
Abstract
Objective
The aim of this study is to assess the feasibility (uptake, retention and adherence) and acceptability of a combination of smartphone apps to deliver a digitized safety plan, BeyondNow, and personalized management strategies, BlueIce, with adolescents discharged from a mental health inpatient ward following self-harm, suicidal ideation and/or behavior.
Methods
Participants in this pre-post pilot study included 20 adolescents between 13–18 years, presenting with self-harming or suicidal behaviors in an inpatient psychiatric ward at a tertiary pediatric hospital. Participants were familiarized with the apps and completed baseline measures prior to discharge. They used the apps for six weeks before completing the follow-up survey, which measured feasibility and acceptability of the apps, as well as suicide resilience.
Results
Seventeen participants completed the pilot. Most of the sample accessed both apps at least once, three accessed the BeyondNow safety plan five times or more, and six used the BlueIce toolbox five times or more. A total of 73.5% of the sample that experienced a crisis used at least one of the apps at least once. Forty seven percent felt that the apps would not keep them safe when in crisis, although almost all of the sample rated both apps as easy to use (94% for BeyondNow, and 82% for BlueIce). Medium to large effect sizes were also found with regard to improvements in suicide resilience.
Conclusion
Both apps were found to be feasible and acceptable in this population, and easy to use, although no conclusions can be drawn regarding the clinical efficacy of the apps.
Introduction
Levels of suicide and self-harm are of significant concern throughout adolescence, 1 with the risk for self-harm 2 and death by suicide 3 increasing dramatically from childhood levels during this developmental period. For young Australians aged 16 to 24 years, 22% of all deaths in this age group were due to suicide in 2009, 4 which is consistent with suicide being the second leading cause of death globally in young people aged 16 to 29 years. 5 Although there has been some success in characterizing suicide and self-harm risk factors in adolescents,1,6 there are gaps in the literature regarding the efficacy and acceptability of interventions with this population. 7 Studies of adherence with follow-up treatment in adolescents who attempt suicide have found that only 30% adhered to referral recommendations.8,9 Of great concern, previous research has also found that between 16% and 60% do not engage in further support following a suicide attempt.10,11 For adolescents hospitalized for acute suicide risk, the transition from an inpatient level of care to a less restrictive environment represents a period of elevated suicide risk. 12 One type of intervention that may assist to mitigate suicide risk and self-harm during this transition period, is the safety planning intervention. 13
Safety plans
Safety planning intervention involves a collaborative approach between the clinician, the patient and their parents to develop a set of strategies to increase self-help and help-seeking behaviors when in a suicidal crisis. 13 Safety plans may be useful in supporting individuals who do not, or cannot, readily engage with mental health services, 13 with recent research finding that the use of safety planning reduces suicidal behavior following discharge, and improves the likelihood of engagement in outpatient mental health services following the transition from inpatient care. 14 Safety plans consist of a number of components including: a) the recognized warning signs of an impending suicidal or self-harm crisis; b) a list of coping strategies that the individual can engage in on their own in the crisis; c) a list of social contacts or social places to visit in order to distract from suicidal or self-harming thoughts; d) a list of family members or friends who may help resolve the crisis; e) a list of mental health professionals, agencies, or emergency services they can contact; and f) removal of access to potentially lethal means.13,15,16 Safety plans are considered to be adaptable documents, that are shared with parents and professionals who are involved in the care of the adolescent, with the document modified and updated over time, depending on which strategies are helpful and which are not. 17
Digital interventions for suicide and self-harm prevention
Safety plans are traditionally completed on paper, which has some disadvantages. It may be inaccessible or misplaced, 18 which can result in the plan not being available when a crisis arises. Portability and accessibility are factors which may contribute to safety-plan engagement, particularly among youths. 19 Safety plans delivered through a smartphone application (app) may be more effective than paper versions, as they are more readily accessible and can be easily modified and adapted over time. Mobile phone apps also provide the opportunity to deliver coping strategies and distractors that are engaging, highly tailored to the individual, and accessible during crisis.
Since apps are cost-effective, convenient, discreet and are frequently used by adolescent populations,19,20 they represent a promising, modern approach to extend and/or complement traditional interventions. Furthermore, recent surveys estimate that 91% of Australian youth own a mobile phone, and 94% of this group are using smartphones, 21 suggesting young people may be receptive to digital interventions.
