
Abstract
Introduction and objective:
Pulmonary mucormycosis is a rare but rapidly progressive fatal disease. Limited data exist on the outcomes and factors associated with poor prognosis of pulmonary mucormycosis. The objective of this study was to evaluate clinical characteristics, factors associated with mortality, and outcomes of pulmonary mucormycosis at a tertiary care hospital in Pakistan.
Methods:
This was a retrospective observational study conducted at a tertiary care hospital in Karachi, Pakistan. Medical records of hospitalized patients diagnosed with proven or probable pulmonary mucormycosis between January 2018 and December 2022 were reviewed. Univariate and regression analyses were performed to identify factors associated with mortality.
Results:
Fifty-three pulmonary mucormycosis patients (69.8% male) were included, with mean age of 51.19 ± 21.65 years. Diabetes mellitus was the most common comorbidity [n = 26 (49.1%)]. Chronic lung diseases were present in [n = 5 (9.4%)], and [n = 16 (30.2%)] had concurrent coronavirus disease 2019 (COVID-19) pneumonia. The predominant isolated Mucorales were Rhizopus [n = 32 (60.3%)] and Mucor species [n = 9 (17%)]. Main radiological findings included consolidation [n = 39 (73.6%)] and nodules [n = 14 (26.4%)]. Amphotericin B deoxycholate was prescribed in [n = 38 (71.7%)], and [n = 14 (26.4%)] of patients received combined medical and surgical treatment. The median [interquartile range (IQR)] hospital stay was 15.0 (10.0–21.5) days. Intensive care unit (ICU) care was required in [n = 30 (56.6%)] patients, with 26 (49.1%) needing mechanical ventilation. Overall mortality was seen in 29 (54.7%) patients. Significantly higher mortality was found among patients requiring mechanical ventilation 20/29 (69%, p = 0.002). Immunosuppression (p = 0.042), thrombocytopenia (p = 0.004), and mechanical ventilation (p = 0.018) were identified as risk factors for mortality on multivariable analysis.
Conclusion:
This study provides essential insights into the clinical characteristics, outcomes, and mortality factors associated with pulmonary mucormycosis. The mortality rate was high (54.7%), particularly in patients with immunosuppression, thrombocytopenia, and those who required mechanical ventilation.
Introduction
Mucormycosis is a potentially devastating invasive fungal infection due to fungi within the Mucorales order. 1 Pulmonary mucormycosis is the second or third most frequent manifestation of mucormycosis.2,3 Recently, an increased incidence of pulmonary mucormycosis has been reported due to factors such as advanced immunosuppressive regimens, diabetes mellitus, post-viral complications, and enhanced awareness. 2 Therefore, increased vigilance in diagnosing and managing pulmonary mucormycosis is required within a broader patient context. 4 The diagnosis of pulmonary mucormycosis remains challenging due to the limited sensitivity and specificity of clinical diagnostic techniques. 4 Additionally, performance of diagnostic tools also varies across patient population. 5 Better patient outcomes in pulmonary mucormycosis hinge upon timely identification, accurate diagnosis, prompt administration of appropriate antifungal agents, and, whenever feasible, surgical intervention. The mortality linked to pulmonary mucormycosis remains high, possibly attributed to delayed diagnosis, the financial burden of management, and limited therapeutic choices. 6 Although earlier studies reported substantial pulmonary mucormycosis mortality rates (56–76%), recent figures have lowered to 29–38%.2,5,7,8 One of the factors leading to variability in mortality rate could be due to predisposing condition leading to mucormycosis. A recent study found 52% mortality in coronavirus disease 2019 (COVID-19)-associated pulmonary mucormycosis patients and reported hypoxemia and Aspergillus co-infection to be associated with mortality. 9
While previous studies have documented risk factors associated with mucormycosis, limited data exist regarding outcomes and factors associated with poor prognosis in pulmonary mucormycosis. Pulmonary mucormycosis warrants a detailed assessment due to its unique pathophysiological mechanisms, clinical presentation, and therapeutic challenges. This retrospective study aimed to bridge existing gaps in knowledge by determining clinical attributes, outcomes, and factors contributing to poor prognosis among patients with pulmonary mucormycosis.
