants, from an infected pregnant mother to her child, by ingestion of contaminated food or drinks, and by accidental exposure. 10 In our review, we found that 6 out of 10 patients did not know how they acquired the disease. This is common, because triatomines take blood meals at night undetected. We also read some cases in which people reported having triatomes as pets. A lack of awareness, poor hygienic habits, cohabitation with animals, and poor house dwelling quality are considered the main risk factors for acquiring the disease. 11
Regarding other less common routes of transmission, such as blood transfusions and bone marrow or organ transplants, many non-endemic countries have recently added screening of the disease to their health protocols, 12 including identifying antibodies against T. cruzi. However, there are several countries in which pregnant women are not universally screened for CD. 13 In one case report, there were three generations of women diagnosed with CD; congenital transmission was suspected between them. 14 Screening of the disease during pregnancy must become a public health policy to prevent further transmission.
Other routes of transmission that cannot be prevented through screening are oral transmission and accidental exposure. Oral transmission has been acknowledged as an important route for acquiring CD, leading to a highly severe, acute presentation and can happen in contaminated food outbreaks. The foods that have been associated with this route are vegetables and wild animal meat; meanwhile, the beverages include açai, babaçu, bacaba, ‘comou’, guava, and orange juice, sugar cane, and palm wine. 15 We identified that açai and bacaba juice were the beverages responsible for half of the cases. However, we could not determine which food or beverage were involved in the other half. People should understand the importance of consuming provisions that have passed through washing and pasteurizing processes, as they almost nullify the possibility of acquiring the disease.
Accidental exposure may occur in a laboratory when an unplanned event compromises the handling of specimens that carry viable organisms. 16 In theory, people who handle them use personal protective equipment to prevent it and know how to react to exposure. In some cases, the handlers underestimated the accidental exposure or did not report the event to the Department of Occupational Health until clinical manifestations appeared.
Clinical manifestations
Clinically, CD can be divided into stages. After the incubation period, which ranges between 7 and 14 days, the host enters the acute stage of the disease, which lasts between 2 and 4 months. At this stage, CD remain asymptomatic in 95% of cases or may present unspecific manifestations in the other 5% of the cases. Among these symptoms are fever, asthenia, adynamia, myalgia, arthralgia, headache, and hepatomegaly or splenomegaly. The Romaña sign and chagomas, which are the hallmarks of the disease, are present in the minority of the cases. Less common symptoms are seizures, altered mental status, and neurological impairment that can be experienced due to CD encephalitis, and dyspnea, chest pressure, and palpitations that can be experienced due to CD myocarditis. 17 In our review, we found that 7 out of 10 patients developed fever, that 3 out of 10 had dermatoses, and that 2 out of 10 experienced myalgia, headache, dyspnea, or hepatomegaly. Other clinical manifestations were less commonly observed; by seeing the clinical picture, we can understand why this stage usually goes unnoticed.
Following this stage of disease, the hosts enter the chronic stage of the disease, and depending upon their immunological response; they can remain in the indeterminate stage (70–90%) or may develop the determinate stage (10–30%), in which cardiac, digestive, or cardiodigestive complications are present. CD cardiomyopathy can be characterized by the presence of arrhythmias, conduction system abnormalities, segmental and general contractility abnormalities, progressive congestive heart failure, thromboembolic phenomena, and sudden death; meanwhile, CD megaesophagus can be characterized by the presence of progressive dysphagia that leads to achalasia and increases the risk of regurgitation and bronchoaspiration, and CD megacolon can be characterized by the presence of progressive constipation that increases the risk of fecaloma, volvulus, and bowel ischemia. 18 In addition, if the host develops immunosuppression, this can result in reactivation of the disease, in which clinical manifestations related to meningoencephalitis, encephalitis, myocarditis, and panniculitis can appear. 19 In our study, we found that only 1 out of 10 patients experienced non-specific symptomatology during the indeterminate stage, which keep them away from seeking medical attention. In contrast, we identified that 5 out of 10 patients developed dyspnea and that 4 out of 10 experienced chest pressure at the chronic determinate stage in its cardiac form; that 7 out of 10 had constipation, and that 3 out of 10 reported having dysphagia and abdominal pain at the chronic determinate stage in its digestive form; and that 4 out of 10 developed constipation and that 3 out of 10 experienced dyspnea at the chronic determinate stage in its cardio digestive form. In addition, we identified that 5 out of 10 patients had fever and that 4 out of 10 reported neurological impairment when they had a reactivation of the disease. At this stage, it is possible to identify the body system that has been affected. CD should be considered part of the differential diagnosis in any individual who lives in, or has traveled to, endemic countries and has developed the cardiac, digestive, or cardiodigestive disease, and in any case of encephalitis, myocarditis, or panniculitis in patients with immunosuppression.