The World Health Organization recommends mobile devices as an option for providing support and therapy to people at risk of suicide. 5 Larsen et al. 22 also suggest that access to high quality mobile devices can potentially reduce injury and death. As self-harm and suicide urges can fluctuate and be relatively short lived, apps offer the ability to deliver timely support and intervention in situ, at the time of crisis. Furthermore, smartphone app interventions may be more engaging than traditional therapies for young people. Studies in emergency department settings 23 and inpatient psychiatric units 24 suggest that adolescents prefer technology-based interventions and are interested in using apps for their mental health.
Digital safety plans in adolescents
Despite a recent burgeoning of apps for self-harm and suicide prevention, 22 few have been empirically evaluated, or have data to support their effectiveness. 25 The BeyondNow safety planning smartphone app was recently developed, 26 based on the original pencil and paper version of the Safety Plan Intervention. 13 It provides an online platform for users to create and edit their safety plan, and share it with family, friends and clinicians. It allows individuals to list their coping strategies, their warning signs or triggers, their reasons to live, ways to limit their access to lethal means, and the contact numbers of people in their support network. An early study explored the feasibility of integrating BeyondNow into a tertiary mental health service for adolescents and adults. This study found its implementation to be feasible and acceptable, with the majority of 16–42 year old participants reporting that they accessed their digital safety plan, and that it was easy to use. 26 Reductions in suicide related coping were found after eight weeks, however no significant improvement in suicide resilience were observed. 26
Complementing the BeyondNow safety plan, BlueIce was specifically designed to reduce self-harming behaviors, and aimed to maximize user engagement by providing an interactive personalized toolbox of strategies. These strategies are based on current evidence and best clinical practice in cognitive behavioral therapy and dialectical behavioral therapy, 27 with BlueIce endorsed as an evidence-based app by the National Health Service in the United Kingdom. BlueIce includes a mood diary, a menu of personalized mood-lifting activities (e.g. uploading uplifting music and photos, mindfulness and relaxation activities), and automatic routing to delay and preventative strategies when risk of self-harm is reported.28–30 In addition, if these tools have not reduced the urge to self-harm, the young person is automatically directed to emergency numbers. A preliminary evaluation of BlueIce was recently conducted in the United Kingdom, including 12–17 year olds with a history of self-harming behaviors, and who were attending child and adolescent mental health services. A total of 88% found the app to be engaging, and wanted to keep using it at the conclusion of the study. 29 The study also documented an improvement in symptoms of depression and anxiety after using the app for 12 weeks in an outpatient setting.29,30
Despite these early promising findings for the BeyondNow and BlueIce apps, it remains unclear as to whether these interventions would be feasible and acceptable in a pediatric inpatient mental health setting, with young people who may be difficult to engage, and are experiencing extreme, and often longstanding and chronic mental health problems. The purpose and features of these two apps are very different, with the BeyondNow app providing online access to a safety plan that is used in clinical treatment of suicide risk, and the BlueIce app containing a suite of strategies, activities and tools that can be used in conjunction with the safety plan to support young people during a crisis, and in the lead up to a crisis. The current pilot study therefore aims to assess the feasibility (uptake, retention and adherence) and acceptability of both apps used in conjunction. Specifically, assessing the use of a digitized safety plan, delivered through the smartphone app BeyondNow, and a personalized toolbox of strategies delivered through the smartphone app BlueIce, with adolescents discharged from a pediatric inpatient mental health unit following self-harm and/or suicidal acts. A secondary aim was to explore any clinical benefits of using the apps, specifically suicide resilience and self-harming behaviors.
Methods
Study design
This pilot study evaluated the feasibility and acceptability of using a safety planning smartphone app (BeyondNow), and a personalized digital toolbox of strategies (BlueIce) for young people who presented to a pediatric inpatient mental health ward with suicidal behavior and/or self-harm. Participants completed a baseline questionnaire during their admission to a mental health ward, when they also had their safety plan and digital toolbox uploaded onto their phones. They then completed a follow up questionnaire 6 weeks later. Feasibility was measured using recruitment rate, participant retention in the study, and adherence to the intervention (log in and use of the apps during this period). Acceptability was measured using a self-report questionnaire exploring participants’ level of use, engagement and satisfaction. The study was approved by the Royal Children’s Hospital Human Research Ethics Committee (HREC 38169A).
