
Abstract
Objectives:
This study sought to assess the current impact of health insurance coverage on medication adherence and blood pressure control of patients being managed for hypertension in Ghana and Nigeria.
Methods:
The study was a prospective study among 109 patients with hypertension in two health facilities with similar population dynamics in Ghana and Nigeria. Patients were systematically selected, categorized as having health insurance coverage or not, and followed up monthly for 6 months. The outcome variables (medication adherence and blood pressure control) were then measured and compared at 6 months. Analysis was done using Stata with level of significance set at p ⩽ 0.05.
Results:
There was a 90% insurance coverage among participants from Ghana compared to 15% from Nigeria. National Health Insurance Authority enrolees in both countries had better blood pressure control and medication adherence compared to non-enrolees (adjusted odds ratio = 2.6 and 4.5, respectively).
Conclusion:
National Health Insurance Authority enrolment was found to be poor among respondents in Nigeria compared to Ghana. Enrolment into the National health financing schemes in both countries led to better blood pressure control and medication adherence among patients with hypertension at primary health facilities. There is therefore the need for system strengthening to improve their sustainability.
Introduction
Health financing through health insurance is a major way to achieve universal health coverage by reducing catastrophic health expenditure arising from out-of-pocket cost for healthcare. 1 The National Health Insurance Authority (NHIA), previously known as the National Health Insurance Scheme (NHIS), became fully operational in 2005 and 2008 for Nigeria and Ghana, respectively. Over the years, efforts have been made to increase coverage which has however remained low with about 5% coverage in Nigeria.2–4 In Ghana, however, health insurance coverage (either NHIA or private scheme) is currently about 68.6%, being as high as 86.2% in one region.1,5 Health insurance has been adopted by most countries of the world as a preferred payment option for healthcare services.1,2,6 Majority of Africans still do out-of-pocket payment for health services, a situation that has worsened the burden of noncommunicable diseases including hypertension, consequently increasing mortality and disability.2,7
Hypertension is a major public health issue affecting about a quarter to half of the African population.8–11 Blood pressure control in patients with hypertension is important as it significantly reduces the risk of cardiovascular events such as stroke, coronary artery disease and premature death.12,13 However, rate of blood pressure control remains dismally poor with over half of patients with hypertension not having their blood pressure controlled.9,11,14
A major setback in the management of hypertension is poor medication adherence.8,11,12,14 Up to 70% of patients with hypertension are not consistent with medications. 11 A major reason for poor medication adherence is lack of money to purchase medications.9,10,13 A study in Indonesia found a significant association between low socioeconomic status and medication adherence among patients with hypertension, as a good number of patients stop their medications because they could not afford them. 15 Other studies in Nigeria, Ghana and Tanzania also highlighted the role of poverty in patients’ adherence to medications and blood pressure control.16–18 Patients might then typically resort to alternative medicines, self-prescriptions or outright stoppage of the medications.8,9,14
NHIA, therefore, to a large extent should provide acceptable cover and reduce the problem of poor BP control from poor medication adherence due to the direct cost of drugs. Whether NHIA has been able to bring about increase in medication adherence and improvement in blood pressure control in Nigeria and Ghana has not been ascertained. In this study, we conducted a pilot study to evaluate the impact of NHIA on medication adherence and blood pressure control in Nigeria and Ghana after over 14 years of the introduction of the scheme in both countries.
Method
This was a prospective study conducted in Nigeria and Ghana as part of a preliminary study on patients with hypertension in both countries. The study was conducted from May 2021 to December 2021. Ethical approval for the study was granted by the Ethics Review Committees of FTH, Ido Ekiti, Nigeria (ERC/2020-06/15/377A) and Ghana Health Service (GHS) Ethical Review Committee (GHS-ERC 007/10/20).
The Federal Teaching Hospital, Ido-Ekiti, Nigeria and Adabraka Polyclinic, Accra, Ghana were used for the study. Both health facilities were determined to have similar institution and patient characteristics. Adult patients aged 18 years and older with hypertension visiting the outpatient department (OPD) of both facilities who consented to participate were consecutively recruited and followed up monthly for 6 months. Patients with secondary hypertension or other comorbidities, those with cognitive impairment those severely ill or weak whose condition, will not allow them to be interviewed as well as those lost to follow up and could not complete the study were excluded.
The sample size was calculated to be 39% at a confidence level of 95% using the single sample for infinite population formula: Ss = (z2 × σ2)/d2,19 where Z = Z value (e.g. 1.96 for 95% confidence level); σ = Standard Deviation; d = distance on either side of mean in confidence interval using the standard deviation of 0.95 ± 0.16 from Sarfo et al. 20 and assuming d of 0.05. Assuming an attrition rate of 10% (which approximates to 4), the minimum sample size was calculated to give 43, bringing the total number of participants to 86 in each country. Data was collected from 109 participants made up of 59 from Nigeria and 50 from Ghana. This was done to increase the power of the study.