Methods
This retrospective, observational study was conducted from January 2018 to December 2022 at the Aga Khan University Hospital (AKUH), Karachi, Pakistan. AKUH is a Joint Commission International (JCI) accredited state-of-the-art tertiary care center that provides care to the patients from all over the country and offers specialized services including bone marrow and solid organ transplant services, intensive care units (ICUs), and hematology–oncology services.
Data collection
Culture positive cases from sputum, tracheal aspirates, bronchoalveolar lavage, transbronchial, pleural, and lung biopsies for Mucorales were identified from laboratory database over the study period. Medical records of the identified cases were retrieved through Hospital Information and Management System (HIMS) and reviewed by primary investigators.
Inclusion criteria
Patients who fulfill the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium criteria 10 and/or Delphi consensus statement from the Fungal Infection Study Forum and Academy of Pulmonary Sciences, India for the COVID-19-associated pulmonary mucormycosis 11 were included.
Proven pulmonary mucormycosis was labeled when histopathology or cytology or culture obtained by a sterile procedure from a sterile site (pleural fluid or lung) showed aseptate hyphae or yielded growth of Mucorales.
Probable pulmonary mucormycosis was labeled when any one host factor as defined by EORTC or simultaneous or previous (within 3 months) COVID-19 along with compatible clinical features, and suggestive imaging (thick-walled cavity, large consolidation, reversed halo sign, or multiple large nodules) and aseptate hyphae or growth of Mucorales) in lower respiratory tract specimen were present.
As all cases were microbiologically positive, therefore, no possible pulmonary mucormycosis was included in this study.
We defined pulmonary mucormycosis as pulmonary or combined sinopulmonary disease.
Exclusion criteria
Patients were excluded if they had a culture positive result from sputum, tracheal aspirates, bronchoalveolar lavage, transbronchial, pleural, and lung biopsies, but their clinical presentation was not consistent with infection, but more with colonization or contamination as determined by primary physician or infectious diseases specialist. We have also excluded patients with clinical diagnosis of mucormycosis of any other organ, but the histopathology or cytology or culture was not obtained by a sterile procedure from a sterile site of pleura or lung. We have also excluded patients with rhinoorbitocerebral involvement only and disseminated disease.
A comprehensive review of electronic, printed medical records, radiology, and laboratory databases of selected patients was conducted, and relevant demographic information, along with comorbidities, risk factors, immunosuppression status, iron therapy, microbiology, imaging, treatment modality, complications, and outcomes was collected on predesigned proforma.
Patient outcomes were assessed in terms of the need for noninvasive ventilation, mechanical ventilation, ICU admission, length of stay (LOS) in the ICU and hospital, and overall mortality.
Ethical consideration
The study was reviewed and approved by the Ethics Review Committee, Aga Khan University (ERC # 2023-8525-24274). Due to the retrospective chart reviews and lack of direct involvement of patients or other human participants, a waiver of informed consent was given by the Ethics Review Committee, Aga Khan University. Patient identifiers were anonymized during data collection and analysis to maintain confidentiality.
Statistical analysis
The data was entered on IBM SPSS (Statistical Package for Social Sciences) version 26.0 (IBM Corp., Armonk, NY, USA) for analysis. Quantitative variables were presented as median with interquartile range (IQR) and mean and standard deviation (SD). Frequencies and percentages were computed for categorical or qualitative variables, namely underlying conditions, clinical characteristics, radiographic features, antimicrobial results, and disease outcomes. Post-stratification Chi-square test or Fisher’s exact test was applied. The logistic regression statistical analysis was conducted with a focus on capturing the comprehensive interplay of variables influencing the outcome of interest. Rather than solely relying on univariable results, a multivariable analysis approach was employed. This decision was grounded in two fundamental considerations: statistical significance and biological plausibility. The odds ratio (OR) and their 95% confidence intervals (CIs) were estimated, with mortality as an outcome. All p values were based on two-sided tests and significance was set at <0.05.
