
Abstract
Background:
Understanding the time to hypertension occurrence after antiretroviral treatment (ART) initiation in people living with HIV (PLHIV) and its determinants is important for designing interventions for control.
Objective:
This study sought to estimate the median time of ART use to hypertension onset and its predictors in Nigerian PLHIV.
Design:
A retrospective longitudinal study.
Methods:
This retrospective review of 2503 normotensive adult PLHIV (⩾18 years) from 2004 to 2020 in two HIV clinics in Nigeria. Incident hypertension was based on clinical diagnosis or two consecutive blood pressure readings ⩾140/90 mmHg, taken during the 8 months of data collection. Survival event was defined as incident hypertension during follow-up or interview day for observed patients unless they were right censored. The Kaplan-Meier survival curve was used to estimate the survival probabilities of hypertension. The Cox proportional hazard model was fitted to identify predictors of hypertension at p < 0.05.
Results:
A total of 2503 PLHIV was followed up. The majority were females (74.6%) and on Dolutegravir-based therapy (93.0%). About 22 (0.9%) were diabetic. Median age at ART initiation was 35 (interquartile range: 29–41) years. The median period of follow-up was 12.0 ± 3.9 years. The cumulative incidence of hypertension was 32.5% (381/2540), with an incidence rate of 40.1/1000 person-years. The median time to incident hypertension was 17.0 years (95% CI: 12.5–21.5 years). Shorter hypertension-free survival times were seen in males, those aged 60+, with diabetes, unsuppressed viral load, history of tuberculosis, other opportunistic infections, or co-trimoxazole use. Significant risk factors included male sex (adjusted odds ratio (AOR) = 1.3, 95% CI = 1.1–1.6), middle age (AOR = 2.3, 95% CI = 1.7–3.2), old age (AOR = 5.6, 95% CI = 3.9–8.4), and unsuppressed viral load (AOR = 1.9, 95% CI = 1.3–2.7).
Conclusion:
Hypertension is commoner among PLHIV with unsuppressed viral load, males, and persons older than 40 years. Effective ART with viral suppression remains essential. Incorporating regular hypertension screening and treatment into HIV care is necessary for optimum health outcomes.
Introduction
Globally, there has been an improvement in the quality of life for people living with HIV (PLHIV), with a reduction in HIV-related mortality since 2004. 1 This was attributed to the introduction of a test and treat strategy in HIV care that ensures that all newly identified HIV-positive clients are initiated on HIV drugs and the advancement in HIV therapeutics.2–4 The consequence of this paradigm shift in HIV care was an improvement in the life expectancy of PLHIV, thereby prolonging their period of stay on highly active antiretroviral therapy. 5 A cohort study in the United States comparing life expectancy among PLHIV and non-PLHIV showed a steadily increasing life expectancy for people with HIV between the years 2000 and 2016. 6 At the end of the study in the year 2016, the life expectancy among non-PLHIV, and PLHIV with a CD4 count of 500 and above, was observed to be the same. However, there was an early onset of comorbidities in PLHIV compared to non-PLHIV. The onset of diabetes, cancer, and cardiovascular diseases occurred 8 to 9 years earlier for PLHIV compared to non-PLHIV. 6
Nigeria has the second largest population of PLHIV in the world, with an estimated number of 1.9 million persons living with HIV in 2020. 7 Following the Nigeria national household survey in 2018 that showed that only about half of the PLHIV in the country were on antiretroviral treatment (ART), the country launched an aggressive antiretroviral therapy surge that doubled the number of PLHIV on drugs. 8 This effort, coupled with the roll-out of highly potent and efficacious Dolutegravir-based therapy, gradually shifted the HIV program focus in Nigeria from HIV epidemic control to multi-disease surveillance (including hypertension) for HIV-positive clients who now live for a prolonged period on antiretroviral therapy.
