
Abstract
Background:
Outpatient parenteral antimicrobial therapy (OPAT) and complex outpatient antimicrobial therapy (COpAT) are common practice in the management of infectious diseases (IDs). However, providing OPAT/COpAT can pose significant challenges pre- and post-discharge, particularly in vulnerable patient populations.
Objectives:
The objective of this study is to assess outpatient complications related to OPAT/COpAT in patients discharged with a home health services referral and to identify pre- and post-discharge intervention opportunities and the associated cost-savings that could be achieved with a multidisciplinary ID team-run OPAT/COpAT program.
Design/methods:
This is a retrospective cohort study of patients who were discharged with OPAT/COpAT through home health services over a 3-month study period. Data on potential pre-discharge interventions and post-discharge complications were recorded.
Results:
Medication-related issues were the most common pre-discharge complications, accounting for more than 50% of identified intervention opportunities. More than half of the included patients experienced at least one documented outpatient complication post-discharge with peripherally inserted central catheter-line-related complication (20.7%) being the most common issue. Using previously published cost-estimates, the implementation of a designated pre- and post-discharge OPAT/COpAT program could have saved over $100,000 over the 3-month study period.
Conclusion:
A multidisciplinary OPAT/COpAT program located in a high social vulnerable area can help reduce complications related to a patient’s antimicrobial therapy. Medication-related issues represent a major area for potential intervention. Our findings suggest that a multidisciplinary ID team will have ample opportunities to improve the transition of care, at both pre- and post-discharge, for patients requiring antimicrobial therapy.
Introduction
Infectious diseases (IDs) are a major economic burden on healthcare systems, with hospital admissions costing at least $96 billion and contributing to 4.5 million hospital days a year. 1 In an effort to shorten inpatient hospital stays, insured patients may have the option of receiving outpatient parenteral [outpatient parenteral antimicrobial therapy (OPAT)] and/or oral antimicrobial therapy [complex outpatient antimicrobial therapy (COpAT)] for complex infections requiring extended treatment (i.e., osteomyelitis) through a home-based OPAT/COpAT model.2–4 While OPAT has been associated with lesser costs and improved patient quality of life when compared to hospitalization, it has been shown that more than 30% of patients discharged on OPAT experience readmission of therapy-related events, including peripherally inserted central catheter (PICC)-related complications and antibiotic-related adverse events.5,6
The involvement of a multidisciplinary ID team in an established OPAT program has been shown to reduce antimicrobial prescribing errors. 7 Through collaboration with home health services, the dedicated OPAT/COpAT program can enhance the continuity of care by optimizing the duration of antimicrobial therapy pre-discharge and improving safety monitoring by receiving and responding to critical laboratory results post-discharge. Nonetheless, there is limited data that describes the utility of pre- and post-discharge OPAT/COpAT programs in optimizing patient care, particularly in socially vulnerable communities where inequities in healthcare access have detrimental outcomes. 8
Loma Linda University Medical Center (LLUMC) is a 450-bed Academic Health Center located in San Bernardino County, CA, the largest county in the contiguous United States. San Bernardino County is one of the most diverse areas in California; however, it is ridden with prevalent inequities in social determinants of health, including education, housing environment, and access to healthcare. 9 These disparities in social determinants of health are potential contributors to the variable, and often high, social vulnerability recognized throughout the county. To this, 29.9% of the racially/ethnically minoritized individuals in the county live impoverished, more than 15% of minoritized individuals are uninsured, and one in five individuals lack essential health literacy competencies. 10 Consequently, high social vulnerability has been linked to a heightened risk for adverse health outcomes, including those that are infectious related. 11
To address the current gap in the literature related to antimicrobial stewardship in socially vulnerable areas, the primary objectives of this study were to evaluate the outpatient complications of patients discharged with a referral for home health services to complete home-based OPAT/COpAT and to identify opportunities for an OPAT/COpAT program with a multidisciplinary pre- and post-discharge ID team to heighten the awareness of common OPAT/COpAT-related complications and describe potential cost-savings in total inpatient costs.
Methods
This was a retrospective cohort study of adult patients admitted to LLUMC between 2nd January 2021 and 3rd April 2021 and were discharged with a referral for home health infusion services were screened for inclusion. Those discharged on either intravenous (IV) or oral (PO) antimicrobials met the inclusion criteria, whereas those not discharged on antibiotics were excluded.