Results
Demographics
A total of 145 patients were identified from laboratory as culture positive for Mucorales. Of these, 53 (36.5%) patients fulfilled the diagnostic criteria and were included in the study. The mean age was 51.19 ± 21.65 years, and 37 (69.8%) were male. The demographics, risk factors, and clinical characteristics of patients are presented in Table 1.
Clinical characteristics of patients with pulmonary mucormycosis.
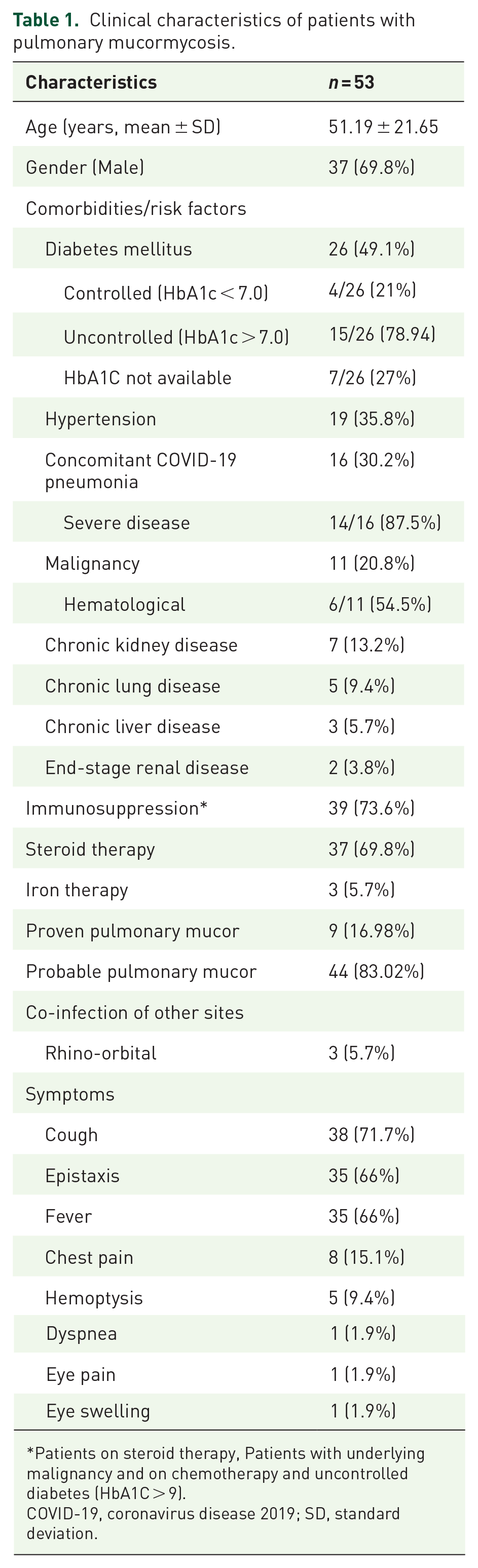
Patients on steroid therapy, Patients with underlying malignancy and on chemotherapy and uncontrolled diabetes (HbA1C > 9).
COVID-19, coronavirus disease 2019; SD, standard deviation.
Risk factors/comorbidities
Common comorbidities included diabetes mellitus 26 (49.1%) and hypertension 19 (35.8%). Of 26 diabetics 15/26 (78.94) had uncontrolled blood sugars (HbA1C > 7). Chronic lung diseases were present in 5 (9.4%) patients. A significant number of patients had some form of immunosuppression 39 (73.6%) and steroid therapy was received by 37 (69.8%) of patients. Eleven patients (20.8%) had underlying malignancy out of which 6 (54.5%) had hematological malignancies. A notable proportion of patients 16 (30.2%) had concurrent COVID-19 pneumonia, out of which 14 (87.5%) had severe/critical disease and 10 (62.5%) had diabetes mellitus. Three patients (5.7%) had admitted with injury, of which two had road traffic accident and one had gunshot injury. Three patients (5.7%) were on iron therapy due to end-stage renal disease.
Clinical features
The clinical findings were nonspecific and comparable to other entities of lower respiratory tract infection (Table 1). Productive cough 38 (71.7%), fever 35 (66%), breathlessness 35 (66%), chest pain 8 (15.1%), and hemoptysis 5 (9.4%) were the most frequent presenting symptoms.
