
Abstract
Poisoning with tricyclic antidepressants is an important cause of drug-related self-poisoning in the developed world and a very common cause of poisoning and mortality in developing countries. Electrocardiographic manifestations of most tricyclic antidepressant-poisoned patients resolve by the administration of 1–2 mEq/kg of sodium bicarbonate. Some rare cases have been reported who have been resistant to the long-term or high doses of bicarbonate administration. We present a case of acute tricyclic antidepressant toxicity referring with status epilepticus, hypotension, and refractory QRS complex widening that resolved after the intravenous administration of 2650 mEq sodium bicarbonate.
Introduction
Poisoning with tricyclic antidepressants (TCAs) is an important cause of drug-related self-poisoning.1,2 Electrocardiographic (ECG) manifestations of most TCA-poisoned patients resolve by the administration of 1–2 mEq/kg of sodium bicarbonate. 3 Some rare cases have been reported who have been resistant to the long-term or high doses of bicarbonate administration. 4 We present a case of acute TCA toxicity referring with status epilepticus, hypotension, and refractory QRS complex widening that resolved after the intravenous (IV) administration of 53 vials sodium bicarbonate.
Case history
Reed coma scale measurement in the poisoned patients.

The patient’s vital signs were as follows: blood pressure = 100/60 mmHg, pulse rate = 84 bpm, and respiratory rate = 28/min. The pupils were mydriatic and reacted sluggishly. The patient was immediately intubated, and gastric lavage was performed. Wide QRS complexes (400 ms) were confirmed on 12-lead ECG. A bolus dose of sodium bicarbonate (150 mEq) was administered, and a maintenance dose (50 mEq/h) was ordered. In the first arterial blood gas analysis (ABG; after the administration of the loading dose of bicarbonate), pH, pCO2, and HCO3 were 7.40, 48.5 mmHg, and 29.5 mEq/L, respectively. His initial serum sodium and potassium levels were 141 and 3.8 mEq/L, respectively.
The patient was admitted to intensive care unit (ICU) and on the second ECG, he still had wide QRS complexes. Another loading dose of 150 mEq bicarbonate was administered without any change in the patient’s ECG. The patient experienced a generalized tonic–clonic seizure and received 10 mg of IV diazepam. The seizure subsided but restarted 5 min later without any improvement in the patient’s level of consciousness during that interval. IV diazepam was again administered with the dose of 10 mg. However, the patient’s seizures restarted about 4–5 min after the administration of benzodiazepines. After IV administration of 40 mg of diazepam and 40 mg of midazolam, he still had convulsions. Phenobarbital was loaded (1200 mg) followed by 3 mg/h which kept the patient seizure-free till the end of ICU stay. Loading doses of bicarbonate were repeated every 3–5 min to reach a narrow QRS. After administering a total dose of 35 vials (50 mL) of bicarbonate 8.4% (about 2.5 h after ICU admission), the patient’s QRS complexes were still wide (360 ms). In the ABG performed, pH was 7.66. Bicarbonate was therefore held. Meanwhile, the patient received IV hypertonic saline (2 mEq/kg), IV MgSO4 (2 g stat and 1 g QID, afterwards), and IV intralipid 10% (2 cc/kg IV loading dose followed by 0.5 cc/kg/h IV drip for 4 h). Serum sodium level was reported to be 144 mEq/L when hypertonic saline was initiated. He also had a low blood pressure at this time (85/50 mmHg) that responded to 5 µg/min of norepinephrine.
Although the QRS complexes were still wide (160 ms (Figure 1; left)), we did not administer additional bicarbonate because of the high pH. Serum sodium of 155 and HCO3 of 51.9 were detected by the end of the first day of admission which was treated by free water gavage.