Setting and sample
Young people were recruited from the inpatient mental health ward (‘Banksia’) at The Royal Children’s Hospital, Melbourne, following an admission involving self-harm and/or a suicidal act or ideation. Banksia accommodates children aged between 12–18 years who require in-patient treatment for serious mental illnesses and severe behavioral problems.
Participants included adolescents aged 13 to 18 years admitted to Banksia following a suicide attempt or ideation and/or engagement in self-harm within 30 days prior to the admission. Young people were excluded if they had a diagnosis of acute psychosis, substance dependence, a learning disability and/or a severe autism spectrum condition, as these conditions may have impaired their capacity to provide informed consent and/or use the apps. Involuntary patients were also excluded, as were young people who were not proficient in English, those who did not own a smartphone, and those that had an Aboriginal cultural background. This final criterion was important to include as this population is provided services and interventions that are culturally sensitive and specific.
Intervention
Measures
Feasibility
Feasibility was measured using the recruitment rate, participant retention in the study, and adherence to the intervention. As defined by the CONSORT 2010 statement, recruitment of 30%, retention of greater than 80% and adherence of 90% to the intervention indicated feasibility, 33 with adherence being the percentage of participants that use the apps when needed post-discharge.
Acceptability
Acceptability was measured at the 6-week follow-up time-point using a self-report questionnaire designed specifically for this pilot study. This questionnaire measured participants’ level of use, engagement and satisfaction. Participants were asked to rate their agreement with a series of statements about both apps independently. Questions included “In the past month, how many times did you look at the app?”, “In the past month, how many times did you change/update the app?” and “In the past month, during a crisis, how many times did you use the app?”. Participants were also asked to rate on a 10-point Likert scale (1 = not at all, 10 = very much so) how much they thought the apps kept them safe from harming themselves, how useful the apps were in managing their symptoms during a crisis, and how much they liked and used the apps. A 5-point Likert scale was also used to rate ease of use, whether they would recommend the app to a friend, and overall satisfaction, with scores of 4 and 5 (above a neutral score) considered to be positive with regard to acceptability.
Suicide Resilience
The adapted Suicide Resilience Inventory-25 (SRI-25), 34 is a 25-item measure used to assess an individual’s perceived resources and ability to manage thoughts and feelings associated with suicide. The SRI-25 comprises three scales: Internal Protective Scale (internal protective thoughts and attitudes associated with suicide), Emotional Stability Scale (the capacity of an individual to regulate their emotions in crisis) and External Protective Scale (the perceived support available to them from those around them). These scales are combined to generate a Total Score of suicide resilience. Items are rated on a 6-point Likert scale, ranging from 1 (strongly disagree) to 6 (strongly agree), with a higher score indicating higher level of suicide resilience. For this pilot study, the wording of the items were adapted slightly to incorporate an assessment of factors helping to manage self-harm as well as suicidal thoughts (e.g. “Ï can resist thoughts of ending my life when I feel emotionally hurt” was adapted to “I can resist thoughts of hurting myself or ending my life when I feel emotionally hurt”). The SRI-25 was completed at the baseline time-point prior to discharge and was again completed at the post-intervention time-point 6 weeks later.
Self-harm
To measure the frequency of thoughts and acts pertaining to self-harm with or without suicidal intent, participants completed two self-report items. These items asked how often they had thought about harming themselves on purpose during the past month, and how often they had actually hurt themselves on purpose in the past month. These questions were completed at baseline and at the six week follow-up. Information regarding their recent self-harming and suicidal behaviors was also collected at baseline, including the method of self-harm and/or suicide attempt prior to admission, previous contact with mental health services and whether they were taking psychotropic medication.
Procedure
Following a daily review of newly-admitted Banksia referrals by a clinician, patients were screened for study suitability using the hospital electronic medical record. Once eligible participants were identified, a member of the research team approached the young people and their parents, and provided information about the study. Participants were recruited in the study once both the young person and their parent/caregiver provided informed written or electronic consent. Prior to being discharged, consenting participants completed a brief baseline questionnaire, completed via pencil and paper, or electronically via an iPad. Participants were then given access to their smartphone and researchers supported the young person by guiding them through how to download, set up and interact with the two apps. All participants were given access to both apps. As in usual practice, clinicians were responsible for developing the hard-copy safety plan with the young person for them to utilize following discharge. In collaboration with clinicians and the young person, researchers assisted with transferring details from this paper-version safety plan to the BeyondNow app, and were guided on how to use the personalized toolbox of strategies delivered through the BlueIce app. Six weeks following discharge, the participants were asked to complete the post-intervention questionnaire, which was sent electronically either via SMS or email.