Laboratory and radiological findings
Significant laboratory abnormalities at the time of presentation included anemia 36 (67.9%), thrombocytopenia 23 (43.4%), leukopenia 8 (5.1%), and hyponatremia 20 (37.7%) patients. The serum creatinine was raised (>1.5 mg/dL) in 19 (35.8%) (Table 2).
Laboratory and radiological characteristics of patients with pulmonary mucormycosis.

HRCT, high-resolution computed tomography.
On imaging bilateral abnormalities were observed in 34 (64.2%). The most frequent findings included consolidation 39 (73.6%), nodules 14 (26.4%), cavities 8 (15.1%), and pleural effusion 9 (17%) (Table 2).
Microbiology
Of the 53 patients, 9 (16.98%) had proven and 44 (83.02%) had probable mucormycosis.
The predominant isolated mucorales were Rhizopus species 32 (60.4%), Mucor species 9 (17.3%), Lichtheimia species 5 (9.4%), and Syncephalastrum species 5 (9.4%). Diagnostic procedures included tracheobronchial aspirate 33 (62.6%), tissue biopsy 8 (15.1%), and bronchoalveolar lavage 5 (9.4%) analysis (Table 2).
Treatment
Amphotericin B deoxycholate (Intravenous 1 mg/kg once in a day) was used in 38 (71.7%) patients, and 14 (26.4%) patients received combined medical and surgical treatment. Combined amphotericin B deoxycholate and caspofungin (70 mg on day 1 then 50 mg daily) were used in 3 (5.7%) patients and posaconazole (300 mg × BD for day 1 then 300 mg × daily) was used in 1 (1.9%) patient (Table 3). Lipid formulations of amphotericin were not given due to their limited availability and high cost in our country.
Treatment, complications, and outcome of patients with pulmonary mucormycosis.

ARDS, acute respiratory distress syndrome; COVID-19, coronavirus disease 2019; ICU, intensive care unit; IQR, interquartile range; LAMA, leave against medical advice; LOS, length of stay.
Outcome
The median (IQR) hospital stay was 15.0 (10.0–21.5) days. ICU care was required in 30 (56.6%) patients, with 26 (49.1%) needing mechanical ventilation. The median (IQR) ICU stay was 8.0 (3.0–13.50 days). The most serious complications were respiratory failure 44 (831%), acute respiratory distress syndrome (ARDS) 32 (60.4%), hospital acquired pneumonia (HAP) 26 (49%), and pneumothorax 8 (15.1%) (Table 3).
Isolated bacterial pathogens in HAP included Acinetobacter species (n = 11), Pseudomonas aeruginosa (n = 7), Klebsiella pneumoniae (n = 6), Stenotrophomonas maltophilia (n = 6), and methicillin-resistant Staphylococcus aureus (n = 5) (Table 2).
Overall mortality was 29 (54.7%), significantly higher among patients requiring mechanical ventilation 20/29 (69%). On univariable analysis, thrombocytopenia [OR 9.500 (95% CI 2.541–35.514) p = 0.001], ARDS [OR 9.600 (95% CI 2.659–34.666) p = 0.001], mechanical ventilation [OR 6.667 (95% CI 1.981–22.435) p = 0.002], and ICU [OR 4.375 (95% CI 1.371–13.959) p = 0.013] were associated with increased odds of death (Table 4). Immunosuppression [OR 15.899 (95% CI 1.101–229.570) p = 0.042], thrombocytopenia [OR 11.427 (95% CI 2.155–60.585) p = 0.004], and mechanical ventilation [OR 7.435 (95% CI 1.404–39.360) p = 0.018] were identified as risk factors for mortality on multivariable logistic regression analysis (Table 5).
Univariable analysis of clinical variables and risk of mortality in patients with pulmonary mucormycosis.

ARDS, acute respiratory distress syndrome; CI, confidence interval; COVID-19, coronavirus disease 2019; ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; OR, odds ratio.
Statistically significant values are highlighted in bold.
