
Abstract
Background
Triple therapy (TT) that includes oral anticoagulation and dual antiplatelet therapy is recommended in patients who are on chronic anticoagulation and undergo percutaneous coronary intervention (PCI). The randomized clinical trials (RCTs) comparing the effectiveness and safety of TT compared to double therapy (DT), which consists of an oral anticoagulation and one of the P2Y12 inhibitors, have shown increased risk of bleeding; however, none of the individual studies were powered to show a difference in ischemic outcomes. To compare the clinical outcomes of TT and DT, we performed this meta-analysis of RCTs.
Methods
Electronic search of PubMed, EMBASE and Cochrane CENTRAL databases was performed for RCTs comparing TT and DT in patients who were on oral anticoagulation (Vitamin K antagonist or non-vitamin K antagonist oral anticoagulant) who underwent PCI. All-cause and cardiovascular mortality, myocardial infarction (MI), stroke, stent thrombosis (ST) and TIMI major and minor bleeding were the major outcomes.
Results
An analysis of 5 trials including 10,592 total patients showed that TT, compared to DT, resulted in non-significant difference in risk of all-cause [odds ratio (OR); 1.14;95% confidence interval (CI):(0.80–1.63); P = 0.46) and cardiovascular mortality [1.43(0.58–3.36); P = 0.44], MI [0.88 (0.64–1.21); P = 0.42], stroke [1.10(0.75–1.62); P = 0.63] and ST [0.82(0.46–1.45); P = 0.49]. TT, compared to DT resulted in higher risk of TIMI major bleeding [1.61(1.09–2.37); P = 0.02], TIMI minor bleeding [1.85(1.23–2.79); P = 0.003] and TIMI major and minor bleeding [1.81 (1.38–2.38); P < 0.0001; I2 = 52%].
Conclusion
Compared to DT, the patients receiving TT are at a higher risk of major and minor bleeding with no survival benefit or impact on thrombotic outcomes.
Keywords
Introduction
After percutaneous intervention (PCI), dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor is recommended to prevent stent thrombosis.1,2 Many of these patients have coexisting atrial fibrillation (AF), mechanical heart valve in place or have venous thromboembolism that warrants concomitant use of uninterrupted oral anticoagulation (OAC) with either vitamin K antagonist or non-vitamin K antagonist oral anticoagulant (NOAC) to prevent systemic thromboembolism.3–5 Therefore, taking the risk of stroke and stent thrombosis into account, guidelines suggest the use of “triple therapy” (TT) consisting of aspirin, P2Y12 (clopidogrel) inhibitor and an OAC. 6 Since this approach may result in considerable fatal and non-fatal bleeding risk,7–9 the shortest possible duration of TT followed by dual therapy (DT) comprising of single antiplatelet and OAC is usually recommended. 6 On the other hand, some studies have suggested the use of DT instead by omitting aspirin and maintaining Clopidogrel and OAC 10 to reduce bleeding complications.
Several randomized clinical trials (RCT) have studied the role of TT vs. DT in this patient population and the results have been conflicting or underpowered to assess ischemic outcomes.10–13 Therefore, to investigate the role of TT as opposed to DT on ischemic outcomes in patients who undergo PCI and have an indication for OAC use, we conducted this meta-analysis of available published RCTs.
Methods
Data sources and search strategy
We conducted this meta-analysis according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 14 We searched electronic databases of PubMed, EMBASE and Cochrane Central Register of Clinical Trials with no language restriction from inception through June 2019 using the search terms: “triple therapy” OR “triple antithrombotic therapy” AND “percutaneous coronary intervention” OR “PCI” AND “atrial fibrillation” OR “AF”. Two investigators (KD and NA) independently performed the database search and agreed on final study selection. In addition, a manual search was performed for relevant references from the selected articles and published reviews.