In Nigeria, there is a dearth of literature on the median survival time for the development of hypertension from antiretroviral drug initiation among PLHIV. Most studies in Nigeria focused on the prevalence of hypertension among PLHIV by conducting a review of records or cross-sectional studies.9–11 However, few studies in Africa that reported a median time to develop hypertension had varied estimates depending on the categories of the study population.12,13 In a 1-year multicenter prospective follow-up study done in Northwest Ethiopia among newly identified PLHIV initiated on antiretroviral drugs, the median time to hypertension development was observed to be 7 months with an interquartile range (IQR) of 5.00–9.00 months, with 13.4% of participants being diagnosed of hypertension within the 1 year of follow-up. 12 A similar study in South Africa reported a median time to develop hypertension in the 5–10 years range for different covariates. 13
Previous studies showed a significantly higher cumulative probability of developing hypertension over time among male patients, patients whose age is ⩾40 years, patients with body mass index (BMI) >25 kg/m2, and patients with diabetes mellitus compared to their counterparts. The most identified risk factors for early hypertension occurrence among PLHIV were male gender and high BMI.12–16 Across studies, males living with HIV were two to three times more likely to develop hypertension compared to the female gender. Also, PLHIVs with higher BMI ⩾ 25 kg/m2 were two to six times more likely to develop hypertension than the others. Other documented risk factors were low CD4 count, severe CD4 count, patient current ART regimen, old age, high viral load, antiretroviral therapy use and presence of diabetes comorbidity, high glomerular filtration rate, and family history of hypertension.12–16
The understanding of the median duration to the onset of comorbidities occurrence from the period of antiretroviral initiation and the associated factors is vital for designing monitoring and surveillance interventions for noncommunicable diseases among PLHIV and also for shaping comorbid therapeutics in PLHIV. This study sought to estimate the median time to hypertension development from the date of antiretroviral drug initiation among PLHIV and assess risk factors for hypertension development in the population. This is essential as Nigeria strives to achieve treatment saturation and epidemic control and intensify efforts in noncommunicable disease surveillance and service integration. This will help to improve the quality of life among aging PLHIV in the country.
Methodology
Study design
A retrospective longitudinal study of 2503 normotensive adult PLHIV (⩾18 years) enrolled in HIV care between 2004 and 2020 in two HIV clinics in Northern and Southern Nigeria, to assess the occurrence of incident hypertension on or before November 2022.
Research setting
The study was conducted in Adeoyo Maternity Hospital, Ibadan, Oyo State, Nigeria, and Our Lady of Apostle (OLA) Hospital, Jos, Plateau State, Nigeria. The two clinics are part of the APIN Public Health Initiatives-supported facilities for Improved HIV service delivery under the Centers for Disease Control iCARES grant in Nigeria. Adeoyo Maternity Hospital is a public secondary health facility, while OLA hospital is a private health facility. The facilities serve as referral centers for the provision of secondary care for most primary health facilities in their senatorial districts. The hospitals provide pediatric and adult outpatient and inpatient care, gynecology and obstetrics services, emergency care, general and specialized surgical care, and have specialized clinics for providing ART services for PLHIV. Their HIV clinics provide ART services to pediatric, nonpregnant adult clients and Prevention of Mother to Child Transmision of HIV (PMTCT) services to pregnant ART clients. They have different sub-units including the adherence counseling unit, consulting rooms, records, phlebotomy unit, patient waiting room, ART dispensary units, and data room for electronic medical record (EMR) operations. They open every weekday and run block appointments for the cohort of patients with similar attributes. In both clinics, noncommunicable disease management, including hypertension, has not been integrated into ART care. However, blood pressure measurements are occasionally done at the nursing station using an analog sphygmomanometer, and identified patients with suspected high blood pressure are referred to the outpatient or general medical clinics for treatment and follow-up. Furthermore, there is incomplete documentation of blood pressure measurements in the EMRs of both clinics, although a majority of the patients had baseline blood pressure measurements at ART initiation.
Oyo State, where Adeoyo Maternity Hospital is located is situated in the South-Western region of the country. According to the 2006 National Census, the State has a population of 5,580,894 with a population projection of 7,976,100 by the end of the year 2021. 17 The prevalence of HIV in the State was 0.9%, 18 while hypertension prevalence ranges between 33% and 39% among adults.19,20 Similarly, OLA hospital is situated in Plateau state, one of the North Central states with a population of 3,206,531 according to the 2006 census and a projected population of 4,717,300 by the end of 2021. 21 According to the Nigeria Indicator and Impact Survey 2018, the prevalence of HIV in Plateau State is 1.5% 18 while the prevalence of hypertension in the state ranges from about 22.2%–32% for adults.22,23
Study participants recruitment
Study participants were adult PLHIV, 18 years and above, who were enrolled in HIV care between 2004 and 2020 and were normotensive (Blood pressure (BP) measurements of <140/90 mmHg) at ART enrollment. Patients who were acutely ill, frail, or patients diagnosed with hypertension during the study period but whose hypertension diagnosis or care history could not be confirmed or cross-referenced, were excluded from the study.