Multivariable analysis of clinical variables and risk of mortality in patients with pulmonary mucormycosis.

CI, confidence interval; OR, odds ratio.
Statistically significant values are highlighted in bold.
The Kaplan–Meier survival estimate analysis for all the included patients revealed that a considerable number of deaths occurred during the first 20 days of hospitalization. Following this initial period, a discernible disparity in survival emerged among remaining individuals with pulmonary mucormycosis (Figure 1).

Kaplan–Meier survival estimate analysis for pulmonary mucormycosis patients.
Discussion
In 2022, the World Health Organization (WHO) published the first Fungal Priority Pathogen List to identify fungi that are a great threat to public health. A total of 19 fungi were listed as priority pathogens and were categorized in critical, high, or medium priority group. 12 Mucorales had been recognized as one of the priority organisms included in the high-priority group due to its high mortality and challenges in the diagnosis, treatment, and prevention. The need for better diagnostics, species-specific antifungal susceptibility data on a large number of strains for the development of clinical breakpoints, and prospective clinical studies to gather morbidity and mortality data was highlighted as a knowledge gap.
In this study, we report 53 cases of pulmonary mucormycosis with a high mortality rate. Diabetes, hypertension, prior pulmonary disease, and immunosuppression were common comorbid illnesses in patients with pulmonary mucormycosis. Around 30% of pulmonary mucormycosis patients in this study had concurrent COVID-19 pneumonia. Overall, more than 50% of the patients required ICU stay, and frequent complications identified were HAP, ARDS, respiratory failure, and pneumothorax. The mortality rate was high (around 55%) in this study population, and immunosuppression, thrombocytopenia, and mechanical ventilation were identified as risk factors for mortality on multivariable analysis.
Pulmonary mucormycosis has traditionally been considered as a rare and fatal disease. A review of literature of around 30 years from 1970 to 1999 reported 87 cases of pulmonary mucormycosis with a survival rate of only 44%. 13 This rate has been reported to be even higher if patients are admitted in a critical care setting. A retrospective case series published prior to COVID-19 pandemic reported a mortality rate of 100% in eight critically ill patients with pulmonary mucormycosis. 14 A recent systemic review found pooled mortality of pulmonary mucormycosis of 57%, similar to our study where mortality rate was 54.7%. 15
Diabetes especially with poor glycemic control is an important risk factor for many infections and also predisposes patients for lower respiratory tract infections. 16 The other conditions predisposing to increased risk of developing mucormycosis are organ transplant, neutropenia, immunosuppressive therapy, malignancies, and increased level of serum iron, similar to finding of our study.17–19
Most patients in our study had prior immunosuppression including steroids use, malignancy, and diabetes mellitus. Similarly, a systemic review conducted in China identified pulmonary mucormycosis as the most prevalent form and diabetes as the predominant risk factor followed by systemic administration of corticosteroids or other immunosuppressant, hematological malignancy and solid organ transplant among patients with mucormycosis. 20
A recent review of mucormycosis in the Middle East and North America (MENA) region observed diabetes and immunosuppressive conditions as the prevailing risk factors with mucormycosis. 21 A systemic review of mucormycosis from Iran also identified diabetes, solid organ, and bone marrow transplantation as important predisposing condition to develop this serious infection. 22 Interestingly, a multicenter study from India found diabetes mellitus as the predominant risk factor in all subtypes of mucormycosis. 23 . The rising incidence of mucormycosis over last two decades has further intensified worldwide due to COVID-19 pandemic in many countries experiencing a particularly high upswing. 24
A significant number of patients (n = 16, 30.2%) had COVID-19 pneumonia in the present study. Among patients with concomitant COVID-19 and pulmonary mucormycosis, the majority (87%) had severe/critical COVID-19, and 68.8% had ARDS and required mechanical ventilation. Although less common than aspergillosis, pulmonary mucormycosis is well known as one of the serious infections associated with high mortality in patients with severe and critical COVID-19. Similar to pulmonary mucormycosis in non-COVID-19 patients, patients with pulmonary mucormycosis and COVID-19 have a high mortality. Pulmonary involvement has been reported to be an independent risk factor for mortality in a study from India. 25 Poor outcomes were identified in patients with both active diseases as well as those who had recovered from acute phase of COVID-19. Diabetes, diabetic ketoacidosis, poor glycemic control, hyper inflammatory state with severe infection, and use of prolonged steroids were found to be associated with increased morbidity and mortality in patients with pulmonary mucormycosis and COVID-19.26,27 Another recent study reported pulmonary mucormycosis in COVID-19 as a distinct syndrome with a higher mortality than other forms of mucormycosis with poor prognosis in patients with hypoxemia and simultaneous aspergillosis and better survival with surgery. 9 Effective glycemic control and judicious use of glucocorticoids should be prioritized in patients with COVID-19 to protect against mucormycosis and improve patient outcome.
