
Abstract
Elderly patients are particularly vulnerable to look-alike/sound-alike medication errors due to physiological differences that alter medication pharmacokinetics and pharmacodynamics. This report presents the case of a 70-year-old woman admitted to the emergency department in an unconscious state. The information provided by the patient’s family suggested a potential unintentional amitriptyline overdose due to confusion with berberine—a plant-derived over-the-counter antidiarrheal medication of similar appearance and packaging. Examination of the remaining amitriptyline tablets indicated the patient had likely consumed 19 tablets of 25 mg amitriptyline. This suspicion was supported by an electrocardiogram showing QRS widening to 110 ms and tachycardia. Following serum alkalization therapy with sodium bicarbonate, the patient’s consciousness improved, her heart rate normalized, and QRS duration was shortened. This case underscores the importance of involving healthcare providers and family members in implementing robust safety measures to prevent unintentional medication errors caused by look-alike/sound-alike medications, particularly among older adults.
Introduction
Medication safety is a critical concern in the elderly population as they are particularly vulnerable to adverse drug events, which may include unintentional overdoses. As older adults often manage multiple chronic conditions, they tend to use complex medication regimens, which increase the risk of medication errors.1,2 Additionally, age-related physiological changes, such as an increased proportion of body fat and reduced renal and hepatic clearance, can alter drug pharmacokinetics and amplify the effects of even a modest overdose, which may lead to severe toxicity. 3 Furthermore, cognitive decline, impaired vision or hearing, reduced health literacy, care provided by multiple health professionals with limited coordination, and the iso-appearance of certain medications often contribute to medication errors in elderly patients. 4 This case report describes a 70-year-old female who mistakenly consumed 19 tablets of amitriptyline 25 mg, which was an error attributed to confusion with an over-the-counter (OTC) antidiarrheal medication. The overdose resulted in life-threatening consequences, including a coma and cardiac conduction disorder with widening of the QRS complex. The patient’s toxic symptoms resolved following serum alkalinization with bicarbonate administration.
Case presentation
A 70-year-old female with a medical history of hypertension, type 2 diabetes mellitus, liver cirrhosis, multinodular goiter, gallstones, mixed tension migraine, and sleep disorder presented to the emergency department with altered mental status and an impaired response to painful stimuli. The initial differential diagnosis included cerebral infarction, meningitis, and metabolic disorders. On examination, her vital signs were heart rate 120 beats/min, blood pressure 140/80 mmHg, respiratory rate 20 breaths/min, temperature 36.6°C, oxygen saturation of 98% while receiving oxygen via nasal cannula at 3 L/min, and Glasgow Coma Scale 8/15 (E2 M5 V3). 5 The patient’s mouth was noted to contain a large amount of cloudy white fluid, likely vomitus, and the gastric tube drained a significant volume of foul-smelling fluid.
Magnetic resonance imaging (MRI) revealed no evidence of acute cerebral infarction or major cerebral artery occlusion. A neurology consultation was obtained, and stroke was considered unlikely. Arterial blood gas analysis, liver function tests, serum ammonia, electrolytes, and other routine biochemical investigations were all within normal limits except for a mildly elevated random blood glucose level and C-reactive protein (CRP; Table 1). Additionally, abdominal ultrasound, chest radiography, and urinalysis showed no abnormalities. Collectively, these findings helped rule out structural brain lesions, hypoglycemia, hyperglycemia, electrolyte imbalance, acid–base disorder, hepatic encephalopathy, and sepsis as potential causes of the patient’s impaired consciousness. During medication reconciliation, the patient’s prescribed medications were identified as amlodipine 5 mg once daily, amitriptyline 25 mg once daily, flunarizine 5 mg once daily, paracetamol 500 mg twice daily, and a combination of magnesium lactate and vitamin B6 (940 mg/10 mg) once daily. Apart from amlodipine, which she had been taking long-term for hypertension management, the remaining medications were prescribed by a chronic pain clinic for the management of mixed tension migraine and sleep disorder, with a planned duration of 28 days. Collateral history obtained from the patient’s daughter revealed that all the prescribed medications appeared to be administered in the correct quantities, with sufficient supply remaining for 24 days after 4 days of use. However, the box of amitriptyline 25 mg contained only five tablets, suggesting that the patient might have consumed 19 tablets over the past 24 h. The patient’s daughter reported that the patient had been alert and engaging in her usual daily activities but was found unconscious in bed at ~10:30 PM, about an hour after taking her medication at around 9:30 PM. The patient’s daughter reported that the day before the incident, the patient experienced diarrhea and consumed a yellow-colored tablet resembling amitriptyline. This tablet was identified as “berberine 10 mg,” a herbal, nonprescription antidiarrheal medication. This raised the possibility that the patient had mistakenly ingested a large quantity of amitriptyline tablets, confusing them with the antidiarrheal medication (Figure 1).
