
Abstract
Objective
To investigate the impact of pulmonary Acinetobacter baumannii infection on the prognosis of patients in a Chinese neurological intensive care unit (NICU).
Methods
Patients with pulmonary infection and positive sputum culture findings were retrospectively enrolled. Logistic regression analysis was used to determine the factors influencing prognosis. Neurological disease improvement/nonimprovement and mortality rates were assessed.
Results
The study included 374 NICU patients with pulmonary infection (110 [29.4%] with A. baumannii, 264 [70.6%] with other micro-organisms). A. baumannii infection (OR = 2.987) and invasive mechanical ventilation (OR = 16.898) were independent factors in disease prognosis. A. baumannii infection was associated with longer NICU stay, fewer improved patients and increased mortality rate compared with other pulmonary infections.
Conclusions
A. baumannii infection prolongs the duration of the NICU stay and negatively impacts on prognosis. Prognosis of NICU patients could be improved by controlling A. baumannii infection.
Introduction
The emergence of super-bacteria that are resistant to multiple antibiotics is an unprecedented challenge facing the medical community. Novel concepts and treatments are needed to fight bacterial disease, including strict control of antibiotic use. An understanding of the frequency of different bacterial infections in varying pathological conditions and their influence on prognosis are both required for the rational use of antibiotics. Our research investigating pulmonary infection pathogens in the neurological intensive care unit (NICU) revealed Acinetobacter baumannii to be one of the most common micro-organisms found in this setting. 1 The aim of the present study, therefore, was to investigate the effect of A. baumannii infection on NICU inpatient prognosis.
Patients and methods
Study population
This clinical, retrospective study recruited patients with pulmonary infection and positive sputum culture findings who were admitted to (and subsequently discharged from) the NICU of The First Affiliated Hospital of Chongqing Medical University, China, between January 2006 and December 2010. The criteria for pulmonary infections included: fever (≥38℃ for >2 days); cough; sticky sputum; increased leucocyte count (>10 × 109/l); and harsh breath sounds with dry and medium rales or wheezy phlegm. 2 Signs of pulmonary infection were observed on chest X-radiography or computed tomography. Routine sputum specimens were submitted for analysis; bronchoalveolar lavage fluid was collected if the patient underwent tracheal intubation or tracheotomy. Bacterial identification and antibiotic susceptibility tests were performed on all specimens, using a VITEK® 2 system (bioMérieux, Marcy-l’Etoile, France) in the Department of Microbiology, The First Affiliated Hospital of Chongqing Medical University, China, with reference to Pseudomonas aeruginosa ATCC 27853, Staphylococcus aureus ATCC 25923 and Escherichia coli ATCC 25922 standard quality control strains (National Committee for Clinical Laboratory Standards, China).
Criteria for NICU admission, refusal and discharge were formulated according to criteria for general ICU admission 3 and neurology characteristics. The standardized criteria for refusing NICU admission included brain death, chronic brain injury without acute symptoms and mental illness. Discharge criteria comprised essentially stable vital signs, including body temperature, heart rate, respiration, blood pressure fluctuating within normal range for >2 days, aetiology of acute nervous system damage controlled or removed, and no requirement for ventilator support.
The Ethics Committee of the First Affiliated Hospital of Chongqing Medical University, China approved the study, and all patients provided written informed consent prior to enrolment.
Data collection
The following data were collected from medical records: sex; age; medical insurance status; hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg); diabetes; chronic obstructive pulmonary disease (COPD); coronary heart disease; A. baumannii infection; concurrent infection; use of invasive mechanical ventilation; serum albumin; haemoglobin; lymphocyte percentage; severity of disease (Acute Physiology and Chronic Health Evaluation[APACHE] II score 4 ); the numbers of patient improvements (unaffected or slightly affected health-related quality-of-life [HRQoL]; assessed via SF-36 questionnaire 5 ), nonimprovements (severely affected HRQoL) and deaths; duration of stay in the NICU; total duration of hospital stay.
Statistical analyses
Data were presented as mean ± SD or n (%). Between-group comparisons were made using Student’s t-test or χ2-test. Logistic regression analysis was used to determine the effect of sex, age, medical insurance status, hypertension, diabetes, COPD, coronary heart disease, A. baumannii infection, concurrent infection, use of invasive mechanical ventilation, serum albumin, haemoglobin, lymphocyte percentage and APACHE II score on prognosis. Statistical analyses were performed using SPSS® software, version 13.0 (SPSS Inc., Chicago, IL, USA) for Windows®. P-values < 0.05 were defined as statistically significant.