Data collection was collected over a period of 8 months. We line-listed eligible participants from the electronic monitoring records of the ART clinics of both hospitals and booked appointments with them for physical interviews and measurement of blood pressure. On the interview day, verbal reports of previous hypertension diagnoses were elicited. Patients who confirmed previous diagnoses were followed up at the clinics where they are receiving hypertension care for records cross-referencing, provided the clinic is within the hospital premises or within a 5 km radius of the study site. Patients who were receiving hypertension care in hospitals outside a 5 km radius were also included, provided they had home-based cards or exercise books for cross-referencing their verbal reports. Furthermore, we also did two consecutive measurements of blood pressure of each patient interviewed, for us to identify previously un-diagnosed hypertension, and those who had blood pressure ⩾140/90 mmHg at the first measurement, had repeated blood pressure during the 8 months of data collection.
Study instrument and variables, and data collection procedure
The study was conducted using a project-developed electronic questionnaire that elicited information on patient demographic characteristics, HIV care history, verbal reports of previous diagnosis of hypertension or diabetes, and also used to extract records of hypertension and diabetes care from the clinics where the patient received care. The electronic tool was developed using a kobo-collect application ensuring end-to-end encryption of transmitted data. BP was assessed with the aid of an Accoson mercury sphygmomanometer (https://www.accoson.com/) while the patient was in a relaxed state. The systolic and diastolic BP values were determined using the initial and fifth Korotkoff sounds, respectively. Two consecutive measurements were taken for each patient, using both the arms of the patient. Reading from the arm with higher BP was used for hypertension diagnosis. The measurements were done by recruited nurses in the facilities, who had demonstration training on appropriate ways of measuring BP. Data collection in both facilities was done by project-recruited data entry clerks (DECs), one per facility. A day of training was organized for the DECs on the study tools, techniques, and procedures.
Incident hypertension in this study was defined as confirmed clinically diagnosed hypertension during the study period (2004–2020), or identified two consecutive BP measurements of ⩾140/90 mmHg done during clinic visits within the 8 months of data collection (JNC 7 classification). Exploratory variables assessed included respondent’s demographic such as age and sex, HIV care history, and hypertension care history. Patient HIV viral count (VL) was classified into suppressed (VL < 20 copies/ml), low-level viremia (VL, 20–999 copies/ml), and unsuppressed (VL ⩾ 1000 copies/ml). Furthermore, respondents’ age was classified into young age, <40 years, middle age, 40–60 years, and old age, >60 years.
Data management and analysis
Data was collected by research assistants under the supervision of site co-investigators using questionnaire forms that elicited information on participants’ backgrounds, clinical history, and Non-Communicable Diseases (NCD) occurrence. The research assistants also conducted verbal interviews and record reviews of HIV and chronic disease clinic records. End-to-end encryption was done to secure electronic data during transmission. Data cleaning and analysis were done using Statistical Package for Social Sciences (SPSS) IBM version 23. Descriptive findings were presented using charts and tables. Survival event was defined as the occurrence of incident hypertension during the follow-up period or interview day, which was observed for all patients except they were right censored. The Kaplan-Meier survival curve was used to estimate the population’s median hypertension-free survival time. Factors associated with median hypertension-free survival time were assessed at a bivariate and multivariate level using log-rank statistical test and Cox proportional regression analysis at p less than 0.05. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 24
Ethical consideration
Informed consent was obtained from all patients who participated in the study, evidenced by signed consent forms. Ethical approval for the study was from the Nigeria Health Research and Ethics Committee (NHREC) on January 11, 2022 with the ethical approval number of NHREC/01/01/2007-18/01/2022 and renewed on January 23, 2023 with ethical approval number NHREC/01/01/2007-27/01/2023B. In addition, the study complied with the Declaration of Helsinki on conducting research among human subjects.
