
Abstract
Background:
Reduced or delayed access to medical resources on weekends could lead to worsening outcomes, in critically ill infected patients requiring intensive care unit (ICU) admission.
Objective:
To investigate the “weekend effect,” on critically ill infected patients in Japanese ICUs for the first time.
Design:
Multicenter retrospective cohort study.
Methods:
We examined data from Japanese ICU patients participating in the DIANA study, a multicenter international observational cohort study. This prospective investigation enrolled critically ill patients with infections admitted to the ICU. The primary endpoint was successful discharge from the ICU within 28 days of admission. Outcome measures were evaluated through both univariate and covariate Cox regression analyses, providing hazard ratios (HRs) along with estimated 95% confidence intervals (CIs).
Results:
Out of the 276 patients enrolled in the DIANA study across 31 facilities, 208 patients (75.4%) meeting the inclusion criteria were included in the analysis. The weekday ICU admission group comprised 156 patients (75.0%), while the weekend ICU admission group comprised 52 patients (25.0%). In the multivariate Cox regression analysis, there were no statistically significant differences observed in the rates of ICU discharge alive within 28 days and 14 days (28 days, HR: 0.94, 95% CI: 0.63–1.40; 14 days, HR: 0.97, 95% CI: 0.64–1.48). Furthermore, the overall ICU mortality rates at 28 days and 14 days after ICU admission did not show statistical significance between patients admitted on weekends and those admitted on weekdays (ICU mortality, 28 days: 13.5% vs 11.5%, p = 0.806; 14 days: 7.7% vs 10.9%, p = 0.604).
Conclusion:
The rates of ICU discharge alive within 28 days after ICU admission did not differ significantly between weekday and weekend admissions, both in the unadjusted and adjusted analyses. Moreover, further well-designed studies are warranted to thoroughly assess this effect.
Plain language summary
Why was the study done? Patients with severe diseases (e.g., acute myocardial infarction) tend to have poor outcome when they admitted to the hospital in weekends because of insufficient medical resources. We examined the weekend effects of patients with severe infections requiring admission to intensive care units (ICUs) because it is poorly understood. What did the researchers do? We studied using the data from the DIANA study (a multicenter international observational cohort study in Japan). This retrospective study included critically ill infected patients admitted to the ICU. What did the researchers find? Among 276 patients at 31 facilities enrolled in the DIANA study, There were 156 patients (75.0%) in the weekday ICU admission group and 52 patients (25.0%) in the weekend ICU admission group. There are no significant differences between patients admitted on weekends and those admitted on weekdays both in Discharged alive from the ICU rate within 28 days and ICU mortality 28 days and 14 days after ICU admission. What do the findings mean? Our study showed there is no difference between the outcomes of patients with severe infection between weekday and weekend admissions. If the weekend effect largely depends on procedural delays, it may be less marked in critically ill infected patients than in other severe diseases. Further, well-designed studies are required to assess this effect better.
Background
Severe infections are the most prevalent cause of death in patients admitted to intensive care units (ICUs) and are potentially life-threatening. 1 Sepsis, a complication of infection, represents a major health burden worldwide and is estimated to affect more than 30 million people every year, potentially leading to 6 million deaths. 2 Compelling evidence has shown that prompt diagnosis and treatment can improve the outcomes.3–8 Kumar et al. reported that for every additional hour delay in initiating antimicrobial treatment in the first 6 h after hypotension onset, the survival dropped by an average of 7.6%. Recent research has identified “the time of the week” among the many risk factors, which is sometimes disregarded, for poor prognosis in patients presenting with time-sensitive medical emergencies. Some previous reports demonstrated that patients admitted to the hospital for treatment on weekends experience worse outcomes than those admitted on weekdays.9–13 Despite many studies examining this “weekend effect” on various medical emergencies, such as cardiac arrest, acute coronary syndrome, esophageal variceal hemorrhage, stroke, and non-elective surgical patients, there are not many studies on the “weekend effect” on sepsis. Herein, we examined the “weekend effect” on critically ill infected patients in Japanese ICUs for the first time.
