
Abstract
Background:
Poor adherence to antipsychotic medications is the leading cause of relapses and hospitalizations in patients with schizophrenia, resulting in worse functional outcomes and quality of life. Long-acting injectable (LAI) antipsychotics are an effective therapeutic option to improve adherence, but they are often underutilized, particularly during inpatient care.
Objective:
To investigate the predictive factors for LAI utilization among inpatients with schizophrenia and to assess whether initiating a LAI antipsychotic treatment during hospitalization reduces the risk of readmission.
Design:
Observational prospective study.
Methods:
Patients were evaluated at admission, discharge, and after 3 months. Two comparisons were performed: patients who initiated a LAI during the hospitalization versus those who continued with oral antipsychotics, and readmitted versus not-readmitted patients within 3 months. Factors statistically associated with LAI initiation or readmission were entered as independent variables in two backward logistic regression models, having “LAI initiation” and “rehospitalization at three months” as outcomes.
Results:
One hundred two patients were included. Twelve were lost at follow-up. Forty-two (44%) initiated an LAI during the admission. Subjects who received LAI were significantly younger, more educated, and less adherent to treatment. Thirty (33%) patients were readmitted within 3 months after discharge. Re-hospitalized subjects had more psychiatric hospitalizations in the past and a lower rate of LAI antipsychotic treatment initiation during the studied hospitalization: 5/39 (13%) patients prescribed a LAI antipsychotic were readmitted within 3 months, compared with 25/51 (49%) prescribed an oral antipsychotic medication (OR = 0.19; p = 0.002).
Conclusion:
Introducing LAI antipsychotic treatment during a psychiatric hospitalization may reduce the risk of early readmissions, thus facilitating the improvement of the course of the illness and the patient’s quality of life.
Introduction
Schizophrenia is among the psychiatric disorders with the greatest impact on patients’ lives, with a lifetime prevalence of approximately 1% worldwide. 1 Successful treatment of acute episodes and long-term maintenance with antipsychotics plays a key role in reducing relapse and promoting long-term stability.2,3 This is critical in a condition characterized by a chronic nature, where recurring episodes often result in worsening symptoms, cognitive decline, and an overall decrease in the patient’s quality of life. 4 Despite the essential role of antipsychotic therapy, poor adherence to these medications concerns about 30%–40% of patients with schizophrenia, represents the leading cause of relapse, 5 and is associated with increased risk of hospitalization and poor outcomes.6–9 In light of this, several studies focused on long-acting injectable antipsychotics (LAIs) that require less frequent and controlled administration compared to oral antipsychotics (OAPs) and are associated with better adherence, 10 prolonged sustainable effects even when discontinued 11 and consequent better outcomes: lower risk of relapse, hospitalization and mortality, lower healthcare costs, better and more certain knowledge about the status of adherence, and greater chance of receiving psychosocial treatments during longer states of clinical stability.7,12–14
Despite guidelines recommendations, prescriptions for LAI antipsychotics remain low: around 30% or less of total APs in Europe and the United States.11,13,15–19 Studies on inpatient populations have found even lower rates of LAI-AP prescriptions, ranging between 8.9% and 13.9%.11,20–22 Conversely, two works performed on selected samples within mental health quality improvement programs or university hospitals have reported higher rates (35%–44%) in inpatient settings.17,23 Even when initiated during hospitalization, LAI treatment is associated with improved adherence and reduced readmissions post-discharge, provided patients do not discontinue this treatment early.11,21–25
The aims of this observational prospective study were, first, to investigate the predictive factors for LAI utilization among inpatients with schizophrenia and, second, to evaluate the association between in-hospital LAI initiation and readmission. To our knowledge, this is the first study in Europe to explore these specific aspects of inpatient LAI utilization.
Methods
The study has an observational prospective design and conforms to the STROBE statement (Supplemental Material). 26 It was performed on clinical data collected between January 1, 2021, and March 31, 2023, at the inpatient psychiatric unit “Servizio Psichiatrico di Diagnosi e Cura, Dipartimento di Salute Mentale, Azienda Unità Sanitaria Locale della Valle d’Aosta” in Aosta, Italy.
Clinical data were collected by consulting the hospital discharge forms and computerized medical records. Inclusion criteria were: (a) hospitalization in the inpatient unit “Servizio Psichiatrico di Diagnosi e Cura, Dipartimento di Salute Mentale, Azienda Unità Sanitaria Locale della Valle d’Aosta” between January 1, 2021, and December 31, 2022; (b) age at admission ⩾ 16 years; (c) discharge diagnosis of a schizophrenia spectrum disorder according to the DSM-5 criteria 27 ; (d) discharge in the community.