Laboratory findings on patient admission.
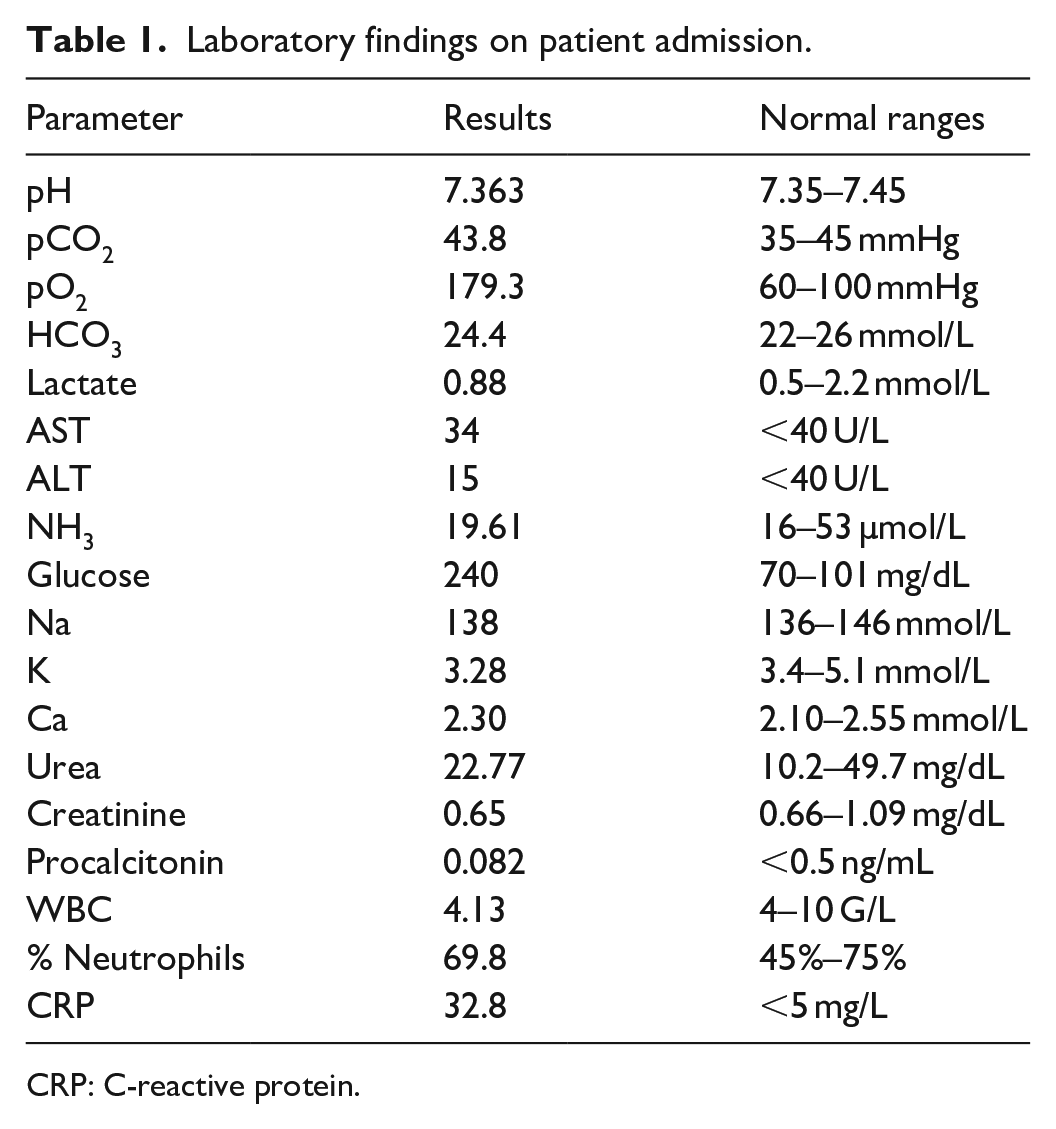
CRP: C-reactive protein.

Confusion between berberine and amitriptyline due to look-alike tablets and packaging.