Results
A total number of 2503 participants were followed up. Median age and CD4 count at ART initiation were 35 (IQR: 29–41) years and 251 (134.0–406.5) cells/ml. (Table 1). Most were female, 1868 (74.6%), and on Dolutegravir (DTG)-based antiretroviral therapy, 2372 (93.0%). About half (52.1%) of the participants had unsuppressed viral load at their first-ever viral load testing closest to the ART initiation time. About 22 were diabetic (0.9%). The median period of follow-up was 12.0 ± 3.9 years. The cumulative incidence of hypertension over the follow-up period was 32.5% (381/2540), with an incidence rate of 40.1/1000 person-year (Table 2). The incident hypertension-free survival time (median duration of ART use to hypertension incident) was 17.0 years (95% CI: 12.5–21.5 years) (Figures 1 and 2).
Patients’ background characteristics.

Others include EFV- and AZT-based ARV.
Bold is just to signify the significant estimates p<0.05
ART, antiretroviral therapy; ARV, Antiretroviral drugs; AZT, Zidovudine; EFV, Efavirenz.
Cumulative incidence and incidence rate of hypertension.


Kaplan-Meier plot comparing median survival time in male and female participants.

Median duration of antiretroviral therapy use to occurrence of clinically diagnosed hypertension.
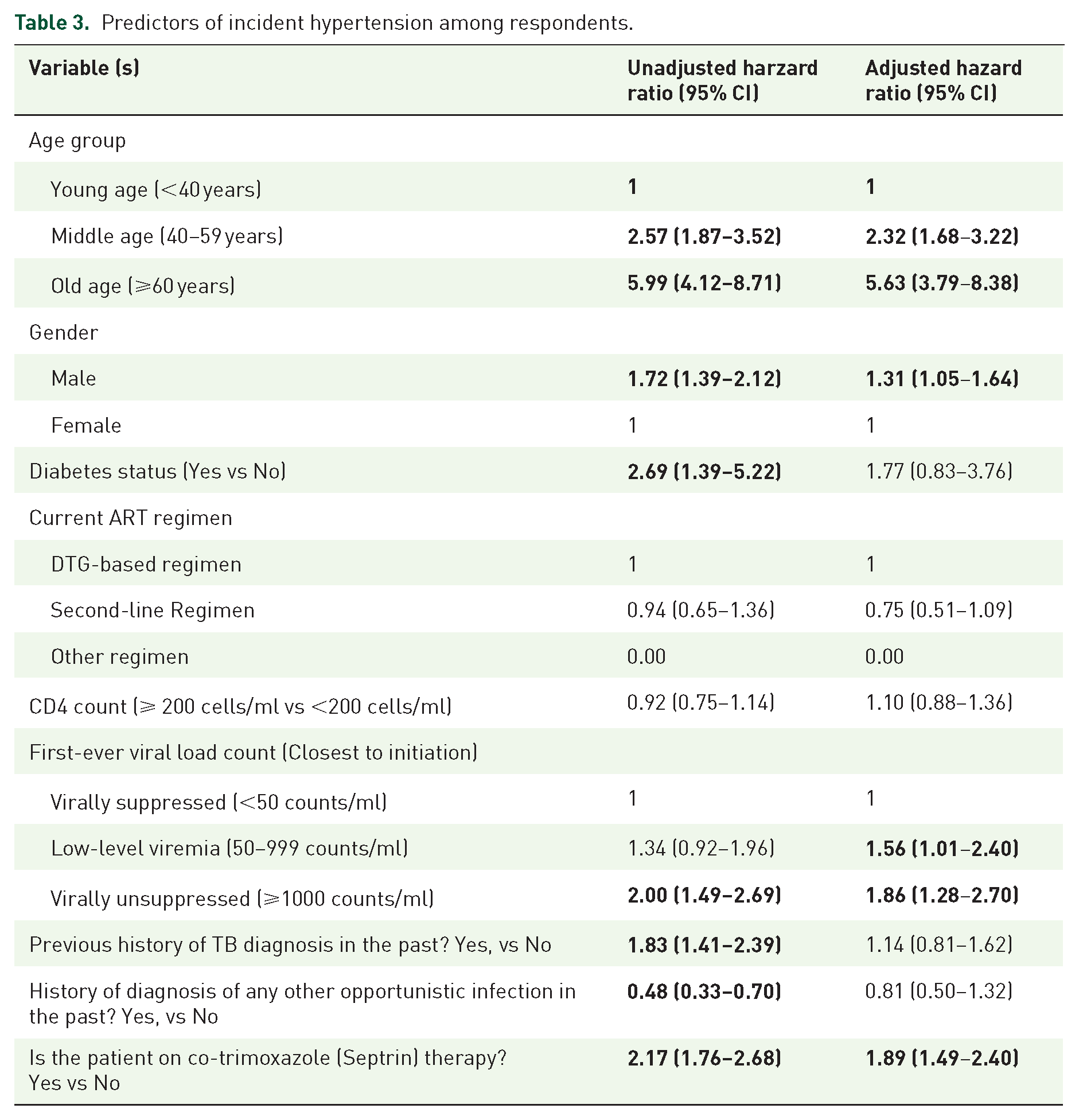
The hypertension-free survival times were shorter in males (12.4 years), old age participants (10.9 years), participants with diabetes mellitus (10.7 years), virally unsuppressed participants (13.5 years), those with a previous history of tuberculosis (11.3 years), with other opportunistic infection (10.1 years) or participants on co-trimoxazole, compared to their counterparts who were female (15.9 years) (p < 0.01), young (15.1 years) and middle age (15.4 years) (p < 0.01), without diabetes mellitus (15.5 years) (p = 0.02), those with viral suppression (15.2 years) and low HIV viremia (15.9 years) (p < 0.01), those without history of TB (15.7 years) (p < 0.01), without on other opportunistic infection (15.6 years) (p < 0.01) or not on co-trimoxazole (16.1 years) (p < 0.01), respectively (Table 1). Factors associated with incident hypertension at a univariate level were male sex (Crude