Laboratory testing
Epidemiological background and clinical manifestations should be considered to make the diagnosis; however, laboratory confirmation is required, and it can be done by multiple methods. Acute CD can be confirmed through direct observation of the parasite in the circulating blood. Simple methods such as fresh blood and blood smear or concentration methods such as Strout test or microhematocrit serve this purpose. Indirect observation can be done by blood culture or xenodiagnoses. In addition, since they need special laboratory requirements and it takes plenty of time to obtain their results, they have fallen into disuse. PCR is an alternative method that has proved its value to diagnose the disease at this stage, especially in congenital cases. 20 In our review, the most frequently performed test for this stage was PCR; coincidently with what has been published in the literature, it was the test that had the highest positive results when performed. However, PCR is not widely available, especially in low-resource settings. In those case scenarios, direct blood examination, blood smear, Strout test, and microhematocrit must remain as the gold standard for diagnosis because they can be easily performed with trained personnel and basic laboratory equipment. Blood culture and xenodiagnoses shall remain only as complementary methods.
On the other hand, chronic CD can be confirmed by detecting antibodies of T. cruzi in the blood. This can be conducted using ELISA, IIF, or HAI. Each of these methods has high sensitivity and sensibility. According to the WHO and the Pan American Health Organization (PAHO), two positive results with two different serologic methods are needed to confirm a diagnosis of CD. Other methods, such as CMIA, CFT, ICT, RIPA, and IB, are useful, but have limited clinical utility, are mainly used for research, or are not commercially available. 21 In our review, the most frequently performed tests for this stage were IIF, ELISA, and HAI, as expected according to the current guidelines. Regarding the other serologic tests, IB was mainly performed in research facilities, and CMIA, CFT, ICT, and RIPA were primarily used in older cases. All the tests that were performed at this stage yielded positive results when performed. However, no test should be taken into consideration by itself.
Imaging testing
Once the diagnosis is confirmed, patients must be entirely assessed by a transdisciplinary team to identify if there are any disease-related complications. At least an ECG must be performed on every patient to rule out cardiac involvement. If an abnormality is detected at the ECG, echocardiography, chest X-rays, 24-h Holter monitoring, exercise stress testing, electrophysiologic studies, nuclear medicine testing, cardiac magnetic resonance imaging (MRI), or cardiac catheterization and coronary angiography may be practiced according to the underlying symptomatology. 22 We found that an ECG was ordered in 4 out of 10 patients during the acute stage of the disease. The complimentary cardiovascular assessment was performed in 4 out of 10 patients with an echocardiogram and in 2 out of 10 patients with a chest X-ray. The main abnormalities found were changes in repolarization, pericardial effusion, and cardiac enlargement, respectively. On the other hand, regardless of the chronic form of the disease, we observed that an ECG was ordered in 6 out of 10 patients during the chronic stage. The complimentary cardiovascular assessment was performed in 5 out of 10 patients with an echocardiogram and in 3 out of 10 with a chest X-ray. The main abnormalities found were right bundle branch block, decreased left ventricular ejection fraction, and cardiac enlargement, respectively. These types of studies were underutilized, but the findings were consistent with what has been described in the literature.