Inpatient ID service, when consulted, provided antimicrobial recommendations. Home health services and related orders were coordinated by a case manager and the patient’s primary team. After discharge, patient laboratory results were sent to the primary care provider. Patient who had an inpatient ID consult were scheduled for an outpatient ID clinic visit to determine need for antimicrobial continuation.
Demographic information, including self-reported race and ethnicity, and comorbid conditions, were collected by chart review. Social vulnerability was estimated using the CDC’s Social Vulnerability Index (SVI), which is a data-driven tool that identifies and maps communities at risk of negative health outcomes during emergencies or disasters. 12 The SVI is calculated by assigning scores to 16 social factors, which are grouped into four categories: socioeconomic status, household composition and disability, minority status and language, and housing type and transportation. Based on the scores, patients are then categorized into lowest, medium-low, medium-high, and highest social vulnerability statuses. 13
Details of the infection type were obtained by collecting microbiology data and the suspected source of infection documented in the discharge summary. The regimen prescribed at discharge was detailed, noting the total number of agents, dose, prescribed route, and frequency of each antimicrobial agent. Length of inpatient hospital stay and rates of 30-day readmission were recorded.
The primary outcomes of this study were to identify opportunities for an OPAT/COpAT program, with a multidisciplinary pre- and post-discharge ID team. Potential pre-discharge interventions were evaluated retrospectively and classified into the following categories: clarification of duration of therapy, broadening or narrowing therapy, adjustment in antibiotic dose and/or interval, clarification of missing monitoring parameters, discontinuation of inappropriate therapy, transition from IV to PO route, and consolidation of antibiotics. Clarification of duration of therapy at point of discharge was identified when documented outpatient antibiotic orders did not match the recommended duration by the inpatient ID consult team. Post-discharge complications of patients who were discharged with home-based OPAT/COpAT were described, which included antimicrobial-related lab abnormalities or adverse reaction, PICC-line-related complication, worsening infection, and loss to follow-up.
The secondary outcomes include estimated cost-saving potential with an established OPAT program using previously published cost-estimates.3,14 The cost-estimates used in the study included: placement of a PICC-line ($1210), cost of home health service ($300.00/day), and hospitalization costs ($1605/day).
Study data were collected and managed using REDCap (Vanderbilt University, Nashville, TN, USA). Data were analyzed using IBM SPSS version 26 (IBM, Armonk, NY, USA). Normality tests were performed using the Shapiro–Wilk test on all continuous variables. Continuous variables were represented by either mean (±standard deviation) or median (interquartile range IQR 25–75%) as appropriate. Categorical variables were represented by counts and percentages.
Results
During the study period, a total of 123 insured patients were identified with home health infusion referrals. After exclusion criteria were applied, a total of 77 patients met study inclusion for further evaluation. Table 1 summarizes the baseline characteristics of the patients. The majority of our population racially/ethnically identified as non-Hispanic White (45.5%) and almost 60% of the patients were categorized into the highest SVI group (n = 45), followed by 24.7% that were classified as medium-high (n = 19), 14.3% in medium-low (n = 11), and 2.6% in the lowest social vulnerability group (n = 2). The median age was 60 years (44, 71), with 43 (55.8%) identifying as male. The median Charlson Comorbidity Index (CCI) score was 3. Overall, the median length of hospital stay was 8 days.
Baseline demographics.

IQR, interquartile range; HTN, hypertension; DM, diabetes; CHF, congestive heart failure; CCI, Charlson Comorbidity Index; IVDU, intravenous drug use; UTI, urinary tract infection; CNS, central nervous system; SSTI, skin and soft tissue infection; BSI, bloodstream infection, IV, intravenous; OPAT, outpatient parenteral antimicrobial therapy; PO, oral; CoNS, coagulase negative staphylococcus; MSSA, methicillin sensitive staphylococcus aureus; MRSA, methicillin resistant staphylococcus aureus; GNR, gram negative rod; Abx, antibiotic.
