
Abstract
Asylum-seekers and refugees have an increased burden of infections compared with the general population. This has been widely recognised by countries welcoming those fleeing conflict and persecution; however, there are no screening standardised guidelines and regulatory processes. Identification of certain neglected tropical diseases (NTDs) and other infections is important for the health and well-being of the individual in addition to public health and biosecurity. In the United Kingdom, screening for infections at port of entry or after arrival is not mandatory. Those on refugee resettlement programmes will have infection screening as part of their pre-entry health assessment, but no such system exists for those claiming asylum in the United Kingdom. In this article, we have reviewed published, peer-reviewed articles looking at the approaches to screening for NTDs and infectious diseases in the United Kingdom. In addition to this, we have reviewed the literature looking at the acceptability, barriers and facilitators of these screening practices. We found that there is a heterogeneous approach to screening practices in the United Kingdom and a paucity of data to support a single ‘best practice’ approach. Based on our findings, we have made recommendations and consideration for NTD screening strategies and highlighted important areas for future research.
Introduction
Background
Migration is inextricably connected to human history. Some people leave their homes to seek employment, travel and meaningful lives in another country. Others are forced to do so because they face persecution, conflict or natural disaster if they stay. As global migration has increased, 1 so too has forced migration due to the exacerbation of several crises in the last 10 years. 2 The number of people seeking asylum or entering the United Kingdom as refugees has increased steadily over the last decade. 3 In 2021, the number of people applying for asylum in the United Kingdom reached 48,540, the highest number for almost two decades. 4
Migrants, and especially forced migrants (definitions in Table 1), might be at higher risk of infectious diseases for many reasons. They have an increased risk of exposure to many pathogens due to higher prevalence in their country of origin, poor living conditions during the journey and in destination countries.
Definitions.
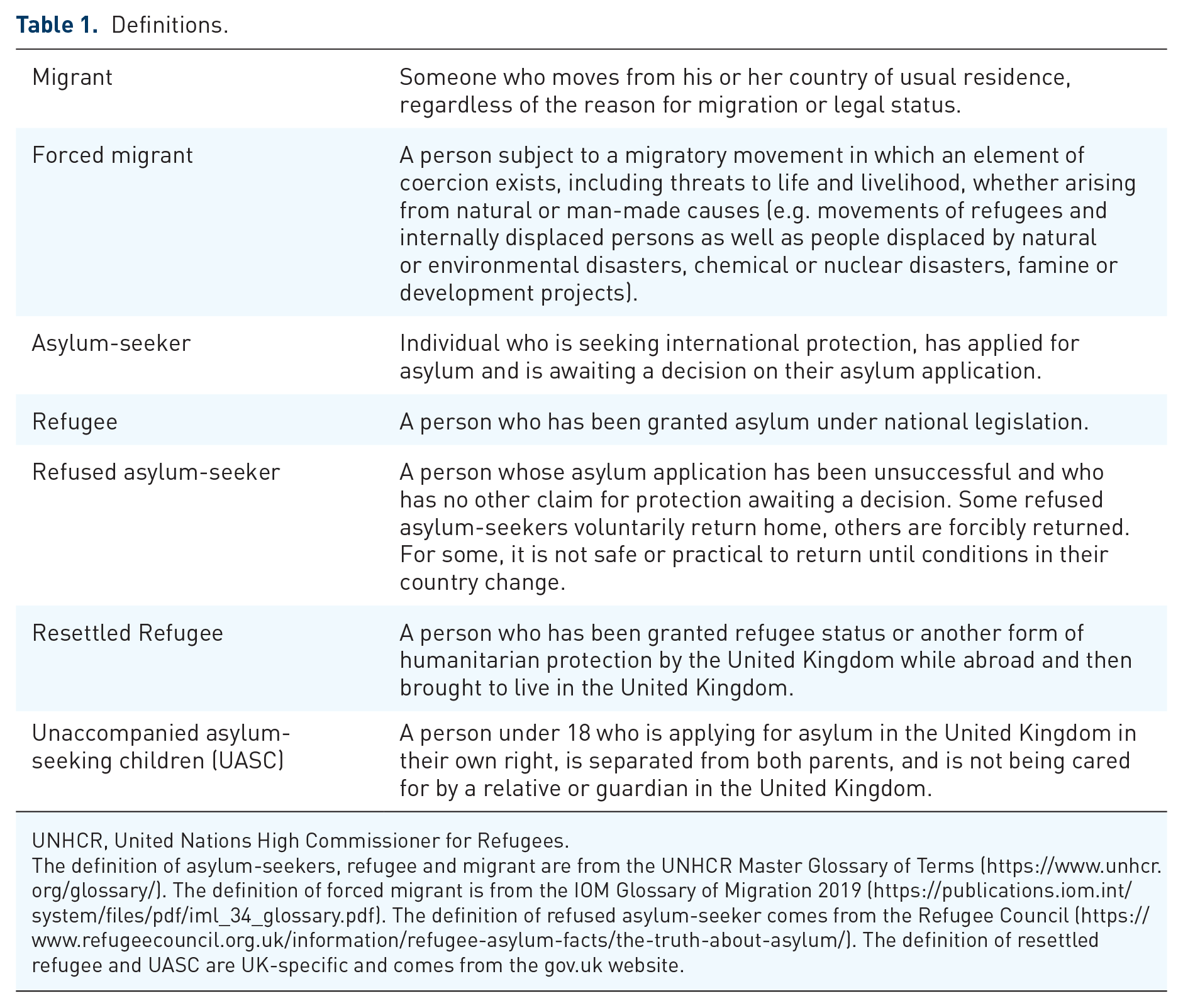
UNHCR, United Nations High Commissioner for Refugees.
The definition of asylum-seekers, refugee and migrant are from the UNHCR Master Glossary of Terms (https://www.unhcr.org/glossary/). The definition of forced migrant is from the IOM Glossary of Migration 2019 (https://publications.iom.int/system/files/pdf/iml_34_glossary.pdf). The definition of refused asylum-seeker comes from the Refugee Council (https://www.refugeecouncil.org.uk/information/refugee-asylum-facts/the-truth-about-asylum/). The definition of resettled refugee and UASC are UK-specific and comes from the gov.uk website.