When CD is suspected, barium swallow, manometry, and endoscopy may be performed to rule out esophageal involvement; meanwhile, barium enema or colonoscopy may be practiced to rule out colonic involvement. 23 Other imaging studies such as abdominal X-rays, abdominal CT, and abdominal ultrasound may be requested upon specific conditions. Each study should be justified and must be performed following the current best practices. In our review, we identified that imaging studies to rule out gastrointestinal involvement were performed in about 1 out of 10 patients during the acute and chronic stages of the disease, which is comprehensive. The main abnormalities found in the esophageal studies were megaesophagus and cardiac narrowing; meanwhile, the most frequently reported abnormalities at the colonic studies were megacolon, megasigma, and megarectum, also consistent with what has been published in the literature.
Furthermore, if central nervous system (CNS) involvement is suspected, a head CT or MRI may be performed. 24 In our study, we found that a head CT was performed in almost 1 out of 10 patients during the acute stage of the disease and in 2 out of 10 during the chronic stage. This is perfectly understandable, because CNS is not as frequently involved as the cardiovascular or gastrointestinal systems, unless immunosuppression occurs. The main finding in this kind of study was the presence of an intracranial mass, which can be related to the formation of abscesses containing trypanosomes.
Treatment
The approach to the management and treatment of CD depends upon the patient’s stage of the disease. Trypanocidal drugs, like benznidazole and nifurtimox, are indicated for those who are at the acute stage, or who are at the chronic stage but are asymptomatic and do not have organ damage. They are contraindicated during pregnancy and in patients with hepatic or kidney failure. Nifurtimox is also contraindicated in case of neurological or psychiatric disorders.2,25 Their cure rate ranges from 70% to 80% when administered during the acute stage of the disease; meanwhile, it ranges from 6% to 10% when administered during the chronic stage. 25 In our review, about 3 out of 10 patients were at the acute stage of the disease, and 7 out of 10 at the chronic stage. From the patients at the chronic stage of the disease, 1 out of 10 remained in the chronic indeterminate stage, and 5 out of 10 developed the chronic determinate stage. The other 4 out of 10 had a reactivation of the disease due to immunosuppression. Even though the chronic stage is traditionally divided into chronic indeterminate and chronic determinate stages, we decided to maintain the ‘reactivation’ tag by what the authors reported. By this means, these cases can easily be identified. Regarding treatment, 5 out of 10 patients received trypanocidal treatment. It is well known that benznidazole is better tolerated than nifurtimox, and from the patients who received specific drug treatment, benznidazole was preferred over nifurtimox. Most of the cases in which patients did not receive trypanocidal treatment are justified because of the disease’s stage at where they were and the underlying complications that they had. However, we read about many cases in which patients were eligible. In these cases, clinicians did not consider that they should have been administered, clinicians wanted to administer them, but drugs were not currently available, or patients chose not to take them due to the possible side effects. When started, almost 4 out of 10 patients were at the acute stage of the disease and 6 out of 10 at the chronic stage. This highlights an area of opportunity, as the effectiveness of these treatments decreases over time.
The treatment of CD cardiomyopathy consists of the administration of a combination of angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, anticoagulants, antiarrhythmics, β-blockers, digoxin, and diuretics. Pacemakers and implantable cardiac defibrillators may be needed to treat the presence of arrhythmias and conduction system abnormalities, as well as cardiac bridging and heart transplantation for end-stage heart failure. 22 The treatment of CD megaesophagus consists of the administration of sphincter relaxants (isosorbide dinitrate or nifedipine), pneumatic balloon dilatation, botulinum toxic injections, and surgery if needed. On the other hand, the treatment of CD megacolon consists of the administration of laxatives, colon enemas, and surgery, if required. 26 In our review, we found that two-thirds of the surgeries that were performed were related to cardiovascular complications (from pacemaker implantation to heart transplantation). The other third of the performed surgeries were related to gastrointestinal complications (from esophagectomy to colectomy). In some cases, surgery is the only option available to improve the symptoms of the patients. However, no patient with CD should develop end-stage chronic complications if it is promptly approached.
