
Abstract
Primary ciliary dyskinesia is a rare autosomal recessive disorder that impairs mucociliary clearance and predisposes children to chronic respiratory infections. Invasive fungal infections caused by Lichtheimia (Absidia) corymbifera are typically confined to profoundly immunocompromised hosts and are exceptionally uncommon in patients without systemic immunosuppression. We report the case of a 6-year-old boy with genetically confirmed primary ciliary dyskinesia (C3orf67 mutation) and right–middle-lobe bronchiectasis who developed persistent cough and increased sputum production. High-resolution chest computed tomography demonstrated right–lower-lobe consolidation and segmental atelectasis. Bronchoalveolar lavage microscopy revealed broad, aseptate/pauci-septate hyphae, and the culture yielded L. corymbifera, establishing the diagnosis of pulmonary mucormycosis. The child received intravenous liposomal amphotericin B for 18 days, followed by oral azole step-down therapy, resulting in complete clinical and radiological recovery. This case expands the spectrum of invasive mucormycosis to include pediatric patients with primary ciliary dyskinesia in the absence of classical immunosuppressive risk factors. Early bronchoscopy, mold-directed culture, and prompt antifungal therapy, supported by multidisciplinary care, are critical for favorable outcomes.
Keywords
Introduction
Primary ciliary dyskinesia (PCD) is a rare autosomal recessive disorder characterized by defective ciliary motility, leading to impaired mucociliary clearance, recurrent oto-sinopulmonary infections, bronchiectasis, and progressive lung damage.1–3 Although bacterial colonization—especially with Pseudomonas aeruginosa and Haemophilus influenzae—is common in PCD, invasive fungal infections (IFIs) are infrequently reported unless associated with systemic immunosuppression or significant structural lung disease.
Mucormycosis is an aggressive IFI caused by fungi of the order Mucorales, including Rhizopus, Mucor, Rhizomucor, and Lichtheimia (formerly Absidia).4–6 These infections typically occur in immunocompromised individuals, such as those with hematological malignancies and uncontrolled diabetes or those receiving long-term immunosuppressive therapy. Lichtheimia corymbifera is a rare but angio-invasive pathogen that has been reported in sporadic cases among immunocompetent individuals with chronic pulmonary conditions.7–9
Pulmonary mucormycosis presents with nonspecific respiratory symptoms and radiologic findings that often mimic bacterial or Aspergillus infections. The disease progresses rapidly due to spore inhalation, vascular invasion, and tissue necrosis, with mortality rates exceeding 50% in localized cases and up to 95% in disseminated forms.10–12 Diagnosis is challenging and requires a high index of suspicion supported by bronchoscopy and mycological confirmation.
Herein, we present a rare case of pulmonary mucormycosis caused by L. corymbifera in a child with genetically confirmed PCD and no systemic immunosuppression. This report underscores the potential for IFI in structurally compromised lungs, even in immunocompetent hosts, highlighting the importance of early diagnosis and multidisciplinary management.