Study selection
Randomized clinical trials comparing the outcomes of triple therapy (defined as DAPT plus an OAC) and double therapy (defined as one of the P2Y12 inhibitors antiplatelet agent plus an OAC) in adult patients (≥18 years) who were taking chronic anticoagulation and underwent percutaneous coronary intervention (PCI) were selected for meta-analysis if they reported on major bleeding and ischemic outcomes as crude events. Studies, which were meeting abstracts and non-randomized were excluded. Additionally, studies studying triple therapy in different patient population were also excluded.
Data extraction
Two investigators (NA and HB) extracted data from the selected studies in duplicate using standardized data-extraction form, which were confirmed by a third investigator (KD). We obtained data on study characteristics (study design, patient selection, inclusion and exclusion criteria, follow-up duration, number of patients, double and triple therapy regimen and endpoints), patient characteristics (age, sex, race, co-morbidities, indication of chronic anticoagulation and PCI and medication use), and crude events on mortality, myocardial infarction, stroke, stent thrombosis and different types of bleeding at follow-up.
Outcomes
All-cause and cardiovascular mortality, myocardial infarction (MI), stroke, stent thrombosis (ST) and major and minor bleeding were the major outcomes. For uniformity among the studies, TIMI bleeding classification was used.
Statistical analysis
We performed statistical analyses with Review Manager (RevMan 5.3, Cochrane Collaboration, Nordic Cochrane Center, Copenhagen, Denmark). We calculated odds ratio (OR) with 95% confidence interval (CI) using random-effects model from the individual studies using the total number of events and patients. The studies were assessed with Cochrane Collaboration’s Bias Assessment Tools. 15 Study heterogeneity was evaluated with Cochran’s Q and I2 index with a plan to explore significant heterogeneity (I2 >50%) with sensitivity analyses. We planned pre-specified subgroup analyses based on type of OAC (warfarin-based vs. NOAC-based) and sensitivity analyses based on study design and type of antithrombotic therapy.
Results
Description of included studies
The flow diagram of study selection is shown in e-Figure 1. Electronic search of three databases (PubMed, EMBASE and CENTRAL) and manual search retrieved a total of 297 publications. After removal of duplicates, we screened 242 citations for eligibility and extracted 22 publications for full text review. Finally, we had a total of five publications10–13,16 for qualitative and quantitative analysis after excluding 17 citations for reasons as specified in the PRISMA diagram.
The individual study and patient characteristics of the included studies are shown, respectively, in Tables 1 and 2. There were 10,592 total patients (5,264 in TT arm and 5,328 in DT arm). Follow-up duration was 6–14 months. All the studies were multicenter international studies.
Study characteristics of included studies.

AF: atrial fibrillation; AFL: atrial flutter; DAPT: dual-antiplatelet therapy; DT: dual therapy; EF: ejection fraction; MV: mechanical valve; N: number; OAC: oral anticoagulation, PAD: peripheral artery disease; TT: triple therapy; VTE: venous thromboembolism.
Patient characteristics in the included studies.

TT: triple therapy; DT: dual therapy; HTN: hypertension; DM: diabetes mellitus; HLD: hyperlipidemia; PCI: percutaneous coronary intervention; ACS: acute coronary syndrome; Dabi: Dabigatran; NR: not reported.
Major outcomes excluding bleeding
TT, compared to DT resulted in similar risk of all-cause mortality [1.14 (0.80–1.63); P = 0.46; I2=46%] (e-Figure 2), cardiovascular mortality [1.43(0.58–3.36); P = 0.44; I2 = 44%], MI [0.88 (0.64–1.21); P = 0.42, I2 = 0%] (Figure 1) , stroke [1.10 (0.75–1.62); P = 0.63, I2 = 0%] and ST [0.82 (0.46–1.45); P = 0.49; I2 = 35%].

Forest plot for myocardial infarction, stroke and stent thrombosis.