Outcome
CD mortality rate has been estimated between 1.5% and 51%. According to Cucunubá et al., 27 this heterogeneity in the estimates comes from the lack of agreement between the methodologies that have been used to calculate them. In our review, we found out that the mortality rate for the acute stage cases was 24.4%, while for chronic stage cases this was 28.4%. When disaggregated the chronic stage cases, the mortality rate was 6.7% for the chronic indeterminate cases, 27.1% for the chronic determinate cases, and 51.1% for the cases that had a reactivation of the disease. When disaggregated the chronic determinate stage cases, the mortality rate was 19.5% for the cardiac form, 5.3% for the digestive form, and 23.5% for the cardio digestive form. This excess in mortality can be explained because of the nature of the case reports. Controlled patients are not usually published in the literature; meanwhile, patients with complications, and consequently, worse prognoses, are frequently reported. Moreover, we can relate to several deaths during each stage with the congenital transmission, oral transmission, or reactivation of the disease, respectively.
Limitations
Our study was performed by assessing the data contained in case reports. These kinds of publications describe the clinical picture of rare diseases or uncommon presentations of common diseases. In the case of CD, those who belong to non-endemic countries are related to their sole presence; meanwhile, those who belong to endemic countries are related to uncommon mechanisms of transmission that lead to uncommon clinical pictures, immunosuppression that leads to reactivation, or advanced disease stages that lead to unfortunate outcomes. These situations should be taken into consideration to understand the overrepresentation of some uncharacteristic features.
Conclusion
CD is a parasitic disease endemic to Latin America, with significant relevance in the world due to increasing migration. In our review, besides describing the trends in the medical practice, which have been appointed in each section of the discussion, we observed a couple of problems that are present in most of the cases: people are unaware of the threat that this disease represents for their health and patients travel a long journey from the onset of their symptoms until they are finally diagnosed. Community awareness must be increased to prevent the disease’s acquisition, and health professionals should be trained early in their career to promptly detect and properly treat the current cases. We cannot longer keep missing opportunities to stop the progression of the disease. Furthermore, public health policies must be modified to guarantee the availability of screening and diagnostic tests, the stock of trypanocidal drugs, and, eventually, preventive and therapeutic vaccines. CD must be acknowledged as a serious health problem, and major stakeholders must intervene to ensure that no patient is left behind.
Supplemental Material
sj-pdf-1-tai-10.1177_20499361211033715 – Supplemental material for A systematic review of historical and current trends in Chagas disease
Supplemental material, sj-pdf-1-tai-10.1177_20499361211033715 for A systematic review of historical and current trends in Chagas disease by Diego-Abelardo Álvarez-Hernández, Rodolfo García-Rodríguez-Arana, Alejandro Ortiz-Hernández, Mariana Álvarez-Sánchez, Meng Wu, Rojelio Mejia, Luis-Alberto Martínez-Juárez, Alejandra Montoya, Héctor Gallardo-Rincon, Rosalino Vázquez-López and Ana-María Fernández-Presas in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
We thank María-José Díaz-Huízar MD, Alberto-Manuel González-Chávez MD, Mario-Alberto González-Chávez MD, Jorge-Alberto Ascencio-Aragón MD, Yolanda Hernández-Ponce MD, and Emmanuel Estefan-Melgarejo PhD for their participation and support in a previous stage of the study.
Author contributions
Conceived and designed the study: DAAH, RGRA; evaluated the studies and extracted the data: DAAH, RGRA, AHO, MAS, LAMJ, RVL; performed the analyses: DAAH, RGRA, AHO, MAS, LAMJ, AM, HGR, RVL; wrote the paper: DAAH, RGRA, AHO, MAS, LAMJ, MW, RM, AM, HGR, RVL, AMFP. All authors revised and approved the final version of the paper.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.