In the emergency department, the rapid urine drug screening for substances of abuse was negative for heroin/opioids/morphine, amphetamines, methamphetamines, barbiturates, cocaine, phencyclidine, and cannabinoids but tested positive for tricyclic antidepressants. In addition, quantitative analysis of plasma drug concentrations detected a low plasma acetaminophen level (0.11 mg/L) and confirmed the presence of amitriptyline in the patient’s blood. However, the exact amitriptyline concentration could not be determined due to the absence of a validated quantification protocol in the laboratory. The electrocardiogram (ECG) on admission demonstrated sinus tachycardia at a rate of 120 beats/min, a widened QRS complex measuring ~110 ms, a QRS axis of 60°, and a prolonged corrected QT interval (QTc) of 566 ms. Notably, a deep notched S wave was observed in lead augmented vector left (aVL) (Figure 2). The patient’s blood pH was 7.405. Initial treatment included administration of sodium bicarbonate at a dose of 1 mEq/kg, equivalent to 50 mL of undiluted 8.4% sodium bicarbonate and infused over 10 min using an electric syringe. A repeat arterial blood gas analysis performed after the bicarbonate infusion showed a blood pH of 7.437, prompting the administration of an additional dose of 50 mL of 8.4% sodium bicarbonate infused over 10 min. Following the administration of a 100 mEq bicarbonate infusion, the patient’s heart rate decreased to 102 beats/min, accompanied by a reduction in QRS duration to 94 ms on ECG (Figure 3). The patient’s consciousness improved, as evidenced by spontaneous eye opening, purposeful voluntary movements, and appropriate responses to verbal stimuli. The second arterial blood pH was measured at 7.44. To maintain alkalosis with a target pH of 7.45–7.55, an infusion of 150 mL of 8.4% sodium bicarbonate diluted in 1 L of D5W was initiated at a rate of 250 mL/h. A follow-up arterial blood gas analysis showed a pH of 7.49. By the second day, the patient demonstrated significantly improved consciousness, stable vital signs, and the ability to follow simple medical commands. Bicarbonate was discontinued. The patient was subsequently transferred to the Neurology Department of a district hospital for ongoing management due to financial constraints. After 10 days of hospitalization, she regained full consciousness and was discharged in stable clinical condition. At a 4-month follow-up, she remained well without any neurological sequelae or delayed complications.

Admission electrocardiogram.

Electrocardiogram following bicarbonate administration.
Discussion
The emergency management of unconscious patients is challenging due to the wide range of potential underlying causes and the need for urgent diagnosis and intervention. 6 The primary causes of altered consciousness in the emergency department include trauma, neurological disorders, metabolic disturbances, and intoxications, with intoxication accounting for up to 20% of cases. 7 Obtaining information from witnesses or family members regarding pre-unconsciousness symptoms, the timeline of altered consciousness, and the patient’s current medications is essential for accurate evaluation and diagnosis.8,9
In this case, laboratory investigations, including MRI and electroencephalogram, revealed no abnormalities and no evidence of infection apart from an isolated elevation in CRP. Renal and liver function tests, along with other biochemical parameters, were within normal limits. Heteroanamnestic information provided by the patient’s daughter raised suspicion of amitriptyline overdose, which was subsequently supported by the presence of sinus tachycardia and myocardial conduction abnormalities, including a widened QRS complex exceeding 100 ms. 10 Acute ingestion of 10–20 mg/kg of most tricyclic antidepressants can lead to severe cardiovascular and central nervous system effects. 11 If the patient indeed consumed 19 tablets of amitriptyline 25 mg, as suspected, corresponding to a dose of ~10.55 mg/kg, she would be at risk of severe, potentially life-threatening toxicity. 12 Sinus tachycardia can be caused by the antimuscarinic and sympathomimetic effects of amitriptyline. 13 A QRS prolongation exceeding 100 ms is associated with an increased risk of intubation, hypotension, seizures, and dysrhythmias and serves as an indication for initiating sodium bicarbonate therapy.14–16 A pivotal prospective study demonstrated that among patients with a QRS duration of 100 ms or more, 34% experienced seizure and 14% developed ventricular dysrhythmias. 17 In contrast, no seizures or ventricular dysrhythmias were observed in patients with a QRS duration of <100 ms. The use of sodium bicarbonate to achieve a target pH of 7.45–7.55 alleviates amitriptyline-induced cardiotoxicity by increasing extracellular sodium to overcome sodium channel blockade. Alkalinization of the blood reduces drug binding to cardiac sodium channels and increases protein binding, thereby lowering the pharmacologically active free drug level.15,18 Following two intravenous boluses of 50 mEq of sodium bicarbonate, the patient exhibited significantly improved consciousness. To maintain alkalinization for at least 12–24 h post-ECG normalization, due to drug redistribution from tissue to blood, 11 a continuous infusion of 150 mEq of sodium bicarbonate was initiated in this case.