Statistical methods
Given the primary aim of the study was to evaluate the feasibility of using the BeyondNow and BlueIce apps, formal power calculations were not required. Data from participants who consented, participated, and completed measures at baseline and at the six week follow-up were included in the analyses. Only participants with complete datasets were included in analyses.
The primary analysis involved descriptive statistics regarding the feasibility and acceptability of the intervention. Repeated measures t-tests explored differences in self-harm and suicide resilience between the pre- and post- intervention time points. Given the small sample size and the study design, clinical effectiveness was not able to be assessed in this pilot, hence effect sizes (Cohen’s d) were also included in the analyses, and were interpreted as small < 0.2, medium > 0.2–0.5, large=>0.5–0.8, very large >0.8. 35
Results
Figure 1 outlines the participant recruitment flow. Over a four-month period (May to August 2019), a total of 83 young people were screened for eligibility, with 69.9% (58/83) satisfying inclusion/exclusion criteria. The main reasons for exclusion included involuntary inpatient status and having acute psychosis or substance dependence. With regard to the recruitment rate, a total of 24 out of 58 eligible young people and their parents consented to participate (41.4% of total eligible participants), with 21 (36.2%) discharged prior to consenting to participation, and 10 (17.2%) declining consent. Twenty consented young people completed the baseline measures, with three of those lost to follow-up prior to completing the post-intervention time-point six weeks later (85% retention rate). There were no significant differences between the young people that consented, and those that were eligible but declined to participate, with regard to age, sex, and suicidal and self-harming behaviors at admission. Similarly, there were no significant differences between participants that consented and completed the study, and participants that consented and withdrew