Case presentation
The reporting of this study conforms to the Case Report (CARE) guidelines. 13 A Saudi preschool boy with genetically confirmed PCD due to a C3orf67 mutation presented to Alhada Armed Forces Hospital, Taif, Saudi Arabia, in January 2023, with a 2-week history of persistent cough and sputum production. His medical history included recurrent respiratory infections, bronchial asthma, obstructive sleep apnea after adenotonsillectomy, and bilateral hearing impairment. His family history was significant for consanguinity and a similarly affected sibling. Upon admission, he was afebrile (temperature: 37°C) with blood pressure of 90/59 mmHg, heart rate of 105 bpm, respiratory rate of 22/min, and oxygen saturation of 96% on room air; physical examination revealed mild right-sided chest crepitations, and his body mass index was 14.0 kg/m2 (11th percentile). Laboratory investigations revealed that the white blood cell count was 16.1 × 109/L (reference: 5.00–15.00), neutrophil count was 13.2 × 109/L (reference: 1.50–8.00), C-reactive protein level was 452.4 mg/L (reference: 0.0–5.0), erythrocyte sedimentation rate was 66 mm/h (reference: 2–30), creatinine level was 80 µmol/L (reference: 27–62), urea level was 9.3 mmol/L (reference: 2.5–6.0), sodium level was 132 mmol/L (reference: 135–145), potassium level was 3.0 mmol/L (reference :3.5–5.1) (dropping later to 1.6 mmol/L), and bicarbonate level was 16 mmol/L (reference: 17–26). Chest computed tomography (CT) (Figure 1) demonstrated right lung collapse, bronchiectasis, and pleural effusion. Abdominal ultrasound showed hepatosplenomegaly and confirmed bilateral pleural effusions. Bronchoscopy revealed thick yellow mucus in the right middle lobe, whereas bronchoalveolar lavage (BAL) microscopy (lactophenol cotton blue stain) showed broad aseptate and pauci-septate hyphae, and subsequent fungal culture grew L. corymbifera (Figures 2 and 3). Blood cultures, respiratory multiplex viral polymerase chain reaction (PCR), and pleural fluid tuberculosis PCR were negative. He was started on liposomal amphotericin B (5 mg/kg/day); however, after 18 days, he developed severe hypokalemia (1.6 mmol/L), electrocardiogram changes, and metabolic acidosis, consistent with amphotericin-induced distal renal tubular acidosis. He was admitted to the pediatric intensive care unit (PICU) for intravenous potassium and bicarbonate correction, and amphotericin B was discontinued. After stabilization, he improved clinically and was discharged on oral itraconazole (5 mg/kg/dose PO twice daily) for 8 weeks. This case highlights the potential for invasive mucormycosis in immunocompetent children with structural lung disease such as PCD and underscores the importance of early diagnosis, targeted antifungal therapy, and vigilant monitoring for drug-related complications. A follow-up CT scan demonstrated radiological resolution of right lower lobe consolidation and atelectasis (Figure 4). The BAL culture was sterile, corroborating the patient’s clinical recovery following antifungal therapy.