The patient’s ECG before (left) and after (right) the completion of the treatment.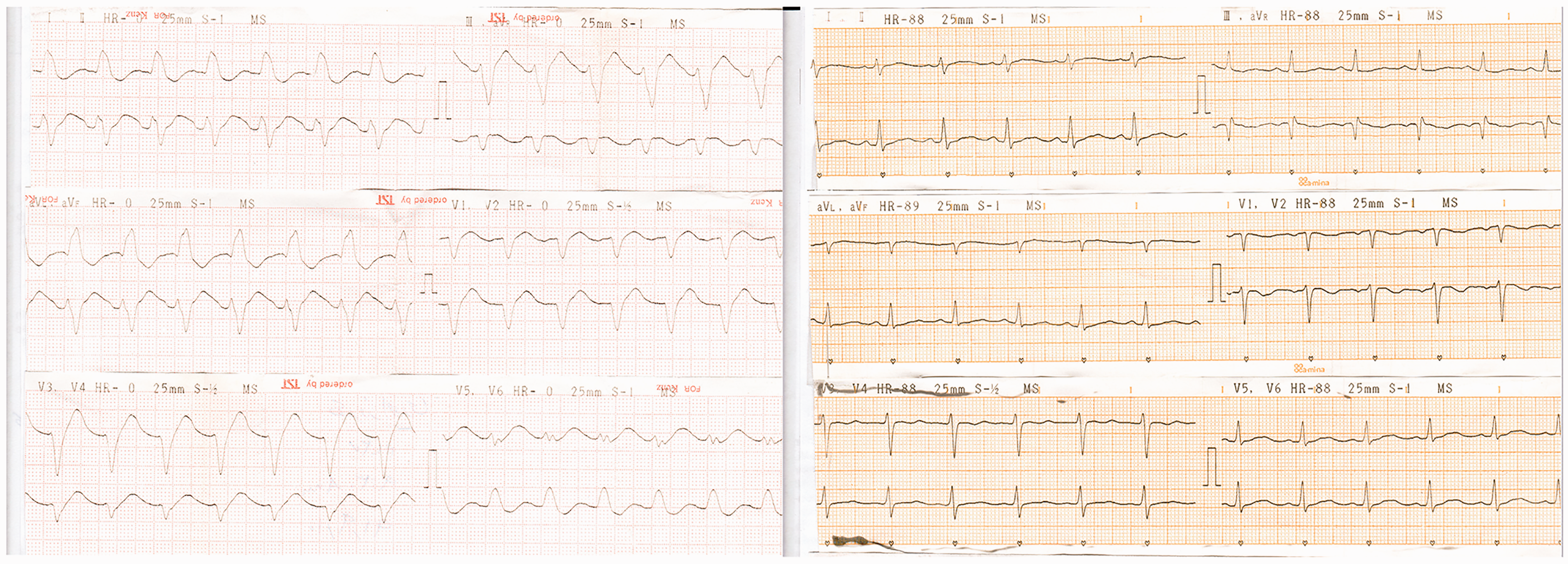
On the second day, QRS complexes were still wide and pH had normalized (7.43). Sodium bicarbonate was again started. After administering 900 mEq of bicarbonate (2650 mEq in total), QRS became narrow (120 ms) (Figure 1; right). By the end of the second day, serum sodium was 141 mEq/L, QRS was narrow, and pH was normal (7.42). One day later, phenobarbital drip was stopped. The patient became conscious and remained in the ICU for another day without receiving bicarbonate. After transferring to the ward, he stayed in the ward for another day and was finally discharged seven days after hospital presentation completely symptom-free. A written permission was taken from him letting publish the data anonymously.
Discussion
As shown, it seems that the main treatment of TCA poisoning-induced cardiotoxicity remains to be sodium bicarbonate. Although the current study only defines a case, has low power of evidence, and this is definitely a limitation of it, step by step precise follow-up of the patient is a strength. TCA-poisoned patients generally experience grave cardiovascular toxicity with doses higher than 10–20 mg/kg. An oral ingestion of 1 g is often considered to be fatal. Patients with prolonged QRS complex are recommended to be treated by 1–2 mEq/kg IV boluses of bicarbonate at 3- to 5-min intervals to reverse the ECG abnormality. In more severe cases, hypertonic saline (3% NaCl; 1–2 mEq/kg followed by additional doses every 3–5 min), magnesium sulfate (25–50 mg/kg (maximum 2 g) IV over 2 min), and lidocaine (1 mg/kg slow IV bolus followed by infusion of 20–50 µg/kg/min) are recommended. 4
Patients with resistant QRS widening who needed large doses of bicarbonate or prolonged bicarbonate administration have previously been reported. 4 This case is interesting because of a mixed resistant ECG to the conventional doses of bicarbonate and his neurologic features characteristic of status epilepticus as well as hypotension. The patient had status epilepticus and, therefore, we preferred not to put him on IV lidocaine. He had experienced hypernatremia (Na = 155 mEq/L) after we had only administered the loading dose of hypertonic sodium and thus, we had to hold additional maintenance doses. We continued to administer sodium bicarbonate to our patient whenever his pH was acceptable enough. This is probably the key point in the successful management of this patient.
Intralipid infusion was able to decrease tachycardia that recurred shortly after the infusion was stopped in a case. 5 In our patient, no improvement was observed in the patient’s ECG even when the intralipid was being infused. This, however, may be because we used intralipid 10% and not 20%.
Conclusion
Sodium bicarbonate is perhaps the treatment of choice in TCA poisoning especially when other treatment modalities are not applicable. In such cases, the treatment can be held when there are contraindications to bicarbonate therapy (for instance pH > 7.55) and restarted when the contraindication has resolved. Meanwhile, administration of other adjunctive therapies is advocated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
None.
Guarantor
HHM is the guarantor for all the content presented in this paper.
Contributorship
Data collection – Hassan Amiri, Nasim Zamani Figure – Hossein Hassanian-Moghaddam, Nasim Zamani. Draft – Nasim Zamani, Hossein Hassanian-Moghaddan. FINAL PAPER APPROVAL – Nasim Zamani, Hossein Hassanian-Moghaddam, Hassan Amiri, Shahin Shadnia.