Methods
Participants
This study constituted a post hoc subgroup analysis derived from an international prospective cohort study known as the Determinants of Antimicrobial Use and De-escalation in Critical Care (DIANA) study. DIANA, endorsed by the European Society of Intensive Care Medicine, was a multicenter observational cohort study that investigated patients receiving empirical antimicrobial treatment in the ICU. It enrolled 1495 patients from 152 ICUs across 28 countries worldwide. Our analysis focused on patients registered in the Japanese ICU database. They were chosen to represent a diverse cross-section of healthcare settings across the country. Participants in the DIANA study were recruited between October 2016 and May 2018. 14 Inclusion criteria comprised individuals aged 18 years or older admitted to the ICU with an anticipated requirement for at least 48 h of ICU support. Empirical antimicrobial therapy initiation was either in the ICU or within 24 h before ICU admission, aimed at suspected community-, healthcare-, hospital-, or ICU-acquired bacterial infections.
Exclusion criteria involved participants lacking adequate admission or discharge data. In addition, individuals included in the DIANA study more than 2 days post-ICU admission were excluded, as they were presumed to have acquired ICU-related infections for reasons other than severe infection necessitating ICU admission. Participants were categorized into weekday (Monday to Friday) and weekend (Saturday and Sunday) admission groups.
The study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations.
Data collection variables and outcome
We collected the following data from the database: background on infectious diseases, including healthcare exposure, immunosuppression, infectious focus (respiratory tract, gastrointestinal tract, skin and soft tissue, genitourinary tract, catheter-related, other focus, and unknown), septic shock, causative microbial identification, multiple bacterial identifications (when each patient had more than one infection or pathogen), bacteremia, need for source control, and empirical antimicrobials. Patient characteristics included sex, age, disease categories (medical, surgical, and trauma) on ICU admission, ICU admission diagnosis, comorbidities, and severity of the condition on ICU admission as measured by the Acute Physiology and Chronic Health Evaluation (APACHE) II, Simplified Acute Physiology Score (SAPS) II, and Sequential Organ Failure Assessment (SOFA) scores.
The primary outcome variable was alive ICU discharge within 28 days of ICU admission. We examined the cumulative incidence of this event at 14 and 28 days. Our variable of interest was “weekend ICU admission.”
Variables included in the multivariable Cox regression model were selected based on clinical significance and insights from previous literature. In particular, variables consistently identified as significant predictors of outcomes in similar studies were included. The following confounding variables were considered: age,15,16 sex, 17 body mass index (BMI), 18 septic shock (defined as hypotension requiring vasopressor use to maintain a mean blood pressure ⩾65 mmHg and/or serum lactate level >2 mmol/l (>18 mg/dl) persisting after adequate fluid resuscitation), chronic illness (one or more of the following: chronic pulmonary disease, chronic hepatic disease, chronic renal failure, diabetes mellitus, cardiovascular disease, solid tumor, hematologic malignancy, and cerebrovascular disease),19,20 immunosuppressed status (including congenital immunodeficiency, neutropenia (absolute neutrophil count < 1000/µl), receipt of corticosteroid treatment (prednisolone or equivalent > 0.5 mg/kg/day) for >3 months prior to study inclusion, solid organ transplant patients receiving immunosuppressive treatment, bone marrow transplant patients receiving immunosuppressive treatment, administration of chemotherapy within 1 year prior to study inclusion, administration of radiotherapy within 1 year before study inclusion, patients with autoimmune diseases receiving immunosuppressive treatment, and human immunodeficiency virus/acquired immunodeficiency syndrome), 21 SAPS II score on ICU admission, 22 renal replacement therapy,23,24 relapse of the primary infection, 25 healthcare exposure (one or more of the following: hospitalization for ⩾2 days in the 12 months before study inclusion (excluding the current episode), antibiotic exposure in the last 3 months before study inclusion, residency in a nursing home or long-term care facility before study inclusion, receiving chronic hemodialysis before study inclusion, or receiving invasive procedures (at home or in an outpatient clinic) in the last 30 days before study inclusion), 26 probable infection focus (gastrointestinal tract and/or respiratory tract),27,28 and causative pathogen (Staphylococcus aureus, fungus, and Pseudomonas aeruginosa).29–31 We focused on three of the most common causes of infection associated with higher ICU mortality.29–31
Infection relapse was defined as the recurrence of infection with the same causative microorganism (possibly with a different susceptibility pattern) at the same infection site, occurring after the cessation of all antimicrobial agents used to treat the primary infection under study.