Unintentional drug poisoning occurs more frequently than intentional poisoning in older patients and is associated with a higher risk of mortality compared to younger individuals.19,20 In our case, medication poisoning in an older adult resulted from confusion between look-alike drugs, amitriptyline and berberine, due to their similar yellow color, tablet appearance, and packaging. Berberine, a nonprescription medication commonly used to treat diarrhea, is typically administered at 0.1–0.3 g/dose, three times daily—equivalent to 10–30 tablets of 10 mg berberine/dose. 21 In our case, the patient reported that she routinely took “a handful” of 10 mg berberine tablets whenever experiencing diarrhea and confirmed doing so on this occasion. A potential contributing factor to the confusion between the two medication bottles is the patient’s significantly reduced visual acuity in both eyes—especially in the left eye, where vision is almost completely lost due to a physical injury sustained 20 years ago. Additionally, her blurred vision may have been further impaired by complications of diabetes. Given the similarity in appearance between the two medications, it is highly plausible that she unintentionally ingested 19 tablets of amitriptyline 25 mg, mistaking them for berberine. Up to 14.7% of medication errors are attributed to look-alike/sound-alike medications, as similarities in name, dosage form, strength, or packaging can result in the administration of the wrong medication or dose, leading to overdoses or adverse effects.22,23 Addressing these challenges requires a comprehensive approach to improving medication safety. Providing clear explanations about medications and strengthening family involvement during care transitions are crucial for ensuring safe medication use at home. Family members play a key role in assisting older patients with drug administration, recognizing therapeutic benefits and adverse effects, and clarifying information, particularly for those with reduced cognitive capacity.24,25 Pharmacists play a crucial role in medication reconciliation during care transitions, as well as educating older adults and their caregivers about potential medication confusions and look-alike medication risks. Pharmacists can help to ensure patients can clearly distinguish between prescription medications and over-the-counter products. 26 Implementing strategies such as placing auxiliary warning labels on look-alike medication containers, counseling families to store medications with similar appearances or packaging in separate locations, using dispensing devices like pillboxes or blister packs to organize medications by dosage times, encouraging patients to keep their medicines in their original containers, and referring the patient for a medication review by a pharmacist can significantly reduce the risk of accidental overdoses and enhance medication safety in elderly populations.4,27,28 A key limitation of this case report is that the quantitative toxicological analysis was only able to detect the presence of amitriptyline, without determining the exact drug concentration. In many low- and middle-income countries, access to advanced toxicological assays, such as high-performance liquid chromatography or gas chromatography-mass spectrometry, is limited by high costs, lack of specialized equipment, and a shortage of trained personnel.29,30 In this case, the diagnosis of amitriptyline intoxication was primarily supported by heteroanamnestic information provided by the patient’s daughter, the exclusion of other differential diagnoses for the patient’s impaired consciousness, characteristic electrocardiographic findings (QRS prolongation to 110 ms), a positive urinary qualitative test for tricyclic antidepressants, and the detection of amitriptyline in the blood. While high serum concentrations can correlate with toxicity severity, clinical management is primarily guided by ECG abnormalities and symptoms, as these have stronger predictive value for complications such as arrhythmias or seizures. 17
Conclusion
Amitriptyline overdose can present with a range of symptoms, including anticholinergic effects, impaired consciousness, cardiac complications (i.e. prolonged QTc interval, widened QRS duration, sinus tachycardia, hypotension), convulsions, and, in rare cases, respiratory distress syndrome. Life-threatening toxicity typically occurs with ingestions exceeding 10 mg/kg in adults. Serum alkalinization with intravenous bicarbonate remains the cornerstone of treatment for tricyclic antidepressant toxicity to achieve cardiovascular stability and prevent fatal arrhythmias. This case also underscores the critical role of family engagement and healthcare professionals in implementing strategies to minimize unintentional medication errors and enhance safe drug administration for older adults.
Footnotes
Acknowledgements
We thank Dr. Duy for his assistance in editing the ECG image to enhance its clarity and visibility.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Author contributions
H.V.N.: conceptualization, patient management, manuscript drafting, and editing. K.A.N.: patient management, manuscript drafting, and editing. N.K.D.: patient management, manuscript drafting, and editing. L.R.: manuscript drafting and editing. T.T.N.: patient management, manuscript drafting, and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.