following baseline survey, on the same measures. Participant characteristics and demographics can be seen in Table 1. The ages of the participating adolescents ranged from 13 to 18 years. Most had engaged in suicidal behaviors, were on psychotropic medication, and had accessed mental health services prior to admission.
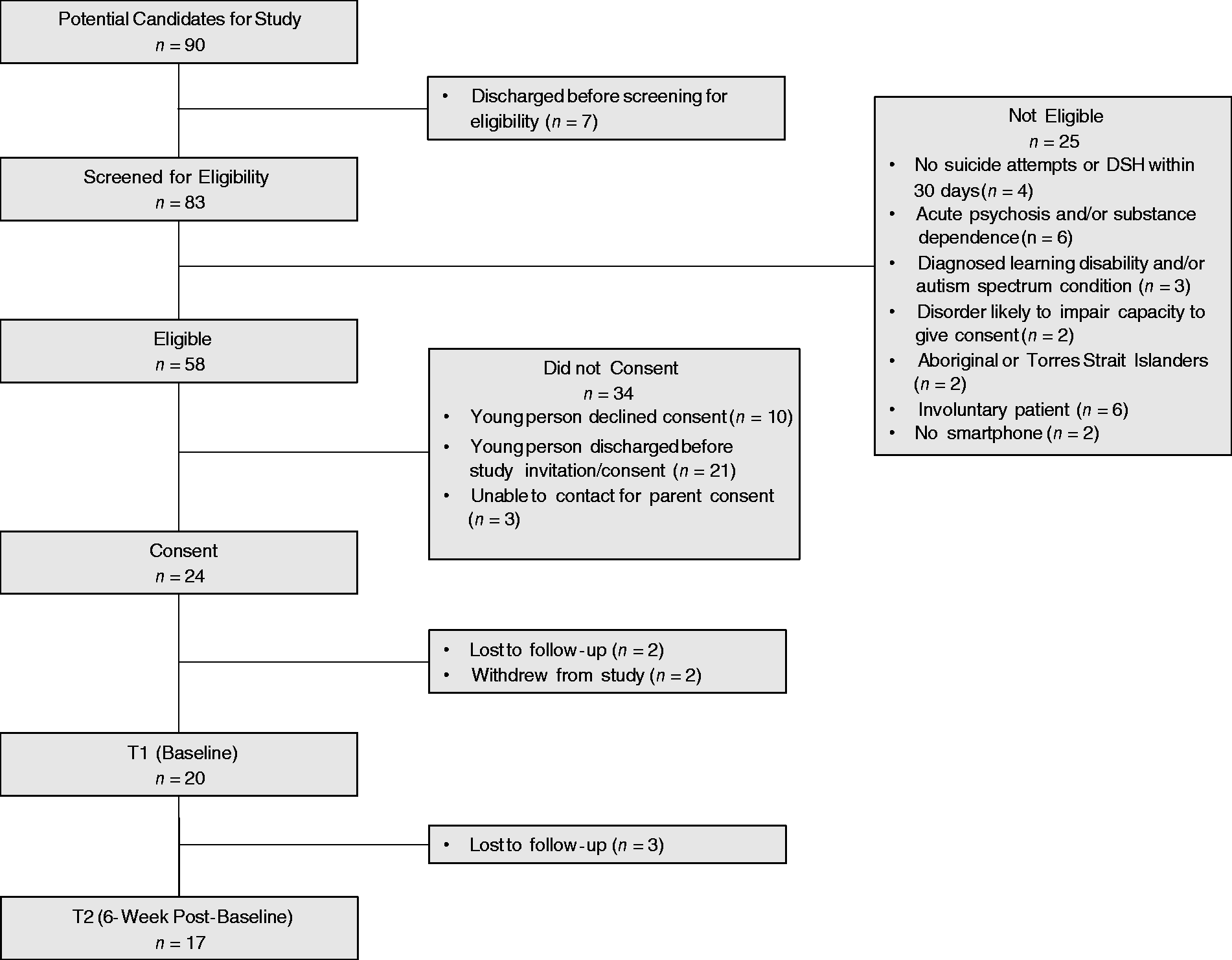
The recruitment flow of participants.
Participant characteristics (n = 20).

aRefers to behaviors engaged in within the month prior to admission.
bRefers to the most extreme form of suicidal behavior exhibited.
Table 2 displays the reported general access and usage of the BeyondNow and BlueIce apps, following discharge. The majority of the sample accessed the apps at least once, with three accessing the BeyondNow safety plan five times or more, and six using the BlueIce toolbox five times or more. Only four edited their safety plan or toolbox, however most importantly, most of the sample that experienced a crisis used both apps, with 73.5% of the sample using at least one app (adherence rate).
Use of the BeyondNow safety plan and BlueIce toolbox apps (n = 17).

The usefulness of the apps within times of crisis is reported in Table 3. Eight felt that the apps would not keep them safe when in crisis, with nine and seven reporting that BeyondNow and BlueIce, respectively, did not help them to manage their symptoms in crisis. Further acceptability measures of the apps can be seen in Table 4. It was found that most participants rated both apps positively with regard to ease of use, and a small majority reported that they would recommend both apps, and were satisfied with the apps. The majority of participants did not, however, believe that they would use the apps in the future.
Usefulness of the BeyondNow safety plan and BlueIce toolbox apps in crisis.
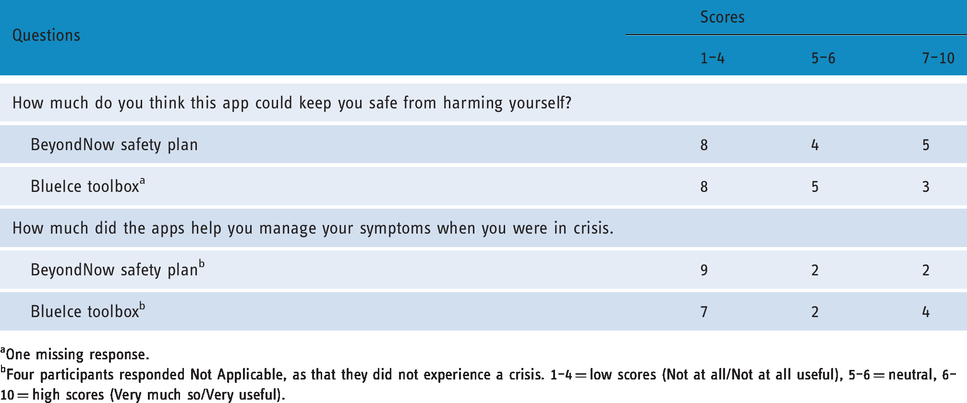
aOne missing response.
bFour participants responded Not Applicable, as that they did not experience a crisis. 1–4 = low scores (Not at all/Not at all useful), 5–6 = neutral, 6–10 = high scores (Very much so/Very useful).