Statistical analyses
Continuous variables were presented as mean, standard deviation, median, and interquartile range (IQR), and categorical variables were presented as numbers and percentages. Categorical variables are tested by Fisher’s exact test and continuous variables by the Wilcoxon Signed-rank test. The outcome was assessed using both non-adjusted and adjusted Cox regression models, from which hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated. The cumulative incidence of an event (live discharge from the ICU within 14 and 28 days) was evaluated using Gray’s test. Mortality was assessed using Fisher’s exact test. All statistical analyses were conducted using R software (version 4.0.3 for Windows; R Foundation for Statistical Computing, Vienna, Austria). All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
Results
Characteristics of the study population
Out of the 276 patients enrolled in the DIANA study across 31 facilities in Japan, 208 (75.4%) patients meeting the inclusion criteria were included in the analysis. The range of ICU beds varies widely, with an average of 12.5 beds (standard deviation of 6.9). We excluded 68 patients with incomplete medical records. There were 156 patients (75%) in the weekday ICU admission group and 52 patients (25%) in the weekend ICU admission group (Figure 1). Table 1 displays the general characteristics of the study population. The median age of the cohort was 72.5 years (IQR, 61.0–80.3). More than half of these patients were male (56.7%) and 34.1% presented with septic shock. The APACHE II, SAPS II, and total SOFA score on the day of ICU admission were 20.5 (IQR, 16.0–26.3), 46.0 (IQR, 32.0–58.0), and 8.0 (IQR, 5.0–11.0), respectively. Weekend and weekday admissions exhibited similar patient and hospital characteristics. The median ages of the two groups were similar (72.0 vs 73.5 years old, p = 0.973). More male patients were admitted on weekdays than weekends, but the difference was not statistically significant (60.3% vs 46.2%, p = 0.106). The severity of illness on the day of ICU admission (median APACHE II, 20.0 vs 22.0, p = 0.497; SASP II, 43.0 vs 53.0, p = 0.128; and total SOFA score, 7.0 vs 9.0, p = 0.055, respectively), the proportion of patients with previous healthcare exposure, and the proportion of immunosuppressed patients (Table 1) were not significantly different between the two groups. The most common probable infection focus was lower and upper respiratory tract infection in both groups (37.2% vs 51.9%, p = 0.074).

Flow diagram of the study.
Patient characteristics.

Categorical variables are tested by Fisher’s exact test and continuous variables by the Wilcoxon Signed-rank test.
APACHE II, Acute Physiology and Chronic Health Evaluation II; BMI, body mass index; ICU, intensive care units; SAPS II, The Simplified Acute Physiology Score II; SOFA, Sequential Organ Failure Assessment.