(a–c) Initial chest computed tomography revealed right lung collapse, bronchiectasis, and pleural effusion.
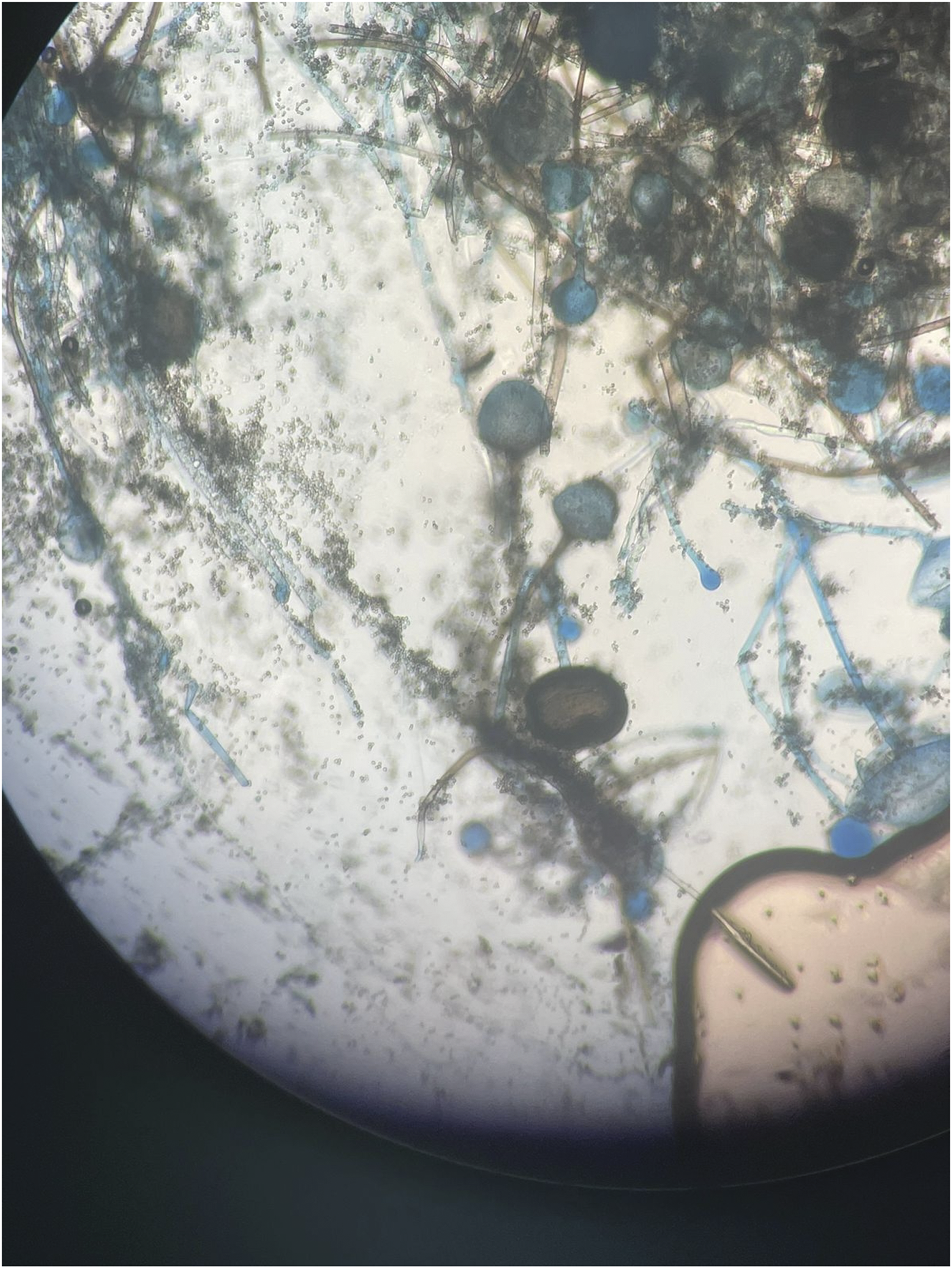
Microscopic view of the clinical specimen showing broad, ribbon-like, pauci-septate hyphae and large spherical sporangia characteristic of Lichtheimia (Absidia) corymbifera. Some sporangia appear darker, possibly ruptured, or more mature.

Microscopic view of a filamentous fungus showing broad, aseptate and paucity septate hyphae and large, spherical sporangia at the tips of sporangiophores. The fungus structures are stained with lactophenol cotton blue.

(a–c) Follow-up computed tomography scan showing radiological resolution of right lower lobe consolidation and atelectasis.
Discussion
This case of a 6-year-old boy with PCD and right-lobe bronchiectasis who developed an invasive Absidia corymbifera infection highlights the potential for serious fungal disease in patients without classical immunosuppressive risk factors. Although Absidia most often affects individuals with hematologic malignancies, uncontrolled diabetes, or prolonged immunosuppression,5,9,14,15 localized immune dysfunction in PCD may also predispose patients to infection.
Structural lung disease and prior antibiotic exposure may disrupt the pulmonary microbiome, facilitating fungal colonization and progression to invasive disease. PCD is classically linked to recurrent bacterial infections owing to impaired mucociliary clearance; however, fungal infections remain rare and under-recognized. However, Aspergillus species have been reported in patients with PCD and bronchiectasis, potentially related to airway remodeling and impaired clearance of inhaled fungal spores.
Mucormycosis in immunocompetent patients is exceedingly rare, but it has been reported in cases of structural lung disease, chronic inflammation, or extensive antibiotic use, which may disrupt normal microbiota and allow fungal proliferation. However, chronic lung disease and prior structural damage may have facilitated fungal colonization and subsequent invasive infection, as reported in the literature on pulmonary mucormycosis in nontraditional hosts. 16 The patient in this case lacked traditional risk factors such as diabetes, malignancy, or immunosuppression, rendering this an unusual presentation. Although colonization is theoretically possible in structurally abnormal lungs, the presence of broad aseptate hyphae on BAL smear and the patient’s clinical resolution with antifungal therapy confirm true invasive disease rather than colonization.