Acceptability of the BeyondNow safety plan and BlueIce toolbox apps.

aRange of scores: 1 = not at all, 5 = very much so).
bscores of 4 or 5, which were above neutral;.
A secondary aim in this pilot study was to explore whether any changes in suicide resilience and self-harming behaviors were able to be detected six weeks following discharge. With regard to suicide resilience as measured by the SRI-25, a significant improvement was found on the Emotional Stability Scale t(32) = −2.08, p = 0.045, with medium to large effects found across all scales, and for the total suicide resilience level. These findings are displayed in Table 5.
Differences in suicide resilience (SRI-25) and self-harm behaviors from baseline to 6 weeks post-discharge.

*p <.05.
Discussion
The current study explored the feasibility (uptake retention and adherence) and acceptability of implementing a digitized safety plan, delivered through the BeyondNow safety plan app, and the BlueIce toolbox app, with adolescents discharged from a pediatric inpatient mental health unit following self-harm and/or suicidal acts. Overall, both apps were found to be feasible and acceptable, with the majority of participants using and accessing the apps in the six weeks post-discharge.
The use of both apps was found to be feasible, with an 85% retention rate, and a recruitment rate of 41.4% of all eligible participants. This indicates that this intervention is clinically feasible, as is a future trial of these apps in this population. About 29.4% did not experience a crisis in the six weeks following discharge, however of those that did experience a crisis, 73.5% used at least one of the apps. Although this adherence rate (73.5%) is below the 90% required to indicate high feasibility for this study, it is nevertheless a critical finding given that this is a difficult to engage population, both within inpatient and outpatient settings. This indicates a high level of interest and engagement with the study, and with the treatment.
Both apps were also found to be acceptable. The majority of participants accessed both apps at least once following discharge, with most also using it during crisis. This population can be difficult to engage clinically, and often disengage from services and support post-discharge. This suggests a high level of engagement with the apps, with some also editing and updating their safety plan and toolbox in a relatively short six week timeframe. In addition, most participants rated the apps as being easy to use, with a small majority indicating that they were satisfied with and would recommend the apps to others, again suggesting they were acceptable.
These findings are consistent with previous research examining the feasibility, acceptability and usability of smartphone apps, as an adjunct to usual intervention, in individuals receiving treatment in tertiary mental health services.19,26,28–30 With regard to the specific apps examined in this study, previous studies have found BeyondNow was a feasible and acceptable intervention with the 16–42 year old participants, suggesting that it has potential for inclusion in clinical pathways within a tertiary mental health service for older adolescents and adults. This previous study also found BeyondNow was easy to use, 26 similar to current findings. This also provides further weight to a recent study which also found BlueIce to be engaging and useable, as well as acceptable and feasible for use with 12–17 year old young people attending outpatient child and adolescent mental health services with a history of self-harming behaviors.29,30
Despite the acceptability and level of use and engagement with the apps, the majority of participants reported that they did not believe, or were not sure whether the strategies within the apps could keep them safe from harming themselves, or helped them manage their symptoms in crisis. Importantly, this indicates that these app were engaging, even if they did not necessarily believe it could prevent future self-harming acts. This was not a surprising finding given that the purpose of these apps was not to function as an isolated intervention to manage suicidal and self-harming behaviors in this complex cohort. Rather, they are intended to be a clinical tool or strategy to support these high risk young people, to be used in conjunction with other clinical intervention, including face-to-face support. This indicates that, for a proportion of this complex adolescent sample, these apps are engaging and can be used as an adjunct to face-to-face clinical treatment following discharge. Further research that examines the amount and type of content in a participant’s safety plan may aid understanding of why some believed that their plan could not keep them safe. These ratings were also consistent with the finding that only 35% believed that they would use the apps in the future. This supports previous research which has found that this population has limited adherence with follow-up treatments and referrals, and are difficult to engage.8–11 However, it is possible that for some, their presenting issue may have resolved or improved, thus there being no perceived need for the apps. Despite the reported limited future use of the apps, the majority felt that they were easy to use, and over half were satisfied with both apps, suggesting that they were seen as acceptable, engaging and user-friendly.