Access to diagnosis and treatment is often limited due to the disruption of the infrastructure in the country of origin; barriers to accessing healthcare are language, stigma, awareness of entitlement, and limited provision of services. In addition to this, frequent relocations between countries and areas within countries pose further challenges to healthcare provision.
Neglected tropical diseases and infectious diseases
Neglected tropical diseases (NTDs) is an umbrella term encompassing 20 communicable diseases. 5 They are described as being ‘neglected’ due to a paucity of research and treatment options. 6 These medical conditions are often endemic in many low- and middle-income countries and affect almost 2 billion people globally. In the United Kingdom, NTDs are usually identified as imported cases, with statistics available only for three of them. 7 The UK Health Security Agency (UKHSA) has published data on chikungunya and dengue infections occurred in 2014 (347 cases of dengue 8 and 295 cases of Chikungunya 9 ). Rabies is monitored annually and all cases occurring since 1902 were imported, with the last one occurred in 2018. 10
NTDs are often asymptomatic or produce only mild symptoms in early stages of infection. Some NTDs can lead to vertical transmission, and most can be either prevented or treated with public health interventions, screening or early diagnosis. If left untreated, many can result in severe morbidity and mortality such as increased risk of malignancy and end organ damage in later life. Previous studies have demonstrated that asylum-seekers and refugees are more likely to be affected by NTDs such as Chagas disease, schistosomiasis, and filariasis.11,12
This population also has a higher prevalence of infectious diseases such as tuberculosis (TB), human immunodeficiency virus (HIV), hepatitis B, as well as malaria and enteric fevers.13,14
Screening
Screening of infectious diseases in migrant populations has gained considerable attention over the last few decades. In the United Kingdom, and many other European countries, screening practices have been largely targeted towards TB, with a focus on biosecurity and the protection of public health. 15
The first systematic screening programme for infection in migrants, in the United Kingdom, was introduced in 1965 and involved port-of-entry screening for TB with chest radiographs.16–18 Since 2012, those seeking asylum or refuge in the United Kingdom through formal routes (i.e. through refugee resettlement programmes) undergo pre-entry screening for TB, blood-borne infections (BBI); HIV and hepatitis B and C, syphilis and other sexually transmitted infections (STIs), intestinal helminths and malaria before coming to the United Kingdom.19,20
The majority of asylum-seekers do not travel through formal routes and are therefore not screened prior to entry to the United Kingdom. There is currently no statutory requirement to have an initial health assessment or screening for infectious diseases for this population. The UKHSA and the Royal College of Paediatrics and Child Health (RCPCH) have published guidelines to support the holistic assessment and screening of this population at any opportunistic healthcare encounter.21,22 The recommendations are summarised in Table 2.