Pulmonary mucormycosis follows an aggressive course with mortality exceeding 50%, which rises to 95% in disseminated disease.11,12 Diagnosis is frequently delayed because of nonspecific symptoms and low clinical suspicion in patients without systemic immunosuppression. 8 In this case, A. corymbifera was confirmed by BAL culture, underscoring the importance of early invasive sampling and comprehensive mycological work-up in children with chronic lung disease.
The pathogenicity of Absidia stems from its angio-invasive behavior, leading to vascular thrombosis and tissue necrosis. 7 Airborne sporangiospores readily colonize damaged airways, particularly in bronchiectatic lungs with impaired clearance. 10
Amphotericin B remains the therapeutic cornerstone,17,18 but it carries a substantial risk of nephrotoxicity and electrolyte disturbances; in our patient, severe hypokalemia necessitated PICU admission and discontinuation of the drug. Liposomal formulations reduce toxicity; however, their use may be limited by cost and availability. Although itraconazole has poor or no activity against Mucorales species in both in vitro and clinical studies, our patient remained free of recurrent symptoms.
In summary, this case emphasizes that localized immune deficits—such as those resulting from PCD and bronchiectasis—can permit invasive mucormycosis in otherwise immunocompetent children. Heightened clinical vigilance, prompt diagnostic bronchoscopy, multidisciplinary management, and careful monitoring for treatment-related complications are essential to improving outcomes in these rare yet life-threatening infections.
Novelty
The novelty of this case report lies in the following aspects. 1. Rare pathogen in an uncommon host: To the best of our knowledge, this is the first pediatric case of pulmonary mucormycosis caused by L. corymbifera in a child with genetically confirmed PCD and no systemic immunosuppression. 2. Expanding disease spectrum: The case challenges existing paradigms by demonstrating that invasive mucormycosis can occur in structurally compromised yet immunocompetent lungs, likely due to localized immune dysfunction in PCD. 3. Clinical and radiological recovery: Successful treatment was achieved with liposomal amphotericin B followed by itraconazole, despite the latter’s limited in vitro activity against Mucorales, suggesting a potentially beneficial off-label use in select nonsevere cases. 4. Highlighting the need for a diagnostic approach: This case underscores the need for early bronchoscopy and mold-directed cultures in atypical pediatric pneumonia cases, in which fungal causes are often overlooked in immunocompetent children.
Limitations
The limitations of the study were as follows. 1. Single case report: The findings are based on a single patient, which limits the ability to generalize outcomes or establish causality between PCD and increased susceptibility to mucormycosis. 2. Lack of in vitro susceptibility data: No antifungal susceptibility testing was performed for the Lichtheimia isolate, rendering the effectiveness of itraconazole anecdotal rather than evidence-based. 3. Short follow-up duration: Long-term clinical and microbiological follow-up data (e.g. relapse rates or fungal colonization) were not provided. 4. Absence of comparative analysis: The study did not compare the outcomes with those of other antifungal regimens or similar cases in the literature, limiting contextual interpretation of treatment efficacy. 5. No exploration of pathophysiological mechanisms: The specific immunological or structural features of PCD that may predispose patients to fungal infection were not investigated in detail.
Conclusion
This case highlights that invasive mucormycosis due to A. corymbifera can occur in children with structural lung disease such as PCD, even without classical immunosuppressive risk factors. Early diagnostic bronchoscopy, mycological evaluation, and prompt antifungal therapy were key to the favorable outcome. Clinicians should remain vigilant for fungal infections in pediatric patients with chronic lung disease.
Footnotes
Acknowledgments
To our patient and his family for their kind participation in this work.
Author contributions
All authors contributed substantially to writing the manuscript, reviewing the literature, the concept and design, acquisition, and interpretation of data; drafting the article, revising it critically for important intellectual content; and final approval of the version to be published.
Data availability
All data and materials related to the study are included in the current manuscript.
Declaration of conflicting interests
All authors declare no competing interests related to the study.
Funding
No funds were available for the current research.