Discharge alive from the ICU rates within 28 days and 14 days
An unadjusted analysis of the outcomes, including a univariate Cox regression analysis, is presented in Tables 2 and 3. The proportion of patients discharged alive from the ICU within 28 days and 14 days were 86.5% on a weekday, 84.6% on a weekend (HR, 0.73; 95% CI, 0.52–1.03), and 79.5% on a weekday, and 67.3% on a weekend (HR, 0.68; 95% CI, 0.47–0.99), respectively. The proportion of patients discharged alive from the hospital within 28 days and 14 days was 76.8% on a weekday, 76.0% on a weekend (HR, 0.75; 95% CI, 0.44–1.27), and 44.6% on a weekday, and 33.3% on a weekend (HR, 0.63; 95% CI, 0.29–1.38), respectively. In multivariate Cox regression analysis, discharge alive from the ICU rates within 28 days and 14 days were not statistically significant (28 days, HR, 0.94; 95% CI, 0.63–1.40; 14 days, HR, 0.97; 95% CI, 0.64–1.48). The cumulative survival curves are shown in Figure 2.
Outcomes.

Univariate and multivariate analyses (28-day discharge ICU alive).
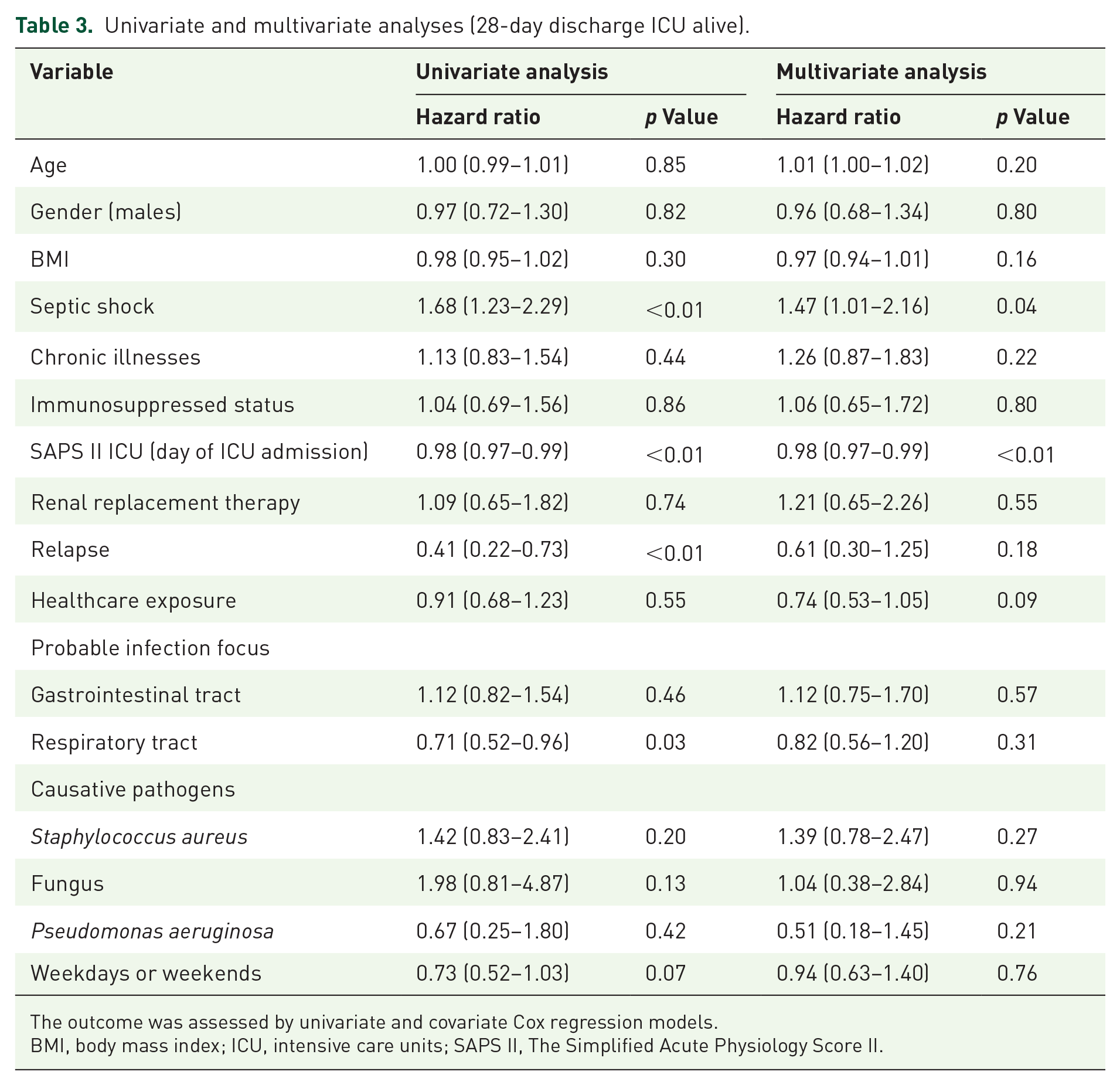
The outcome was assessed by univariate and covariate Cox regression models.