Summary of the UKHSA migrant health guide.
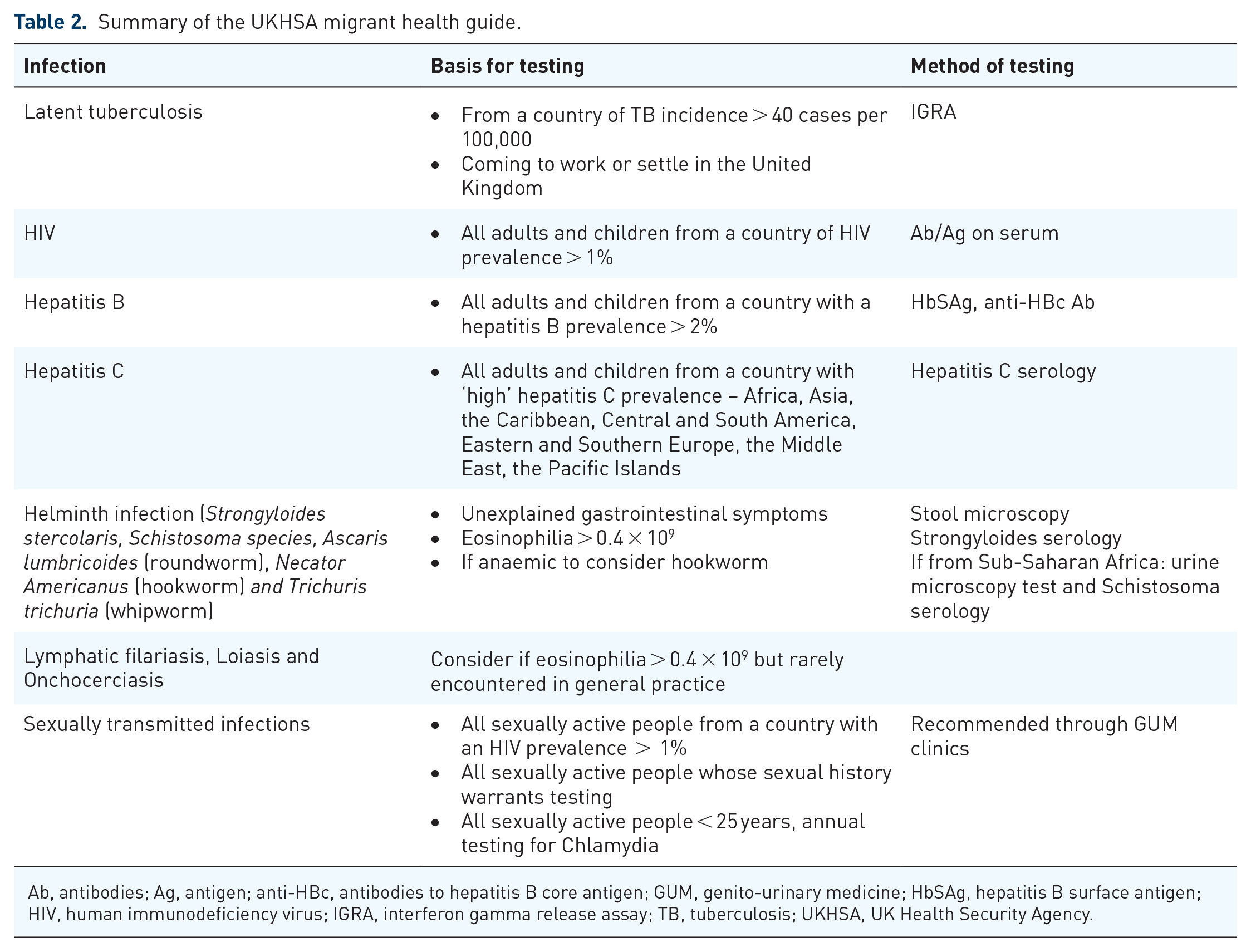
Ab, antibodies; Ag, antigen; anti-HBc, antibodies to hepatitis B core antigen; GUM, genito-urinary medicine; HbSAg, hepatitis B surface antigen; HIV, human immunodeficiency virus; IGRA, interferon gamma release assay; TB, tuberculosis; UKHSA, UK Health Security Agency.