Bleeding outcomes
TT, compared to DT significantly increased the risk of TIMI major bleeding [1.61 (1.09–2.37); P = 0.02; I2 = 20%] (Figure 2), TIMI minor bleeding [1.85 (1.23–2.79); P = 0.003; I2 = 39%] and combined TIMI major and minor bleeding [1.81 (1.38–2.38); P < 0.0001; I2 = 52%].
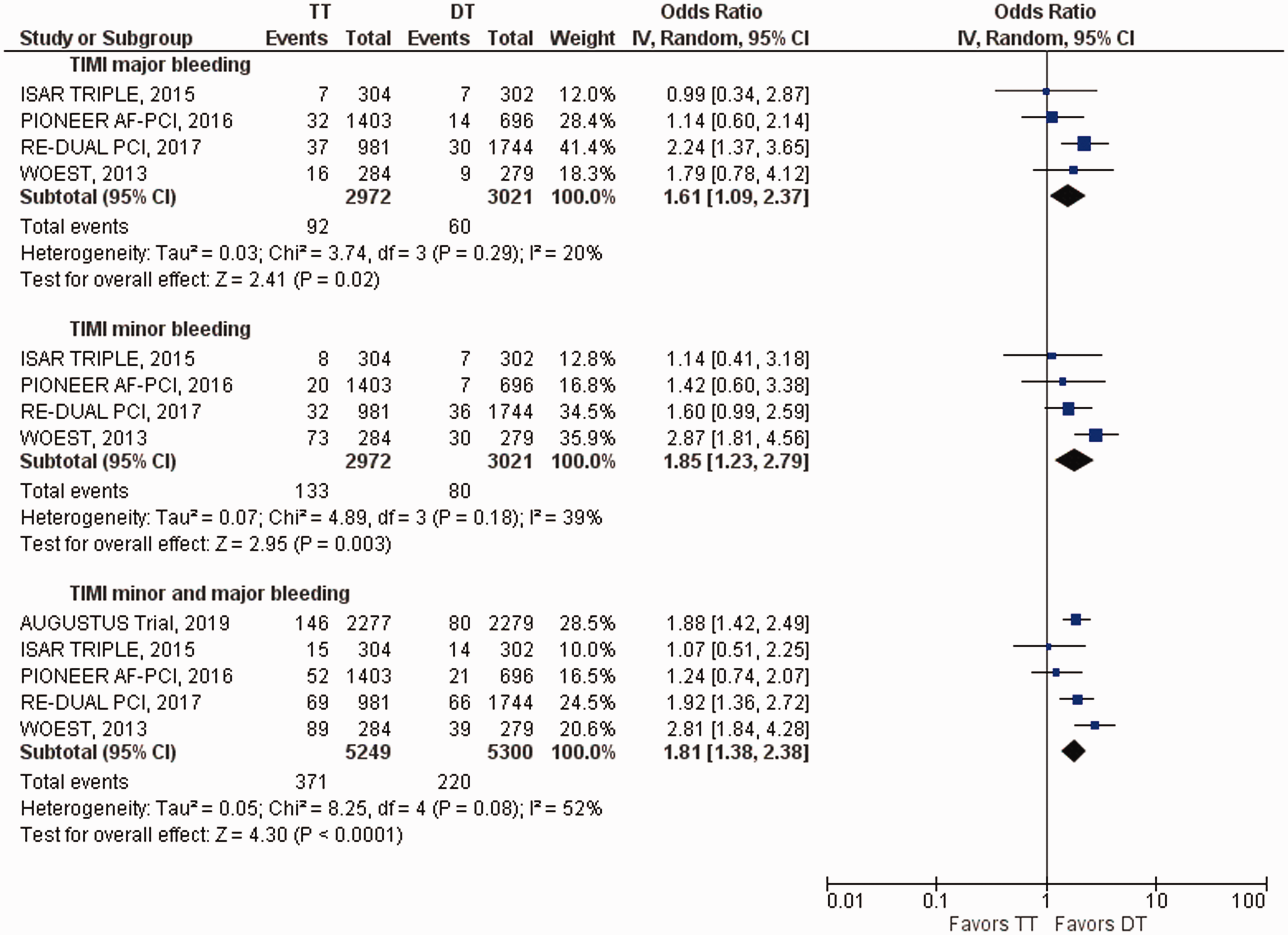
Forest plot for bleeding outcomes.