Clinical features are nonspecific, similar to other lower respiratory tract infections and cannot be utilized to identify patients with pulmonary mucormycosis precisely. Productive cough, shortness of breath, and fever were the most common symptoms in this study and few patients also developed hemoptysis. This is in accordance with study done by Feng and Sun, 8 except increased frequency of hemoptysis noted, that is, 28.3%, which is in contrast to present study whereas only 9.4% presented with hemoptysis. Radiological features are also nonspecific and can present as consolidation, nodules, cavities, and pleural effusion, consistent with finding of present study. However, reverse halo sign, nodules, and ground glass haziness can be considered as supportive evidence to initiate antifungal therapy against mucormycosis in relevant clinical context.28–30
The most common species isolated from respiratory specimens were Rhizopus species and Mucor species in this study. Both of these are recognized as predominant mucorales among Asian countries. 1 Rhizopus spp and mucor spp were also found to be the most common organisms in patients with mucormycosis associated with COVID-19 among Pakistani population with predominantly pulmonary disease. 31
Combined surgical and medical treatment is associated with favorable outcome in pulmonary mucormycosis.8,9,32 This could explain high mortality in current study as very few patients received both antifungal therapy and surgical intervention. A significant number of patients had ARDS leading to need of mechanical ventilation and ICU stay in this study. Among patients with pulmonary mucormycosis and severe/critical COVID-19, 68.8% developed ARDS and required mechanical ventilation.
Thrombocytopenia, severe COVID-19 disease, ICU stay, ARDS, respiratory failure, and mechanical ventilation were common among nonsurvivors of pulmonary mucormycosis in this study depicting advanced and critical state of illness. Disseminated disease, voriconazole use at clinical suspicion for invasive mold pneumonia, prolonged neutropenia, high APACHE II score, severe lymphocytopenia, thrombocytopenia, high lactate dehydrogenase (LDH) levels, steroid use, and longer duration of disease are predictor of poor outcomes in pulmonary mucormycosis.15,33–35
Although diabetes was the most prevalent predisposing condition, it was not associated with high risk of mortality in this study. This could be due to the high prevalence of diabetes mellitus in the general population, and meticulous efforts were made toward management of hyperglycemia after diagnosis.
Our study has few limitations; being retrospective and single-center study, results cannot be generalized to larger population. All patients presented to the hospital during the study period were included in the study, and sample size estimation was not performed. Hence, power analysis for sample size calculation was not done. Another limitation is the inclusion of hospitalized patients, which provided insight into severe cases of pulmonary mucormycosis. Consequently, our findings do not provide information on the manifestations and outcomes of less severe cases managed as outpatients. We also found a lower proportion of diabetic patients in our study compared to other countries. This could also be due to a referral bias as our center is a tertiary care multidisciplinary referral center, which receives complicated patients from within and outside the city. The low number of patients with diabetes could be due to referral bias and may not reflect the actual prevalence of diabetes in patients with pulmonary mucormycosis.
Conclusion
Pulmonary mucormycosis is a highly aggressive and fatal disease that is prevalent in patients with compromised immunity. Due to its rapid progression and high mortality rate, pulmonary mucormycosis must be managed effectively with combined medical and surgical interventions to improve survival. The survival rates of this potentially curable illness must be increased through early detection and active care of pulmonary mucormycosis.