Indiscriminate NTDs screening is not currently recommended by these guidelines; however, investigations for helminth infections, lymphatic filariasis, loiasis and onchocerciasis are suggested if there is a positive history of exposure or eosinophilia is picked up on routine full blood count (FBC) test.
This article reviews the existing literature regarding the approaches to screening for infectious diseases and NTDs in asylum-seekers, refugees and newly arrived migrants in the United Kingdom, and it provides recommendations on how to implement this practice.
Methods
We have searched three databases – MEDLINE, Embase and Global Health – with no time restriction. We used a Boolean search strategy combining keywords and MesH term around three main concepts: ‘asylum-seekers’ or ‘refugees’ and ‘infectious diseases’ and ‘screening’. We restricted the result to studies conducted in the United Kingdom. (Search strategy and details of the methods used are available in Supplementary Materials.)
As the terms ‘refugees’, ‘asylum-seekers’ and ‘migrants’ are sometimes used interchangeably, we have used all the synonyms to avoid omitting studies.
The main objectives of the review are:
To investigate the approaches to infectious diseases and NTDs screening of refugees and asylum-seekers in the United Kingdom;
To explore acceptability, barriers and facilitators of screening practices;
To explore the attitude of healthcare workers towards screening migrants for infectious diseases and NTDs.
We included both qualitative and quantitative studies which described a screening intervention on the target population. We have defined our target population as refugees or asylum-seekers or newly arrived migrants (where newly arrived were defined as arrived in the United Kingdom in the last 5 years). We excluded studies that did not describe a screening intervention or did not focus on our target population. We did not include ‘grey literature’ (i.e. not published in journals or books, not peer-reviewed articles) in our review.
Data were extracted using a form including the following variables: characteristic of the study design, location, screening strategy and screening settings, numbers screened, infection screened and outcomes. For the qualitative studies, the main themes have been grouped in these categories: acceptability, barriers and facilitators in access to care, and attitudes of healthcare workers.
Results
The original search found 110 papers, of which 46 were excluded on the basis of the title and abstract. The full text of 64 articles was analysed, and another 5 articles were identified from Snowball Reference. Twenty articles were included in the literature review, of which 13 were quantitative studies, 6 qualitative and 1 mixed methods (see Figure 1).

Literature review flow chart.
Quantitative studies and mixed methods
Fourteen studies were included in the quantitative analysis, of which one was a mixed method study. Nine studies described a retrospective methodology, with four identified as retrospective cohort study and five as retrospective audit or data analysis. Four studies had a cross-sectional design. The mixed-method study used a retrospective design for the analysis of the quantitative data.