Variables for this study included health insurance status, sex, age, educational level and occupation, and the outcome measure being blood pressure control and medication adherence.
Blood pressure was taken thrice 10 min apart and the mean of the last two readings was determined. Participants with blood pressure <140/90 mmHg were classified as controlled while those with BP ⩾ 140/90 mmHg were classified as uncontrolled.15,21,22
Medication adherence was assessed using the Hill Bone Scale which has been validated for use in blacks.23,24 The 9-item medication subscale of the 14-item tool was used to assess for medication adherence in the respondents. Individual responses were scored on a Likert scale of 1 to 4, 1 indicating best compliance and 4 worst compliance, and the scores summed up. Respondents with scores greater than 18 were considered non-adherent and those with scores less than 18 were considered adherent.8,23 Participants were assessed at baseline and 6 months and outcome variables taken on both occasions.
Statistical analysis
Statistical analysis was done using Stata (16.1; StataCorp LLC, College Station, TX, USA). Variables were described and compared with the outcome measures using a chi square test, with the application of the Fisher’s exact test. Logistic regression analyses were also done with controlled BP and medication adherence as outcome measures of interests. Analyses were done assuming a 95% confidence and alpha level of 0.05 considered significant.
Results
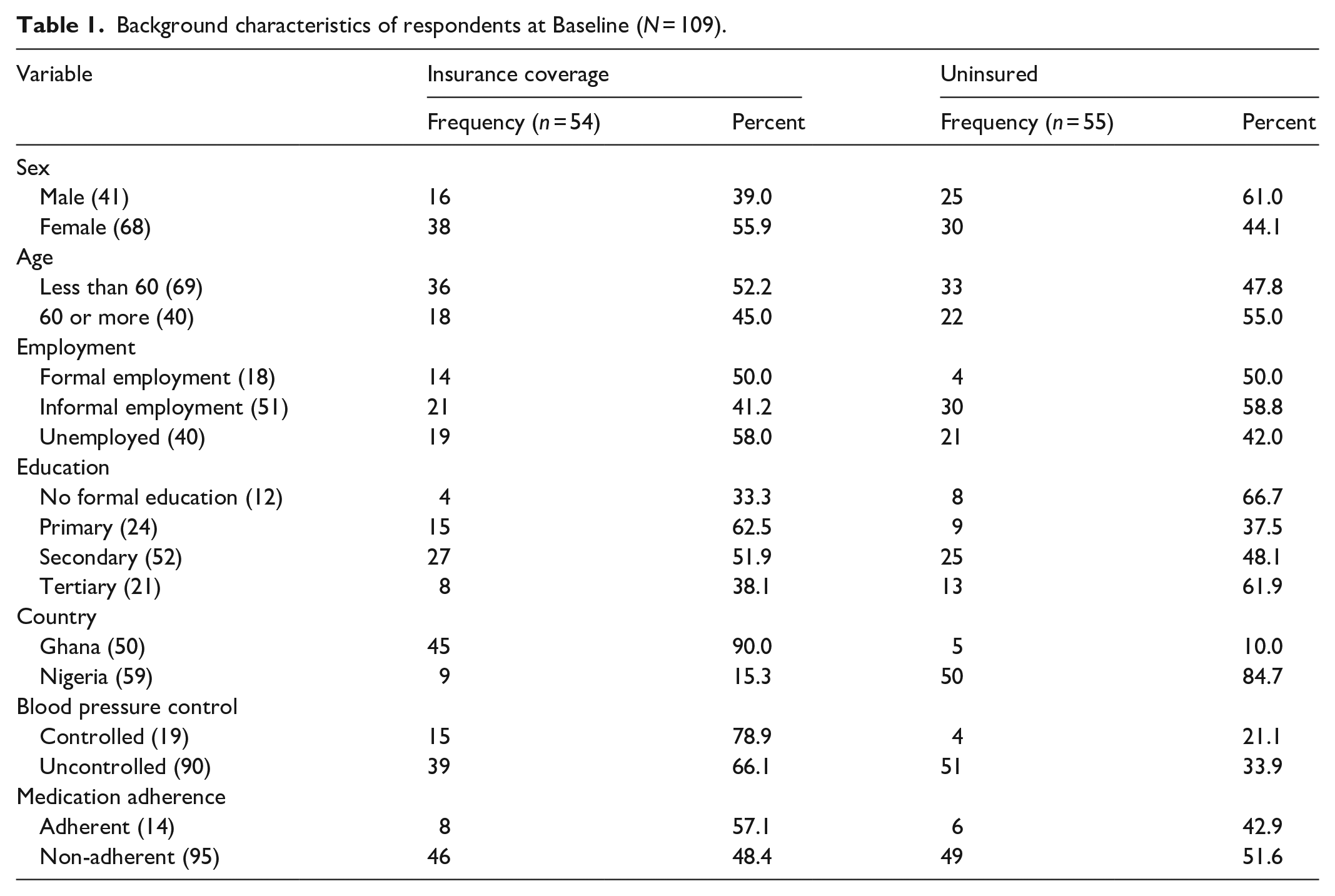
There was a total of 112 potentially eligible participants, 60 from Nigeria and 52 from Ghana, who were screened and recruited having met the eligibility criteria and consented to the study. However, three patients were lost to follow up; one in Nigeria due to change in location and two in Ghana due to death and change in location, respectively. The remaining 109 participants completed this pilot study over the 6-month period and their results were analysed. They were made up of 59 participants from Nigeria and 50 from Ghana. These included 41 males and 68 females. There was a higher level of insurance coverage among Ghanaian participants (p < 0.001), with 90% coverage, compared to 15% in Nigeria (Table 1). Health insurance coverage did not differ significantly among sex (p = 0.114), age category (p = 0.470), employment category (p = 0.239) and education levels (0.525).