Sensitivity and subgroup analyses
Since we included the results of the landmark analysis from ISAR-TRIPLE in our primary analysis, we performed a sensitivity analysis by excluding it. There was no change in the overall direction of results. In addition, we performed analysis by excluding rivaroxaban-based triple therapy outcomes in PIONEER-AF trial as that was the only trial with such comparison. There was no change in the overall results.
Additional subgroup analyses (figures presented as online supplement) were performed for warfarin-based DT vs. NOAC-based DT. There was no significant difference in TIMI major bleeding [1.43 (0.74–2.75); P = 0.29; I2 = 0%] (e-Figure 3), TIMI minor bleeding [2.04 (0.85–4.85); P = 0.11; I2 = 61%] (e-Figure 4) or combined TIMI major and minor [1.82 (0.71–4.68); P = 0.21; I2 = 80%] between warfarin-based TT and warfarin-based DT (e-Figure 5). Compared to NOAC-based DT, warfarin-based TT resulted in significantly higher risk of TIMI major bleeding [1.93 (1.28–2.90); P = 0.002; I2 = 5%], TIMI minor bleeding [2.15 (1.40–3.32); P = 0.0005; I2 = 0%] and combined TIMI major and minor bleeding [1.83 (1.36–2.45); P < 0.0001; I2 = 0%]. On the other hand, comparison of warfarin-based TT vs. warfarin-based DT showed higher all-cause mortality [2.01 (1.06–3.79); P = 0.03; I2 = 0%] (e-Figure 6) in the warfarin-based TT group but no difference was noted in cardiovascular mortality [2.51 (0.97–6.51); P = 0.06; I2 = 0%] (e-Figure 7) between the two groups. No difference was noted in the outcomes of MI, ST and stroke in the subgroup analyses (e-Figures 8 to 10).
Study quality and publication bias
All the included studies showed bias for non-blinding of the participants and the outcomes per Cochrane collaboration’s bias tools. No bias was observed for randomization, allocation concealment, incomplete data and selective reporting. Publication bias was not tested due to small number of studies for meaningful assessment of publication bias.
Discussion
In this meta-analysis, we sought to compare “triple therapy” with “dual therapy” in patients undergoing PCI who had an indication for OAC use. We found no difference in all-cause and cardiovascular mortality, MI, stroke and ST between the groups, but the risk of bleeding was higher in patients on TT than on DT. The lack of benefits in ischemic outcomes and increase risk of bleeding were seen all four individual trials included in this analysis. Combing all randomized clinical trials potentially increased the analytical statistical power of underpowered RCTs and therefore, this meta-analysis provides insight into the overall efficacy of TT vs. DT.