Outpatient antimicrobial therapy was most commonly prescribed for bone/joint infections compromising 38% of cases. Following this, cardiovascular and intra-abdominal infections were the next most frequent indication encountered, each accounting for 14% of cases. Monomicrobial infections (45.5%) were more common than polymicrobial (26%) and culture-negative (28.6%) infections. The most commonly isolated pathogens were Enterobacterales (n = 28) followed by coagulase-negative Staphylococcus (n = 10) and methicillin-sensitive Staphylococcus aureus (n = 10). A total of 60 patients were discharged on IV antimicrobials only, 15 were discharged on both IV and PO antimicrobials, and 2 were discharged on PO antimicrobials only. The median duration of prescribed OPAT at discharge was 23 days. Details of the agent(s) prescribed at discharged are detailed in Table 1. The leading antimicrobials prescribed were ceftriaxone (n = 18) and meropenem (n = 14) for the IV route, and metronidazole (n = 11) for the PO route. Nineteen of the 77 patients were discharged with more than one antimicrobial agent.
Table 2 provides details on the potential interventions at the point of discharge and the outpatient complications encountered. Prior to discharge, 33 of the 77 patients had at least one potential intervention opportunity, totaling 51 interventions. Of these 51 potential interventions, 26 (51%) potential interventions were medication-related. The most common intervention opportunities were clarification of duration of therapy (n = 19), followed by broadening/narrowing antimicrobial choice (n = 14) and dose adjustment/optimization (n = 8). Documented delays in discharge due to OPAT-related issues were observed in eight patients and resulted in a total of 58 additional hospital days. Insurance-related issues (n = 4/8) were the most documented reason for delay in discharged, followed by coordination of care (n = 2/8) and treatment-related delays (n = 2/8).
Pre-discharge interventions and post-discharge complications.
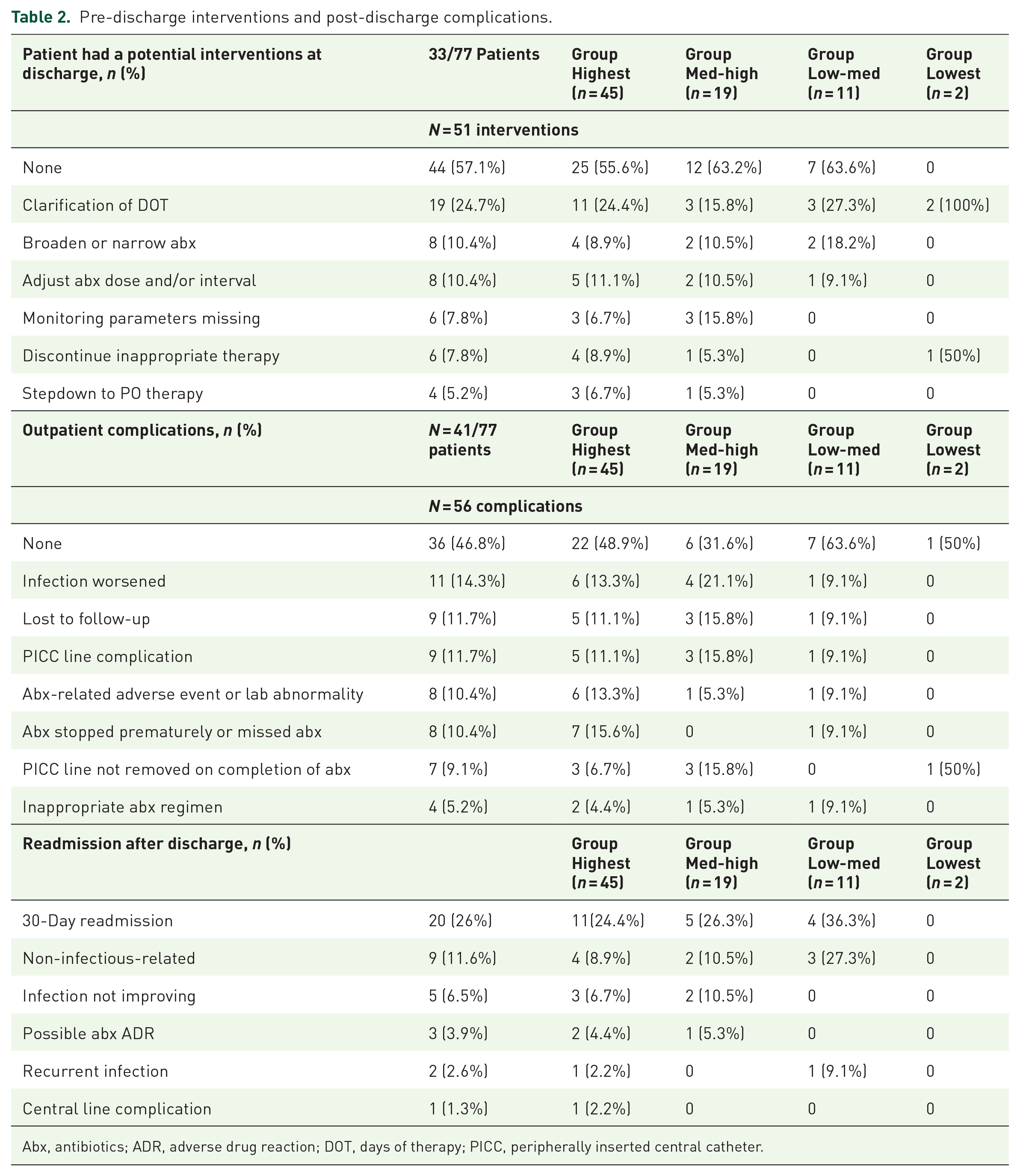
Abx, antibiotics; ADR, adverse drug reaction; DOT, days of therapy; PICC, peripherally inserted central catheter.