Background characteristics of respondents at Baseline (N = 109).
After 6 months from commencement of study, the blood pressure and medication adherence were again taken and are shown in Figure 1. The total patients with blood pressure control has increased from 19 to 27 with 66.7% of respondents with good BP control having health insurance cover. Those with medication adherence also increased from 14 to 74 with 57.1% of them having health insurance.

Blood pressure control and medication adherence at 6 months (N = 109).
At the end of the study, being an NHIA enrolee (p = 0.040), female sex (p = 0.018) and being in Ghana (p = 0.003) were found to be significantly associated with good BP controlled (Table 2)
Effect of health insurance and background characteristics on BP control (N = 109).

NHIA: National health insurance authority; BP: blood pressure.
Statistically significant.
There was also an association between medication adherence and NHIA enrolment (p = 0.001), male sex (p = 0.029), and being resident in Ghana (p < 0.001) as shown in Table 3.
Effect of health insurance and background characteristics on medication adherence (N = 109).

NHIA: National health insurance authority.
Statistically significant
When subjected to logistic regression, it was found that for the entire population, participants with health insurance coverage were 2.6 times more likely to have controlled blood pressures at the end of the study than patients without insurance coverage. This association was found to be statistically significant (p = 0.044). Within individual countries however, there was no observable significant relationship between health insurance coverage and BP control at the end of the study (pGhana = 0.300, pNigeria = 0.417).
As shown in Table 4, aside health insurance coverage, sex (p = 0.018) and country (p = 0.003) showed significant associations with the blood pressure control of participants. With respect to sex, though the pooled study population showed a significant association, none was observed on country sub-analyses (pGhana = 0.395, pNigeria = 0.072).
Logistic regression of effect of health insurance and background characteristics on BP control & medication adherence (N = 109).

CI: Confidence interval.
Statistically significant.
At the end of the study (6 months), the odds of health insurance beneficiaries having adequate medication adherence was 4.5 times the odds of non-insurance beneficiaries. This association, for the entire population was found to be statistically significant (Table 4). The relationship at country analyses was however not significant (pGhana = 0.513, pNigeria = 0.457). Furthermore, though sex influenced medication adherence for the entire population, observation at sub-population level was different (pGhana = 0.112, pNigeria = 0.616).
Discussion
We set out in this study to get a current perspective of the effect of NHIA on individual management outcomes, here being blood pressure control and medication adherence. It was found that overall, participants with health insurance coverage, at the end of the study, were more likely to have controlled blood pressures and medication adherence than patients without insurance coverage (AOR = 2.6 and 4.5, respectively). The study also found the Ghanaian arm to have significantly more NHIA enrolees compared to Nigeria. This is similar to the national NHIA coverage of both countries which is currently 68% and 5% for Ghana and Nigeria, respectively.1,2,25,26 The wide difference in coverage is disturbing considering the fact that both countries started the scheme about the same time, funding in both countries is from government capitation, premium from enrolees, contributory payment by formal sector employees and voluntary contribution by other citizens who are not employed in the formal sector.1,2
Enrolees are also similar in both countries and include formal sector employees, voluntary enrolees. However, Ghana, unlike Nigeria, includes all children less than 18 years and elderly persons greater than 70 years.1,2 Also, majority of enrolees in Nigeria are those in the formal sector. There is also paucity of funds to run the scheme as it is currently being funded by capitation from government. 2 The enrolees through their unions have refused to make their contributory payment which was the original design of the scheme. 2 This, coupled with the voluntary nature of the scheme is mainly due to lack of confidence in the system by the populace which is further heightened by a perceived low quality of care by healthcare providers, use of intermediaries in the form of Health Maintenance Organizations (HMOs), lack of commitment on the part of government who access healthcare mostly outside the country and massive corruption among the major stakeholders from the regulators, the HMOs, the service providers and even the enrollees.2,8
Respondents with NHIA coverage had better blood pressure control compared to those without NHIA coverage. This is similar to findings of a similar study in Southern Nigeria that found better blood pressure control among patients with NHIA coverage. 8 A study conducted in China also found a positive association between health insurance coverage and blood pressure control. 27 This may be due to the fact that NHIA coverage means patient is not limited by funds, thus access to standard healthcare including medications does not depend on patents’ ability to pay as opposed to out of pocket spending where patients are limited by their capacity to pay for healthcare and medications. Also, respondents from Ghana had better blood pressure control compared to those from Nigeria. This may be attributed to the greater NHIS coverage in Ghana compared to Nigeria.