BMI, body mass index; ICU, intensive care units; SAPS II, The Simplified Acute Physiology Score II.

Cumulative survival rate.
Mortality
Overall, ICU mortality rates at 28 days and 14 days after ICU admission did not show statistical significance between patients admitted on weekends and those admitted on weekdays (ICU mortality at 28 days: 13.5% vs 11.5%, p = 0.806; at 14 days: 7.7% vs 10.9%, p = 0.604).
Discussion
Although a limited number of studies have explored the weekend effects for critically ill infected patients requiring ICU admission, there has been no research targeting Japanese ICUs. This is the first study to explore the association between weekend ICU admissions and the prognosis of critically ill infected patients in Japanese ICUs. The results revealed no weekend effect in patients discharged alive from the ICU within 28 days of ICU admission. These results are consistent with some previous reports but contradict other studies. In 2013, Powell et al. analyzed 114,611 emergency department admissions with a principal diagnosis consistent with sepsis. They found that the difference in overall inpatient mortality, in terms of the weekend, was not significant (17.9% vs 17.5%, p = 0.08). 32 On the other hand, in 2016, Shin et al. studied 398,043 patients with severe sepsis. Patients admitted on weekdays had a lower 7-day mortality rate (OR = 0.89, 95% CI 0.87–0.91), 14-day mortality rate (OR = 0.92, 95% CI 0.90–0.93), and 28-day mortality rate (OR = 0.97, 95% CI 0.95–0.98) compared to those admitted on weekends. 33 The disparities observed among studies could be attributed to variations in the organization of care within ICUs or differences in the study populations.
Herein, we investigate the factors contributing to the absence of significant disparities observed in various other life-threatening conditions. The weekend effect, known to result in delays in emergency care, surgical procedures, or interventions requiring specialist coordination that may not be readily accessible outside regular working hours, is one such factor. Several studies have indicated that, even after accounting for procedural delays, there is no discernible difference in overall in-hospital mortality rates for patients admitted on weekends, suggesting that procedural delays largely underlie the etiology of the weekend effect.34–36 If the weekend effect largely depends on procedural delays, it may be less marked in critically ill infected patients than in other life-threatening conditions such as myocardial infarction or patients requiring non-elective surgery. This is because most infected patients do not necessitate the activation of specialty procedure laboratories or the operating room. For example, concerning cardiac care units, additional factors that could contribute to elevated mortality rates during off-hours include the availability of skilled personnel and diagnostic tests, the staffing levels of physicians and nurses, as well as human factors such as sleep deprivation and fatigue. However, most of these problems can be addressed in the ICU. All services, including diagnostic procedures, optimal treatment, and necessary staffing, will likely be fully and immediately available 24/7 in the ICU. The impact of an intensivist's presence during off-hours or unit organization on ICU mortality remains uncertain.37,38 Thus, the possible need for special procedures, such as surgery or catheterization, may be a major factor in the weekend effects of life-threatening conditions.