Target population
The target population in the studies was diverse. Only three studies focused on asylum-seekers: one on the adult population, 23 one on unaccompanied asylum-seeking children (UASC) 24 and one on accompanied asylum-seeking children. 25 One study focused on refugees arriving in the United Kingdom through a governmental resettlement programme. 13 Out of the remaining 10 studies, 7 focused on migrants that are described as ‘newly arrived’26–32 and 3 retrospective studies focusing on migrants living in specific locations in the 5 years preceding the analysis.33–35 (Summary tables of the studies included are available in Supplementary Materials.)
Screening strategies
Studies that included NTD screening. Only two studies described a broad approach to screening for infectious diseases including NTDs. Both were cross-sectional studies of specialist paediatric clinics for asylum-seeking children. Harkensee and Andrew 25 screened accompanied asylum-seeking children for infectious diseases based on risk of exposure in country of origin and countries of transit. Children were screened for Latent TB Infection (LTBI), BBI, malaria, strongyloidiasis, schistosomiasis and eosinophilia, which was used as a proxy for parasitic infections. Williams et al. 24 screened UASC in their paediatric infectious diseases clinics in London. The screening was voluntary, offering universal testing to all UASC using a panel-based approach for LTBI, BBI and STIs. All children had an FBC, urine dip and stool for parasitological examination. Where indicated by geographical origin or positive results, serology was performed for schistosomiasis, strongyloidiasis and filarial infection.
Studies screening for multiple infections, excluding NTDs. Two studies screened for multiple infections.13,27 Both studies performed blood tests for LTBI and BBI. One study 13 focused on pre-entry screening and included syphilis testing and the use of chest x-ray (CXR) as a screening strategy to rule out active TB.
Studies screening for single infectious disease. All the remaining studies (10/14) described screening strategies with a focus on a single disease. Nine out of 10 focused on TB screening,23,26,28–34 with the remainder focusing on hepatitis B. 35
Different TB screening strategies were employed. The majority of the studies used interferon- gamma release assay (IGRA) testing, with two of them using additional CXR to detect active TB. Two studies28,32 screened with only CXR as part of port of entry screening. Three studies described the use of tuberculin skin test (TST) in newly arrived migrants, either in combination with CXR, 31 exposure history and symptom screening 23 or TST alone. 30 Finally, one study in Immigration Detention Centre used a verbal TB screening of symptoms and prior diagnosis. 29
Screening settings
Pre-entry screening. Two out of 14 studies described a pre-entry screening practice with migrants screened in their country of origin before reaching the United Kingdom.13,26
Port of entry screening. A further four studies described screening at the port of entry to the United Kingdom, either at shipping ports23,32 or airports. 28 One study described screening at a hospital as the dedicated location for port of entry screening. 30
Screening in primary care in the United Kingdom. Four studies were carried out in primary care settings, with general practitioners being responsible for carrying out the screening.26,27,33,35
Screening in specialist settings in the United Kingdom. A further four studies were conducted in specialist settings of which two of them are TB clinics31,34 and two are paediatric infectious diseases clinics.24,25
Outcomes of infectious diseases screening
Of the studies which considered NTDs as part of their screening, only one study reported positive results. Williams et al. 24 reported that 40% of patients screened had an infection identified: 16% schistosomiasis, 8.6% giardiasis, 8% strongyloidiasis and 7% intestinal tapeworm. The other study did not find any patients with schistosomiasis or strongyloidiasis, but the numbers of patients tested were very low (only 4 out of 80; 5%). They reported a 3.7% rate of unexplained eosinophilia that was treated empirically with mebendazole (Harkensee and Andrew).25
As the focus of this review is on screening for NTDs, we have not reported the rates of other infections detected in the studies included in this review. Interpreting these results would be additionally complex as different methodologies were used in each of the studies, uptake of the investigations in the population and the denominator were often not clearly defined, making inter-study comparison difficult.
Qualitative and mixed-methods studies
We included seven studies in the qualitative analysis: six of them had a qualitative design and one was a mixed-method study which included qualitative data from focus groups. Three studies interviewed service users,25,36,37 and two interviewed service providers.38,39 One study interviewed migrant health community leads representing a dominant migrant group, 40 while the final one interviewed key stakeholders with an interest or experience in migrant health. 41
Acceptability among migrants
Screening for infectious diseases in migrant populations has been generally well received in acceptability studies.36,37
In the Brewin et al. 37 study offering screening for TB, the majority of participants reported finding screening reassuring and seeing it as a socially responsible concept.