NHIA enrolees also had better medication adherence compared to non-enrolees. This could be due to the fact that they had access to their medications as the cost of antihypertensive medications are covered under the scheme compared to non-enrolees who had to procure their medications from out of pocket spending. Considering the lower economic status of both countries, being able to procure medications competes with expenditures like food, shelter and education and in the face of low income. A study conducted in Ekiti, southwestern Nigeria which was one of the sites for our study showed that most patients with hypertension spend a third of their monthly income on blood pressure medications. 14 This is huge and unsustainable. Low income was also found to be associated with poor medication adherence among hypertensive patients in Indonesia and Panam.15,28 Non medication adherence leads to increased morbidity and mortality and poor outcome. Efforts should therefore be made to increase medication adherence by increasing accessibility to medications. This can be achieved through improved NHIA coverage. Surprisingly, countries like Indonesia that started their national health insurance 9 years after Nigeria (2014) currently have 82% coverage. 6 Therefore, achieving a greater NHIA coverage is achievable, the nation just need to look in the right direction. It is hoped that the new National Health Insurance Authority (NHIA) act which was passed recently would help achieve this. 16
Limitations and strengths
The study considered patients who were enrolled on NHIA as having NHIA coverage whereas some of them particularly the wealthy ones may be paying out of pocket. The Nigerian study was done in a major town in Ekiti State, South West Nigeria while the Ghanaian study was done in Accra, the country’s capital. This may have accounted for the very high coverage in Ghana (90%) which is far above the national coverage of about 68.6%.
The strength of this study lies in the fact that it is a prospective study. Most studies on NHIS coverage in the region were cross-sectional.
This study is clinically relevant as it will help clinicians and policy makers appreciate the role of NHIA in the management of chronic diseases including hypertension and step up advocacy for wider coverage particularly in the non-formal sector.
Conclusion
NHIS enrolment was found to be poor among respondents in Nigeria compared to Ghana. However, respondents with NHIS coverage had better medication adherence and blood pressure control. There is therefore the need to put measures in place to increase NHIS coverage in sub-Saharan Africa as it offers a major channel to reduce hypertension and its attendant sequelae among its population.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231152324 – Supplemental material for Medication adherence and blood pressure control: A preliminary assessment of the role of health insurance in Nigeria and Ghana
Supplemental material, sj-docx-1-smo-10.1177_20503121231152324 for Medication adherence and blood pressure control: A preliminary assessment of the role of health insurance in Nigeria and Ghana by Tijani Idris Ahmad Oseni, Paa-Kwesi Blankson, Bolade Folasade Dele-Ojo, Fiifi Duodu, Chidiebere Peter Echieh, Sulyman Biodun Alabi, Bamidele O Tayo, Daniel F Sarpong, Mary Amoakoh-Coleman, Vincent Boima and Gbenga Ogedegbe in SAGE Open Medicine
Footnotes
Acknowledgements
We appreciate the Stroke and Cardiovascular Research Training (S-CaRT) program for bringing the researchers together to work on the project and for providing funding. We also thank our research assistants in Nigeria and Ghana for their efforts.
Author’s contribution
OTIA, BPK, DBF, DF, ECP conceived the idea, conducted the study and analysed the data OTIA, BPK, DBF, DF, ECP, ABS, TBO, DSP, AM, BV, OG designed the study, wrote the manuscript, edited and revised the manuscript, approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Ethics Review Committees of Federal Teaching Hospital (FTH), Ido Ekiti, Nigeria (ERC/2020-06/15/377A) and Ghana Health Service (GHS), Accra, Ghana (GHS-ERC 007/10/20).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The sum of four thousand, nine hundred and ninety-nine dollars ($4,999) was received as grant for this project from NIH/FIC Stroke and Cardiovascular Research Training (S-CaRT) Institute, Prime Award No. 2D43TW009140-06.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.