In addition, the idea that there are fewer physicians on weekends and that it takes more time to deal with emergencies may not necessarily be true for ICUs. Luyt et al. demonstrated that off-hour admissions (off-hour admissions encompassed night-time (6:00 p.m. to 7:59 a.m.), weekends (from Saturday 08:00 a.m. to Monday 7:59 a.m.), and holidays admissions) were not associated with higher mortality and may even be associated with a lower death rate in all adults (⩾18 years) admitted to a tertiary care medical ICU. 39 Luyt et al. provided possible explanations for their findings. For example, the daytime may be more hectic than the night-time for both physicians and nurses; they may have more regular work during the daytime, including a higher volume of new orders, the need to perform more procedures, and conference discussions. There may be fewer physicians in ICUs during off-hours or weekends; however, this may be offset by the lower workloads of physicians and nurses.
This study had several limitations. First, increasing the sample size might help to clarify the difference between the two groups. The possibility of random error will likely be mitigated by this. Second, we did not record the time of ICU admission. We could not assess the prognosis between off-hours and non-off-hours. Some reports have shown that patients admitted to the ICUs at night demonstrate worse prognosis than those admitted in the daytime, while others do not.40–42 However, our study did not compare off-hours and in-hours. Third, we did not distinguish between admissions from the emergency department and ward admissions. These two patient groups may have had different characteristics. Fourth, data on mortality after ICU discharge and the reason for discharge from the ICU were not collected. Some patients discharged from the ICU may withdraw from therapy and choose palliative or end-of-life care. Fifth, the findings may not be applicable beyond Japan as all participants were admitted to ICUs within Japan. Intensive care resources in Japan are comparatively limited, with fewer ICU beds and intensivists per 100,000 people compared to countries like the US (34.7 beds) and Germany (29.2 beds), whereas Japan has only 5.1 beds per 100,000 individuals.43–46 In addition, open ICUs are more common in Japan, while closed ICUs, which allow closer doctor communication and have lower mortality rates, are more prevalent elsewhere. Taking these factors into account, the role of ICUs in Japan may differ to some extent from that of ICUs in other countries. The average number of ICU beds at the participating centers is 12.5 which is close to that of the average number of 11.6 ICU beds in each hospital with an ICU, according to data from the Japanese Society of Intensive Care Medicine.45,46 Finally, the proportions of patients with respiratory and genitourinary tract infections were higher among those admitted during weekends, which may suggest that weekend admissions included milder cases compared to weekday admissions. In the multivariable Cox regression analysis, we adjusted for this difference in severity by including these two variables. Consequently, our results are representative of the conditions in major Japanese acute-care hospitals. Our analysis cannot completely eliminate confounding factors. However, considering that a prospective study to investigate whether patients are admitted on weekdays or weekends is not feasible, we believe our analysis is sufficiently reliable given the methods currently available.
Conclusion
The findings of this study could not demonstrate a weekend effect on outcomes of critically ill infected patients requiring ICU admission. There were no statistically significant differences in the proportions of patients discharged alive from the ICU within 28 days after ICU admission between weekday and weekend admissions, both in the unadjusted and adjusted analyses.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241292626 – Supplemental material for The weekend effect in critically ill patients with severe infections in Japanese intensive care units: a multicenter retrospective cohort study
Supplemental material, sj-docx-1-tai-10.1177_20499361241292626 for The weekend effect in critically ill patients with severe infections in Japanese intensive care units: a multicenter retrospective cohort study by Teiko Kawahigashi, Taisuke Jo, Tetsuya Komuro, Jan De Waele, Liesbet De Bus, Akihiro Takaba, Akira Kuriyama, Atsuko Kobayashi, Chie Tanaka, Hideki Hashi, Hideki Hashimoto, Hiroshi Nashiki, Mami Shibata, Masafumi Kanamoto, Masashi Inoue, Satoru Hashimoto, Shinshu Katayama, Shinsuke Fujiwara, Shinya Kameda, Shunsuke Shindo, Taketo Suzuki, Toshiomi Kawagishi, Yasumasa Kawano, Yoshihito Fujita, Yoshiko Kida, Yuya Hara, Hideki Yoshida, Shigeki Fujitani and Hiroshi Koyama in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.