Hazard Ratio (CHR) = 1.7, 95% Cl = 1.4–2.1), middle age (CHR = 2.6, 95% Cl = 1.9–3.5) and old age (CHR = 6.0, 95% Cl = 4.1–8.7), unsuppressed viral load (CHR = 2.00, 95% Cl = 1.5–2.7), presence of diabetes mellitus, (CHR = 2.7, 95% CI = 1.4–5.2), previous history of TB (CHR = 1.8, 95% CI = 1.4–2.4), and use of co-trimoxazole therapy, (CHR = 2.2, 95% Cl = 1.8–2.7). Only male sex (adjusted Hazard ratio (AHR) = 1.3, 95% CI = 1.1–1.6), middle age (AHR = 2.3, 95% CI = 1.7–3.2), old age (AHR = 5.6, 95% CI = 3.8–8.4), and unsuppressed viral load (AHR = 1.9, 95% CI = 1.3–2.7) were found to be significant after adjusting for covariates (Table 3).
Predictors of incident hypertension among respondents.
Discussion
This study aimed to assess the incidence of hypertension and its associated factors among PLHIV. Our study observed a higher incidence rate of hypertension among PLHIV compared to figures reported in previous studies. Specifically, we found an incidence rate of 40.1 per 1000 person-year, which surpasses the rates reported by Mulugeta et al. 12 in Ethiopia (16.35 per 1000 months or 0.02 per person-year), Okello et al. 25 and Byonanebye 26 in Uganda (111.5 per 1000 person-years or 0.1 per person-year, and 24.8 per 1000 person-years or 0.025 per person-year, respectively). Additionally, a study conducted in Ghana reported an incidence rate of 320.1 per 1000 or 0.3 per person-year among PLHIV receiving ART care at a tertiary health facility. 27 One possible explanation for the higher incidence rate observed in our study is the longer duration of follow-up, which had a duration span of 17 years. In contrast, many previous studies had comparatively shorter follow-up periods ranging from 1 to 10 years.
Furthermore, it has been well-documented that PLHIV in Nigeria may have a higher prevalence of risk factors for cardiovascular disease. 28 For instance, the cumulative incidence of hypertension (32.5%) that we observed in our study closely aligns with the reported incidence of 31% among a cohort of PLHIV in northern Nigeria. 9 This underscores the elevated risk of hypertension among PLHIV in Nigeria and highlights the importance of screening for cardiovascular diseases in this population.