Exclusion criteria were: (a) pregnancy; (b) moderate to profound intellectual developmental disorder (DSM-5 criteria 27 ); (c) being a forensic patient; (d) treatment with a LAI at admission; (e) treatment with clozapine at admission and/or discharge.
In Italy, almost all psychiatric hospitalizations occur in wards within a general hospital. These wards are called “Servizi Psichiatrici di Diagnosi e Cura” (SPDC) and are part of the mental health departments of the national health service. SPDCs have a maximum of 16 beds and an average stay of 12.4 days per hospitalization. 28
Data were collected at three time points: (i) at admission in the psychiatric ward (t0); (ii) at discharge (t1); (iii) 3 months after discharge (t2). At discharge (t1), we evaluated the administration of a LAI treatment during the hospitalization as the outcome variable. At t2, the outcome was the presence of at least one re-hospitalization during the 3-month follow-up.
The following sociodemographic and clinical variables were collected for each patient:
(a) Sociodemographic variables: age, gender, marital status, education, employment status, housing situation, access to social incentives including social inclusion checks, civil disability pensions, survivor’s pensions, and work grants.
(b) Clinical variables: nonpsychiatric comorbidities, psychiatric comorbidities, duration of illness, number of previous psychiatric hospitalizations, number of previous antipsychotic treatments, active and past alcohol and/or substance abuse, documented poor adherence in the last psychiatric visit before admission, type of the current admission (voluntary vs compulsory), and psychopharmacological treatment at admission and discharge.
Documented poor adherence was evaluated as follows. During interviews at outpatient psychiatric units, the psychiatrists of the Mental Health Department (Dipartimento di Salute Mentale) routinely assess adherence to psychopharmacological treatments with the patient and his or her key caregivers. Based on the information collected during the interviews, the psychiatrists report a situation of probable poor adherence to the computerized medical records. To define a case of documented poor adherence, we consider the last record in the 3 months before the date of admission.
Statistical analyses
Normality distribution of continuous variables was assessed with the Shapiro-Wilk test. These data were described with medians and interquartile ranges, while categorical ones were described with absolute frequencies and percentages. At discharge (t1), patients who initiated a LAI during the hospitalization (LAI) were compared with those treated with oral antipsychotics (OA). At follow-up (t2), the comparison was between readmitted and non-readmitted patients. Continuous data were compared with the Mann–Whitney U test, and categorical data with the χ2 test.
Variables showing statistically significant between-group differences in the t1 or t2 comparisons were entered as independent variables into two different multivariate backward logistic regression models (one for each comparison). The first model had “LAI administration during hospitalization” as the outcome variable, and the second had “one or more readmissions during the follow-up period.” A significance level of 5% (p < 0.05) was considered for all statistical analyses.
Statistical analysis was performed with Statistical Package for Social Sciences (SPSS) software version 28 for Windows (IBM Corporation, Armonk, NY, USA).
Results
One hundred and two patients were included in the study. Twelve were lost at follow-up.
Table 1 shows the comparison between patients who received a LAI during the hospitalization (n = 42; 41.2%) and those who did not (n = 60), suggesting a high percentage of subjects who were admitted without LAI antipsychotic therapy and who received it for the first time during hospitalization. No differences were found in antipsychotic class prescription.
Comparison between patients treated with oral antipsychotics or LAI during the hospitalization studied.

Significant differences are in italics.
AP, antipsychotic; F, female; IQR, interquartile range; LAI, long-acting injectable; t0, admission time of the hospitalization studied.
Patients who received a LAI were significantly younger and more educated, and had a higher frequency of documented poor adherence to psychopharmacological treatments in the 3 months before admission. Of the 51 cases of poor adherence, 48 (94%) were documented during the psychiatric examination carried out in the emergency room within 4 h of admission to the ward. In the other three cases, the examination was conducted in the outpatient clinic within 1 month of admission. No differences were found in antipsychotic class prescription.
The comparison between readmitted (n = 30) and not-readmitted (n = 60) patients during the 3-month follow-up is shown in Table 2. Readmitted patients constituted 1/3 of the sample. Patients who had been early rehospitalized (revolving-door phenomenon) had a past history of numerous previous psychiatric admissions and were less likely to initiate an LAI during the studied hospitalization, that is, had continued with oral antipsychotic therapy after discharge. No differences were found in antipsychotic class prescription.
Comparison between readmitted and non-readmitted patients during the 3-month follow-up.