Results
Demographic and clinical characteristics of patients with pulmonary infection admitted to a Chinese neurological intensive care unit, stratified by infecting micro-organism.

Data presented as mean ± SD or n (%).
No statistically significant between-group differences (P ≥ 0.05; χ2-test for categorical variables, Student’s t-test for continuous variables).
COPD, chronic obstructive pulmonary disease.
Micro-organisms associated with pulmonary infection in patients admitted to a Chinese neurological intensive care unit (n = 374).

Data presented as n (%).
Logistic regression analysis of factors affecting prognosis of patients with pulmonary infection, admitted to a Chinese neurological intensive care unit (n = 374).

OR, odds ratio; COPD, chronic obstructive pulmonary disease.
X31 and X32 are the dummy variables of medical insurance status in logistic regression analysis, such that X31 = 0; and X32 = 0 is private expense, X31 = 0 and X32 = 1 is medical insurance, and X31 = 1 and X32 = 0 is public expense.
Prognosis and duration of stay in the neurological intensive care unit (NICU) and hospital in Chinese patients with pulmonary infection, stratified by infecting micro-organism (n = 374).
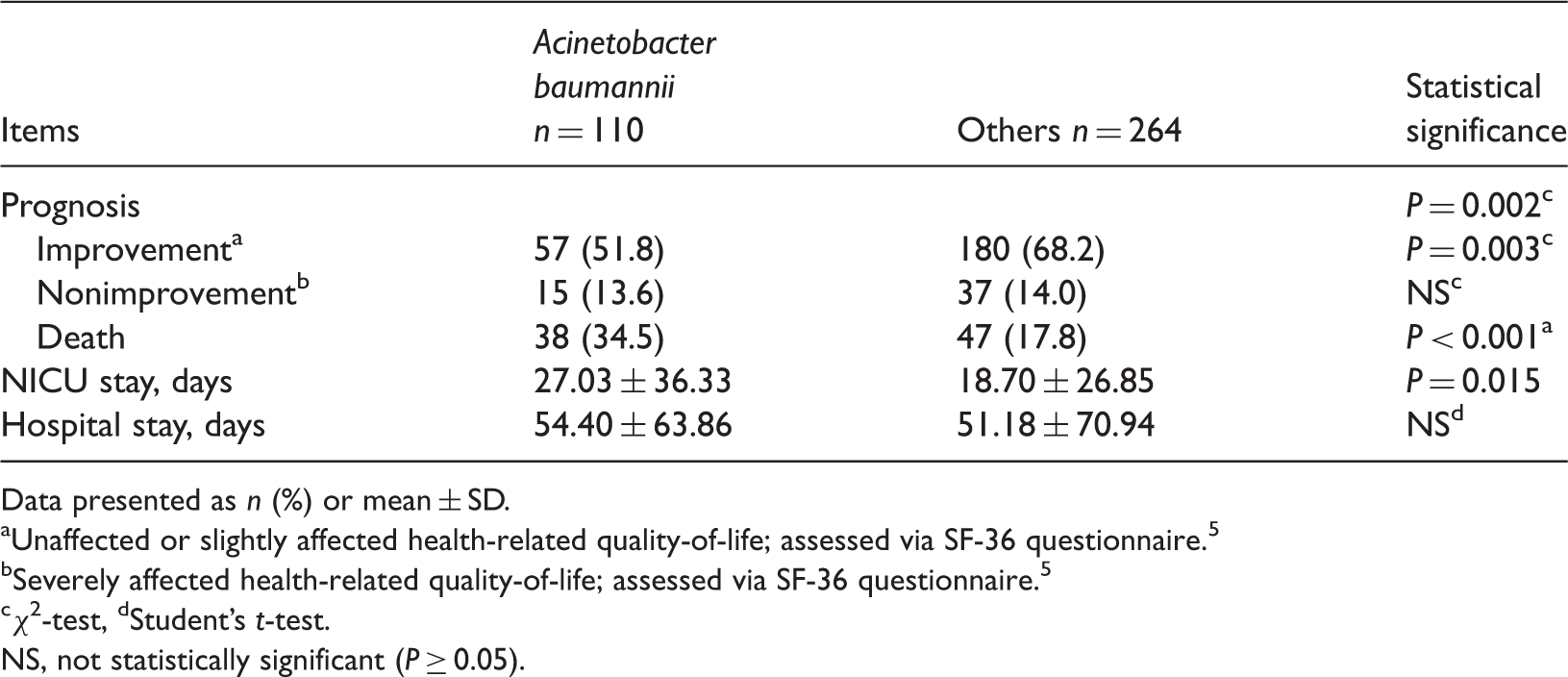
Data presented as n (%) or mean ± SD.