After discharge, 9 patients were lost to follow up and 41 patients experienced at least one identified outpatient issue, including PICC-line-related complication (20.7%), worsening infection (14.3%), and antimicrobial-related reaction (10.4%). For the 11 patients who were noted to have a worsening infection, all patients were treated with IV antimicrobial therapy, 3 of whom additionally received oral metronidazole. Bone/joint infections remained the most common indication (n = 7/11), followed by a case of myositis (n = 1), intraabdominal abscess (n = 1), complicated urinary tract infection with renal abscess (n = 1), and cocci meningitis (n = 1). Three patients had PICC-line-related issues resulting in missed antibiotic doses. Two patients had their therapy extended by ID physician during outpatient clinic visit. Finally, two patients were lost to outpatient follow-up.
A total of 20 patients were readmitted within 30 days of discharge, with 10 of the 20 patients being readmitted due to at least one OPAT-related issue including worsening infection (9.1%), recurrent infection after completion of therapy (3.9%), possible antimicrobial-related reaction due to antimicrobial therapy (3.9%), and a PICC-line-associated complications (1.3%). An exploratory analysis of outcomes stratified by SVI score is also included in Table 2, but due to the limited number of patients in groups other than the highest SVI group, the data are presented descriptively, and no further analysis was performed.
The potential cost-savings of an established OPAT program with a pre- and post-discharge ID team was also assessed in this study. Pre-discharge, eight patients experienced discharge delays resulting in 58 hospital days that could have been avoided, leading to potential savings exceeding $93,000. Post-discharge, thirteen patients could have avoided up to 157 days of home health services with clarification of the duration of therapy. Assuming a daily cost of $300 for home health services, the potential savings could have been up to $47,100. Additionally, five patients could have avoided CVC/PICC line placement at discharge given the availability of an alternative oral agent, resulting in potential savings of over $6,000. Taken together, an established pre- and post-discharge ID in an OPAT program has significant cost-saving potential and may have saved over $100,000 over a 3-month period.
Discussion
In this study, we aimed to identify the existing limitations in the OPAT procedures of an institution serving a highly socially vulnerable population. Our findings indicate that a substantial proportion of the insured patients, 64/77 (83%), discharged with OPAT/COpAT were from an area of medium-high or high vulnerability. Prior studies have demonstrated that people residing in areas of high vulnerability, often characterized by low socioeconomic status, are more likely to have chronic comorbidity and less likely to have a primary care provider to properly manage the chronic ailment. As reflected in our study, the majority of the included patients, 45/77 (58%), had at least one chronic illness, with diabetes and hypertension being the most prevalent. 15 Of interest, chronic illnesses have been shown to exacerbate or increase the severity of IDs. This is of concern as our study documented worsening infection following discharge in 9/77(12%) patients, all of whom were from areas of mid-high or high vulnerability.