Similarly, Eborall et al. 36 found that an infectious diseases screening programme for LTBI and BBI was both acceptable and beneficial by migrants in a primary care clinic in Leicester. Healthcare leads of a migrant community have also reported that screening was acceptable among migrants provided the services are sufficiently accessible. 40
Barriers
Multiple barriers to the implementation of screening programmes have been widely reported.25,38–41 The stigma attached to the diagnosis of certain infectious diseases has been described by both migrants 40 and healthcare workers. 36
Some of the cultural barriers described by service users include staff being ‘culturally insensitive’ and the services not being ‘migrant friendly’. 40 Asylum-seeking families interviewed by Harkensee and Andrew 25 reported a perception of healthcare systems failing to adapt to their needs. Additional barriers to accessing healthcare are fear of deportation,40,41 not having English as a first language or lack of availability of appropriate translation services, 38 lack of information surrounding the entitlement to healthcare as well as a lack of awareness of the relevant services that are provided. 40
Healthcare workers interviewed in two other studies cited the limited capacity and time constrictions in the National Health Service (NHS) as having a negative impact on the ability of services being able to respond to the needs of refugees and asylum-seekers.39,41
Facilitators
The importance of community members with lived experience as peer-educators and champions of health promotion have been highlighted in the study by Berrocal-Almanza et al. 41 This is further supported by the linkage of higher acceptability and participation in screening programmes when conducted in community settings or settings where access is easier.25,40,41
Primary care settings are perceived as being safer for TB screening by a migrant population in London, and screening for infectious diseases was felt to be more acceptable when embedded in a general health check-up 40 in addition to screening for a broader number of infections. 36
Additional structural facilitators such as the availability of more appointments and the presence of translators have been described by asylum-seeking families interviewed. 25
Attitude of healthcare workers
Only one study focused on healthcare workers’ attitudes towards infectious diseases screening in the migrant population. 38 Only 29% of those surveyed would consider screening a migrant who was newly registered at the practice for BBI and TB. In addition, the majority of primary care staff surveyed (78.9%) reported that they would identify existing migrants for testing opportunistically, rather than inviting them for a routine screening appointment. 38
Discussion
Reviewing the existing literature has highlighted that despite disproportionately affecting asylum-seeker and refugee populations,11,24,42 NTDs are rarely screened for in routine UK practice. Although recommended, 21 screening is not part of a set of implemented guidelines or NHS regulatory standards, thereby adding barriers to this practice. In the two studies including NTDs screening in their protocols, the testing was selective and targeted, focusing on a limited number of infections: schistosomiasis, strongyloidiasis, filariasis and intestinal parasites.24,25
There are complex reasons why heterogeneous approaches to screening for NTDs have been adopted. A universal screening programme, by definition, must be able to identify asymptomatic conditions in a target population, using acceptable and cost-effective tests. Interventions should have a clear benefit to the health and well-being of the individuals both directly and indirectly affected.
NTDs can be categorised into three groups based on the feasibility of screening (Table 3). For some NTDs, the principles of screening would not be applicable as they either present symptomatically or are rare, there is no effective treatment or there is no screening test available. For example, dengue, chikungunya and human African trypanosomiasis would present with specific signs and symptoms. Similarly, for rabies and snake bites, in the absence of a history of exposure, there would be no clinical need for screening.
List of neglected tropical diseases subdivided by screening applicability.