The current study also explored the potential clinical impacts of using the apps. It was found that there was a statistically significant improvement in perceived emotional stability factors when in crisis, with medium to large effect sizes found on the other scales in the measure. The direct impact, however, of the apps on suicide resilience and self-harming behaviors is not able to be determined, due to there being no control group and a lack of documentation of other therapeutic services received during the follow up period. A larger controlled trial is needed to determine the clinical benefits of these apps, and whether different clinical or technological approaches are required to engage young people in their treatment, and improve clinical outcomes. The health economic benefits of using these apps, as well as potential reductions in hospital admissions as a result of their use also need to be explored.
Clinical implications
These preliminary results are promising, and suggest that these apps may support the treatment of adolescents requiring inpatient treatment for suicide risk and self-harm. This population can be difficult to engage clinically, and often disengage from services and support post-discharge.8,9,11 Hence providing these apps as an adjunct to therapeutic services facilitate timely support and accessible information when in crisis, and have the potential to prevent some admissions in pediatric emergency departments, and inpatient mental health services. Despite these findings, ratings regarding satisfaction, comfort of use and likelihood of recommending to others were lower than expected. Further research exploring which aspects or features of the apps could be improved is warranted to improve the potential for future clinical implementation.
Improvements were also detected in the emotional stability and resilience to manage thoughts about self-harm. Although caution must be taken in interpreting these results, these improvements in suicidal and self-harming behaviors are promising in a high risk population that is difficult to engage, but cannot be wholly attributed to the apps as participants also received other interventions in parallel. Future research should examine whether these digital tools provide greater consistency in mental health care and treatment, during episodes of care from emergency, inpatient and outpatient mental health services.
Limitations
Caution must be taken when interpreting these findings, due to some study limitations. Firstly, the small sample size and lack of control group limit the confidence with which we can draw conclusions. It is possible that improvements in suicide resilience may have occurred via natural recovery, and/or due to the engagement with outpatient mental health services. Nevertheless, these improvements in suicidal and self-harming behaviors are promising, with greater research required to examine the impact that these apps have on reduction to self-harming thoughts and behaviors.
The study design was also limited by the reliance on clinical staff to recruit young people and assist with the study enrolment process, with not all clinicians engaged with the study. This impacted recruitment and success of downloading the apps onto phones when participants were keen to be involved in the study. These challenges are common and reflect clinicians’ caution regarding digital mental health support.36,37 As adolescents admitted to in-patient mental health services are often resistant to treatment, clinician engagement plays a crucial role in successfully providing these apps as an adjunct to therapeutic services. Finally, the current study examined the feasibility and acceptability of two apps which have different purposes and functions, and so the individual benefits of each cannot be determined.
Conclusions
We explored the feasibility and acceptability of the BeyondNow digital safety plan app, and the BlueIce personalized toolbox of strategies, with inpatients in a pediatric mental health hospital ward. Although no conclusions can be drawn regarding clinical efficacy in this pilot study, medium to large effects were found with regard to improved suicidal resilience and reduced self-harming behaviors, and they were both found to be feasible and acceptable in this population, and easy to use.
Footnotes
Acknowledgements
We acknowledge the generosity of the participating young people and families as well as the valuable support of the clinical staff within the Banksia Ward of the Royal Children’s Hospital.
Contributorship
FM, ON, LC, SL, GM, VA, CP were involved in the design of the study. FM, ON, LC, SL, LK, GM, SG, VA, CP were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. FM, ON, SL, LK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and standards
The study was approved by the Royal Children’s Hospital Human Research Ethics Committee (HREC: 38,169 A). The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and international committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. No professional writers were involved in writing this manuscript.
Funding
We acknowledge the generous funding support for this project from the Royal Children’s Hospital Foundation and the Victorian Government's Operational Infrastructure Support Program. The research project reported in this published work was conducted by the authors as part of their employment or placement with the Murdoch Children’s Research Institute and The Royal Children’s Hospital, Melbourne, Australia.
Guarantor
FM.
Peer Review
Dr. Shirley Yen, Harvard Med School has reviewed this manuscript.