A dedicated OPAT program that includes multiple disciplines has the potential to decrease hospital readmissions and antimicrobial-related adverse events. Our study highlights the need for an expert in resolving medication-related issues in areas of high vulnerability, where the majority of our pre-discharge interventions were antimicrobial-related. With this, ID-trained pharmacists recognize and resolve antimicrobial-related issues and are integral to the multidisciplinary ID team. Other studies have also demonstrated the importance of integrating an OPAT-designated service into their healthcare system and recognizing that there is not a customary approach for OPAT program structure. To this, one approach is the transitions of care OPAT bundle developed by a hospital located in the Bronx, NY. 12 The OPAT model involved ID professionals, homecare agencies, and nursing facilities that collaborated extensively to ensure ease in the transition at discharge for the patient. Another study from a hospital in Chicago implemented a structured OPAT program that included an ID physician, an ID pharmacist, and a designated OPAT nurse. 7 While different in approach and structure, both programs saw a decline in OPAT-related complications after establishing an intervention designed to optimize outpatient treatment.
Herein, we identified 51 potential areas for intervention prior to discharge in 31/77 (41%) of the patients. This is of particular interest as more than 50% of the potential opportunities for intervention were medication-related. These included clarification of the duration of therapy and adjustments to the therapeutic regimen (including either broadening or narrowing therapy). These results parallel previously published literature that highlights the importance of reviewing a patient’s medication profile prior to discharge to reduce medication errors. 7 Furthermore, a quasi-experimental cohort reported an increase in the process of care measures following the implementation of a designated ID transitions team. 16 The investigators noted a significant decrease in antimicrobial prescribing errors following the establishment of this team. Prior to the establishment of the transitions team, there was an antimicrobial prescribing error in 18.1% of discharges. This number was decreased in the post-intervention group, with only 1.36% of discharges having a noted prescribing error. While we cannot definitively state that the number of errors uncovered during our investigation would have been reduced with the implementation of a designated OPAT/COpAT-focused transition service at our institution, the data from similar efforts lend itself to this being a probable outcome.
Additionally, there were 56 complications identified in 41/77 (53%) patients and a 30-day readmission in 20/77 (26%) of the patients. The complications and hospital readmissions occurred most often in patients from areas of mid-high or high social vulnerability, with 16/20 (80%) of readmissions in this group. The most common complications were worsening infection in 11/77 (14%), PICC-line-related complications in 9/77 (12%), or losses to follow-up in 9/77 (12%). These results mirror other studies that report an increase in complications when long-term IV or oral therapy are provided without the involvement of designated transition teams. Investigators at an urban academic center also reported readmissions due to disease worsening or progression as well as line-associated issues prior to the implementation of an OPAT program and saw a significant reduction in the readmission rates following the integration of a structured OPAT program.7,12 Also, patients residing in highly vulnerable areas are at an increased risk for complications following hospital discharge leading to rehospitalization, which is consistent with the results presented in our study. 17
Patients discharged with long-term IV or oral therapy without the necessary transitions of care interventions can be a significant economic burden, especially for hospitals that serve a highly vulnerable area.7,12 Most of the patients in this study were insured by Medicaid. Our analysis estimated that implementing a designated pre- and post-discharge OPAT/COpAT team may have avoided costs of up to $100,000 over 3 months and reduced the number of inpatient days by 58 days. This is important as individuals residing in vulnerable areas often have financial limitations, and the delay in the ability to return to work will negatively impact their quality of life.
Our study has several limitations that should be taken into consideration. First, our study only included patients who received home-based OPAT/COpAT, and therefore our findings may not be generalizable to those discharged to receive antimicrobial therapy at a skilled nursing facility, acute rehab center, or long-term care facility. Second, most of our patients received OPAT, with just 2 of 77 patients who received COpAT. Therefore, the post-discharge complications may not reflect those who receive COpAT. Finally, the cost-saving estimates presented in our study are based on previously published literature and may not reflect the current costs, including those specific to medications, or be directly applicable to other institutions. Despite these limitations, our study provides valuable insights into the potential benefits of implementing a pre- and post-discharge ID team to assist with ID transitions of care for patients receiving home-based OPAT/COpAT programs.
Conclusion
OPAT/COpAT is a viable alternative to prolonged inpatient antimicrobial treatment. However, in the absence of an established multidisciplinary OPAT/COpAT program, there is a continued risk of antimicrobial prescribing errors and an increase in infection-related readmissions during the transition of care. Overall, we saw that the individuals living in areas of elevated vulnerability were most likely to experience adverse outcomes due to the lack of an OPAT/COpAT program, which may cause a widening health equity gap. Further research on the benefits of an OPAT/COpAT program in highly vulnerable areas is essential to guide and inform the programmatic improvements to existing models.