The indication for screening of other NTDs such as leprosy, leishmaniasis, Buruli ulcer, cysticercosis, echinococcosis, filariasis, trachoma and onchocerciasis is not as clear. While these conditions may pose a high risk of morbidity and mortality to the individual, other strategies may be more relevant and cost-effective for the early identification, recognition and treatment of these conditions. Possible alternative interventions are raising awareness among the migrant communities to seek early medical advice and improving the education of both service users and service providers as to the signs and symptoms indicative of NTDs endemic in low- and middle-income countries. Some examples where education of both service users and service providers may be of benefit are new cutaneous ulcers found in a migrant patient should lead to the consideration of leishmaniasis or Buruli ulcer if endemic in their country of origin; new seizures in a patient from rural Peru should ring alarm bells for cysticercosis; anaesthetic, discoloured patches of skin, thickened nerves or nodules as well as loss of eyebrows in patients from India would make leprosy a diagnostic possibility.
For other NTDs such as strongyloidiasis and soil-transmitted helminths, the benefit of screening is undoubtedly relevant. These are relatively common conditions endemic in broad geographical areas, with reliable and reproducible tests and safe and cost-effective interventions. The same is true for both schistosomiasis and Chagas disease if the individuals have lived in endemic countries.
While we have found some evidence of screening for schistosomiasis, strongyloidiasis and soil-transmitted helminths in our review, Chagas disease is not mentioned. One of the reasons is that this disease is geographically circumscribed to Central and South America. Historically, migration from this area has been directed to Southern Europe (mainly Spain, Portugal and Italy); therefore, there may be less awareness among healthcare professionals in the United Kingdom regarding the exposure risks in this population. This has been highlighted by a study conducted out of one of the main specialist centres in the United Kingdom, looking at the delay in diagnosis of Chagas disease. This study showed that a significant proportion of patients had severe, life-threatening complications such as cardiomyopathy at initial presentation to healthcare settings. 43 Another study from the same centre showed a low uptake of antenatal screening in pregnant women despite the increased risk of vertical transmission and congenital disease. 12 One potential contributor of this low uptake may be that the Latinx in the United Kingdom are often undocumented, may be living in precarious conditions, and could be marginalised due to a limited command of the English language. 44 These factors can lead to additional barriers to the access of healthcare services in the United Kingdom. Chagas disease is therefore a good example of how a comprehensive screening programme for Latinx, improved education for healthcare providers as well as raised awareness in the community would be beneficial both for the individual and as a public health intervention.
Two broad approaches to the screening for infectious diseases in migrant populations were identified in this review: targeted screening and panel testing. Panel testing is defined as universal screening regardless of the country of origin, while targeted screening implies testing only for certain NTDs based on risk assessment (i.e. prevalence of the disease in the country of origin or transit). There are pros and cons to both of these strategies. It was generally found that panel testing for infectious diseases and NTDs was a more acceptable approach than testing for single infections. This was especially highlighted when screening was perceived as being part of a general check-up. 40 This approach also led to a reduction of the stigma attached to screening for certain infections, thus underlining the importance of a holistic approach to the health needs of this vulnerable population. 40 There are multiple considerations that can be attributed to the perceived benefits of panel testing including the following: reduction in recall bias (the exact geographical locations transited may not be known or remembered accurately), reduction in risk of re-traumatisation of vulnerable individuals (repeated requests to recount the exact journey taken in seeking refuge and asylum) and reduction in appointment length (by removing the need to discuss and document the exact journey taken). However, certain NTDs are only endemic in distinct geographical areas; therefore, panel testing may not only have cost implications but result in less accurate diagnoses. A geographical approach requires a more in-depth knowledge of the epidemiology of infectious diseases by the healthcare provider but will reduce the additional burden placed on specialist parasitology laboratories and reduce the risk of false-positive/cross-reactive serological investigations.
Nonetheless, our review found that in the United Kingdom, there has been a huge heterogeneity of screening strategies, with only 6 out of 16 studies using a broader approach to infectious diseases screening. The majority of the studies focused instead on a single disease, mainly TB. This is consistent with previous research 15 and with surveys of infectious diseases experts. 45 It may reflect the level of attention given to reducing the burden of TB by policy makers.
The different screening strategies for TB found in the literature review mirror the policy changes in the United Kingdom to tackle active and latent infection in this population. Port of entry screening was abandoned in 2012 and replaced by pre-entry TB screening. 19 There are, however, no strategies that have been developed to try to reach more vulnerable groups of migrants such as those who travel via ‘informal routes’ and remain undocumented.