The findings of this meta-analysis are similar to the result of several observational studies17–19 and published meta-analyses of those studies.20,21 An important finding of our study is no difference in thrombotic and thromboembolic events between triple and dual therapy. One hypothesis of comparable ischemic outcomes between the groups could be direct or indirect thrombin inhibition by OAC, 22 which can potentially provide cardio-protection against ischemic events/thromboembolism. Moreover, addition of OAC to antiplatelet therapy in patients with acute coronary syndrome who do not otherwise need OAC has shown to reduce ischemic events in RCTs,23–25 which can also explain possible benefit of OAC in patients with PCI when used as a part of DT. On the other hand, higher risk of bleeding with concomitant use of dual anti-platelet agents and OAC as TT has been reported in the past 26 and is well supported by our meta-analysis. It is important to note that bleeding events at follow-up in ISAR-TRIPLE were fewer in TT arm as compared to the rest of trials, which was because we only included landmark results in the analysis. However, our sensitivity analysis after excluding ISAR TRIPLE 11 showed no impact on the results. In RE-DUAL PCI trial, the use of DT lowered bleeding incidence from one quarter to one half in a dose-dependent fashion when compared to TT. 12 Stopping one of the antiplatelet agents most likely aspirin, which could cause gastric irritation and cause gastrointestinal bleeding, could explain the lower incidence of bleeding with dual therapy approach. Moreover, clopidogrel has shown to be more effective than aspirin in preventing ischemic events 27 likely from inhibiting platelet activation. 28
Our findings are in line with a recently published meta-analysis 29 which shows similarly higher rate of bleeding with TT; however, we have performed multiple subgroup analyses (e-Figures) comparing bleeding and thrombotic outcomes from VKA vs. NOAC-based OAC which provides an important information of higher bleeding from warfarin-based TT, suggesting that NOAC should be preferred when bleeding risk is high. However, due to small number of studies in the subgroup analyses, the results should be interpreted cautiously and considered hypothesis-generating at best. Furthermore, to potentially balance the risk of bleeding (based on HAS-BLED score) with prevention of thromboembolism (based on CHA2DS2VASc score), limiting the duration of TT to a shortest possible should be considered. For selected patients at high thrombotic and low bleeding risks, current guidelines recommend extending the use of TT beyond hospital discharge for up to one month followed by DT for up to 12 months. 30 In contrast, for those patients with low thrombotic and high bleeding risk, single antiplatelet agent can be discontinued after six months followed by full stroke prevention OAC dose. 30
Regardless of subgroup analyses, our meta-analysis suggests use of DT as an alternative to the TT in patients undergoing PCI who concurrently need OAC. While more randomized trials are necessary, we believe that with our findings, which are based on analysis of randomized trials, DT would be a suitable alternative to using triple therapy in this patient population.
Study limitations
The major limitation of the current meta-analysis is small number of randomized trials, which were underpowered to point a difference in thrombotic outcomes. The use of different agents in the individual trials may limit generalizability of the results. However, no significant heterogeneity was observed in the overall analyses. Lack of patient level data is another potential limitation. Due to limited data, it was not possible to perform analyses on the outcomes of ischemic vs. hemorrhagic stroke. The results of subgroup analyses should be interpreted cautiously since only two studies were available for the subgroup analysis.
Conclusion
This meta-analysis shows that compared to double therapy, patients receiving triple therapy are at a higher risk of both TIMI major and minor bleeding with no evidence of benefits on the thrombotic outcomes. Future research should focus on the appropriate combination therapy of OAC and antiplatelet therapy in this patient group.
Supplemental Material
CVD885572 Supplemetal Material - Supplemental material for Ischemic and bleeding outcomes of triple therapy in patients on chronic anticoagulation undergoing percutaneous coronary intervention: A meta-analysis of randomized trials
Supplemental material, CVD885572 Supplemetal Material for Ischemic and bleeding outcomes of triple therapy in patients on chronic anticoagulation undergoing percutaneous coronary intervention: A meta-analysis of randomized trials by Khagendra Dahal, Usman Mustafa, Sharan P Sharma, Nachiket Apte, Hari Bogabathina, Magdy Hanna, Hussam Watti, Michael Azrin, Juyong Lee, Goerge Mina, Pavan Katikaneni Kalgi Modi in JRSM Cardiovascular Disease
Footnotes
Authors’ contributions
KD took part in the study concept and design; SPS, UM, NA, HB, HW, MH, GM, HW, MA, JL, PK and KM took part in acquisition, analysis, or interpretation of data; KD and UM drafted the manuscript; SPS, UM, NA, HB, HW, MH, GM, HW, MA, JL, PK and KM were involved in the critical revision of the manuscript for important intellectual content; KD took part in the statistical analysis; SPS, UM, NA, HB, HW, MH, MA, JL, GM, PK and KM were in charge of the study supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
KD.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.