Unaffected or slightly affected health-related quality-of-life; assessed via SF-36 questionnaire. 5
Severely affected health-related quality-of-life; assessed via SF-36 questionnaire. 5
χ2-test, dStudent’s t-test.
NS, not statistically significant (P ≥ 0.05).
Discussion
Pulmonary infection is the most common type of infection in the NICU 1 and can aggravate the primary disease, prolong the NICU stay, increase the medical costs and threaten the life of the patient. There is a disproportionately high number of elderly patients in a typical NICU, 6 as well as patients with neurological symptoms including altered consciousness. This results in difficulty diagnosing pulmonary infection (which typically presents with cough, shortness of breath and tachycardia, low-grade fever, loss of appetite and lethargy), prolonging treatment time and negatively affecting prognosis.
The nonfermenting, Gram-negative, conditionally pathogenic bacillus A. baumannii is widely distributed in hospital environments, and has strong resistance to moisture, heat, ultraviolet rays and chemical disinfectants. 7 The A. baumannii infection rate is increasing, and was found to be the fourth most common nosocomial infection in the US 8 and China. 9 A single Chinese study found that A. baumannii accounted for 16% of infections in 2010, 9 while another indicated that A. baumannii was responsible for 12% of nosocomial pulmonary infections in 2011. 1 In the present study, A. baumannii was the pathogen in 29.4% of pulmonary infections. Taken together, these data suggest that the incidence of A. baumannii infection is increasing. Risk factors for A. baumannii infection include long-term hospitalization, ICU stay, mechanical ventilation, invasive surgery, antibiotic exposure and severe underlying disease. 10 The NICU is a primary location for receiving and treating patients with emergent and severe nervous system diseases, but the risk of infection is four- to five-fold greater in the NICU than in other wards. 11 It is therefore essential that medical staff practice reasonable antibiotic use and effectively prevent and control pulmonary infections.
In contrast to the findings of others, 10 there was no effect of A. baumannii infection on the total duration of hospitalization. This inconsistency may be related to factors including disease category, economic affordability and demands on resources that were not evaluated in the current study; these should be included in further studies. The significantly longer NICU stay associated with A. baumannii infection in the present study is most likely due to the aggravating effect of infection on the neurological condition, in accordance with the findings of others. 10
The mortality rate inpatients with A. baumannii infection was significantly higher than that of those infected with other pathogens in the present study, in agreement with others. 12 Pulmonary infection has been shown to increase mortality rates in patients with cerebrovascular disease, 13 and stroke associated pneumonia leads to disease aggravation and death in the hospital. 14 A. baumannii infection may affect disease prognosis in two ways. First, NICU patients are susceptible to nosocomial pulmonary infections because of their own critical disease, other underlying diseases or low resistance. Cerebrovascular diseases associated with pulmonary infection have been shown to impact short-term prognosis and increase neurological impairment, such that patients with pulmonary infection experience disease exacerbation, and prolonged NICU stays and rehabilitation. 15 Secondly, the prolonged NICU stay associated with A. baumannii infection in the present study may increase the risk of reinfection, which may directly affect prognosis.
Multidrug-resistant A. baumannii (MDRAB), extensively drug-resistant A. baumannii (XDRAB) and pan drug-resistant A. baumannii (PDRAB) are widespread, 16 limiting the treatment options and increasing mortality rates and medical costs. 17 In order to minimize increased A. baumannii antibiotic resistance, it is important to follow guidelines regarding the prevention and control of nosocomial infections and monitor changes in resistance and drug sensitivity.
In conclusion, A. baumannii infection prolongs the duration of stay in the NICU, increases the mortality rate and prolongs the rehabilitation time. Tracking and monitoring studies are required to control the infection effectively and to reduce mortality, in order to create guidelines for policies and regulations for the health care industry.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.