In our study, males were more likely to develop hypertension when compared to females. This appears to be a common trend among PLHIV as demonstrated in the past literature. For instance, Tsuro et al. 13 and Brennan et al. 15 in separate studies of PLHIV in South Africa, demonstrated a higher risk of hypertension among males. Similar findings were reported among PLHIV in Ethiopia 29 and in a multi-country study encompassing 11 cohorts of PLHIV in Europe, Australia, and the USA. 30 Only a few studies reported higher risks of hypertension among females.12,16 There are some potential reasons for the higher burden of hypertension among male PLHIV. One explanation could be the protective effect of estrogen on women, although this declines with age. 23 Also, men may be more prone to engaging in lifestyle factors that predispose them to hypertension, such as a sedentary lifestyle, smoking, and excessive alcohol use. 12 Additionally, innate biological differences between males and females especially in genetics and body composition may put men at higher risk of hypertension. 31
In our study, older PLHIV (>40 years) have a significantly higher risk of developing hypertension and this seems to be a common observation from past studies.15,26,27,29 The risk of hypertension doubled for those older than 60 years as compared with those aged 40–59 years. This increased risk may be due to multiple factors associated with aging and the interaction with HIV infection. A plausible reason for the increased risk among older PLHIV is the age-related reduction in arterial distension and a marked increase in atherosclerosis. Furthermore, some age-related comorbidities may be present and predispose older PLHIV to hypertension, such as diabetes mellitus, kidney diseases, and dyslipidemia.32,33 Also, the persistent immune activation and chronic inflammation associated with HIV infection have huge implications for cardiovascular health and these effects are more prominent with increasing age. 34 We reported that patients with low-level viremia and unsuppressed viral load were more likely to develop hypertension, suggesting that ongoing HIV replication may be a significant contributor to hypertension risk. 29 The type of ART regimen was not a significant predictor of incident hypertension among our study participants. Of note is that the majority of the participants in this study are currently on a dolutegravir-based regimen. The interaction between HIV infection, aging, gender, immune activation, and chronic inflammation creates a complex landscape for cardiovascular health among PLHIV. Therefore, further research with larger sample sizes and more robust study designs is needed to examine the effect of ART on incident hypertension among PLHIV in Nigeria.
This study stands out as one of the first to document such findings within a relatively large cohort of PLHIV attending ART clinics in both southern and northern regions of Nigeria, observed over a long period of time for the incidence of hypertension. Our study had certain limitations, including the absence of data for important variables such as BMI, family history, smoking and alcohol intake, and physical activity status. These variables have been recognized as potential influential factors in the development of hypertension among PLHIV. Future research endeavors should consider incorporating these variables to gain a more comprehensive understanding of the factors contributing to hypertension in this population. Furthermore, the study did not examine the association between ARV use and incident hypertension.
Conclusion
Our study reported a high incidence of hypertension among PLHIV with early occurrence of hypertension among males, older age, HIV virally unsuppressed participants, and participants with diabetes mellitus. There is a need to scale up hypertension control interventions among PLHIV to combat the high incidence of hypertension in the sub-population, with prevention activities tailored toward the identified risk factors for the early occurrence. Effective management of hypertension among PLHIV requires the integration of ART services with the control of noncommunicable diseases such as hypertension, diabetes mellitus, and cancers. By integrating these services, healthcare providers can deliver comprehensive care that addresses the unique needs and challenges faced by PLHIV. This integrated approach will not only have significant health benefits for PLHIV but also improve the overall effectiveness and efficiency of health service delivery, especially in resource-limited settings.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241289800 – Supplemental material for Time to incident hypertension and independent predictors among people living with HIV in Nigeria
Supplemental material, sj-docx-1-tai-10.1177_20499361241289800 for Time to incident hypertension and independent predictors among people living with HIV in Nigeria by Oluseye Ayodele Ajayi, Prosper Okonkwo, Temitope Olumuyiwa Ojo, Oluwaseun Kikelomo Ajayi, Olabanjo Ogunsola, Emmanuel Osayi, Ifeyinwa Onwuatuelo and Jay Osi Samuels in Therapeutic Advances in Infectious Disease
Footnotes
Appendix
Acknowledgements
The authors would like to thank our ART staff at all the sites used for this study for their cooperation and dedication in providing the study data. We would also like to acknowledge the National Institute of Health, Fogarty International Center (NIH-FIC), Emory Nigeria—Research Training Program (EN-RTP D43TW010934-05) who provided support to the first author.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.