When looking at screening settings, appointments in primary care and community settings were deemed the most acceptable by the service users.25,37,40,41 The most likely reasons for this are accessibility, cost of travel and awareness of existing services in addition to the awareness of the rights to access the existing services. 25 This highlights the importance of developing health services which are adaptable to the needs of the population. Interestingly, despite outreach interventions having proved to be successful in other socially marginalised groups,46,47 no study mentioned the use of outreach teams in settings such as contingency accommodation or other non-healthcare community settings.
One of the limitations of our search strategy is the inclusion of studies with a broad concept of ‘migrant’ rather than restricting the search to asylum-seekers and refugees. This is due to the fact that these terms are often used interchangeably in the literature, and focusing on a narrower concept would have risked omission of relevant studies. Only three of the included studies focused specifically on asylum-seekers23–25 and one on refugees. 13 The target population of the majority of the studies was newly arrived migrants, without distinction on their ‘status’. We recognise it may be difficult to characterise these distinct populations given the political implication of the legal status/right to remain. However, we believe that identification of the different sub-population of migrants is likely to be of benefit to them. This would allow for services to flexibly meet their specific health and social care needs. While asylum-seekers and refugees are often complex and highly vulnerable individuals, the majority of migrants to the United Kingdom move from high-income settings with a high educational level and standard of living. In addition to this, the ‘healthy migrant effect’ is often seen, whereby new arrivals to a country have a reduced burden of both communicable and non-communicable diseases when compared with the general population of the host nation.48,49
This review has highlighted the lack of evidence around infectious diseases screening strategies focusing on asylum-seekers and refugees. The paucity of data addressing the uptake of screening programmes, the effectiveness of different screening strategies and lack of outcome measures of the screening add to the challenges faced by healthcare professionals and policy makers. It is therefore not feasible at present to make generalisable recommendations for panel-based NTD screening. Additional research would be of benefit to try to address this gap in knowledge.
When planning screening interventions, priority should be given to the identification of outreach settings (such as hotels or migrant community centres), community engagement and using peer support workers. More attention should be placed on the identification of sub-groups of the migrant population thus allowing more focus to be given to specific needs within these groups.
On balance, we recommend that screening for some NTDs alongside broader infectious diseases screening is considered as part of a comprehensive health assessment of this population. We believe that this strategy would contribute to lowering the stigma associated with the diagnosis of certain diseases and increasing screening acceptability.
Ultimately, screening policies should aim to overcome the barriers in accessing healthcare for these vulnerable populations, providing early recognition and treatment of diseases with potential long-term consequences to health and well-being.
Supplemental Material
sj-doc-2-tai-10.1177_20499361221116680 – Supplemental material for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom
Supplemental material, sj-doc-2-tai-10.1177_20499361221116680 for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom by Paola Cinardo, Olivia Farrant, Kimberlee Gunn, Allison Ward, Sarah Eisen and Nicky Longley in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-doc-3-tai-10.1177_20499361221116680 – Supplemental material for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom
Supplemental material, sj-doc-3-tai-10.1177_20499361221116680 for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom by Paola Cinardo, Olivia Farrant, Kimberlee Gunn, Allison Ward, Sarah Eisen and Nicky Longley in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-1-tai-10.1177_20499361221116680 – Supplemental material for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom
Supplemental material, sj-docx-1-tai-10.1177_20499361221116680 for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom by Paola Cinardo, Olivia Farrant, Kimberlee Gunn, Allison Ward, Sarah Eisen and Nicky Longley in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-4-tai-10.1177_20499361221116680 – Supplemental material for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom
Supplemental material, sj-docx-4-tai-10.1177_20499361221116680 for Screening for neglected tropical diseases and other infections in refugee and asylum-seeker populations in the United Kingdom by Paola Cinardo, Olivia Farrant, Kimberlee Gunn, Allison Ward, Sarah Eisen and Nicky Longley in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.