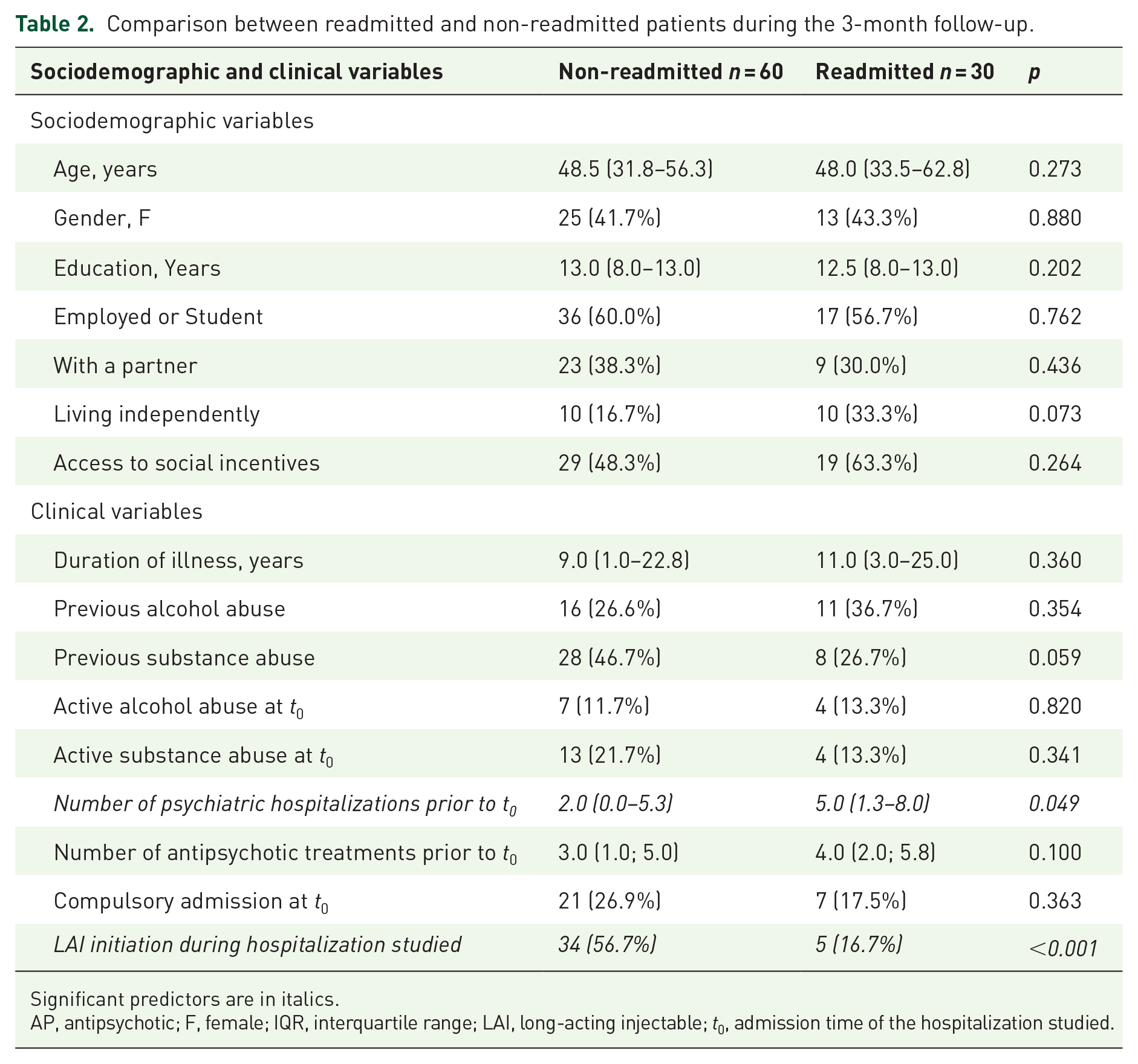
Significant predictors are in italics.
AP, antipsychotic; F, female; IQR, interquartile range; LAI, long-acting injectable; t0, admission time of the hospitalization studied.
The first regression model (Table 3) indicated that higher education and poor adherence in the last 3 months were significantly associated with the initiation of a LAI during the hospitalization studied. Subjects who had more years of schooling (OR 1.17, 95% CI 1.03–1.33, p = 0.020) and poor documented adherence immediately prior to admission were more likely to start LAI therapy during the study hospitalization. In particular, every year of education was associated with a mean probability increase of 17% to initiate an LAI antipsychotic.
Factors associated with the LAI initiation during the hospitalization studied (n = 102).
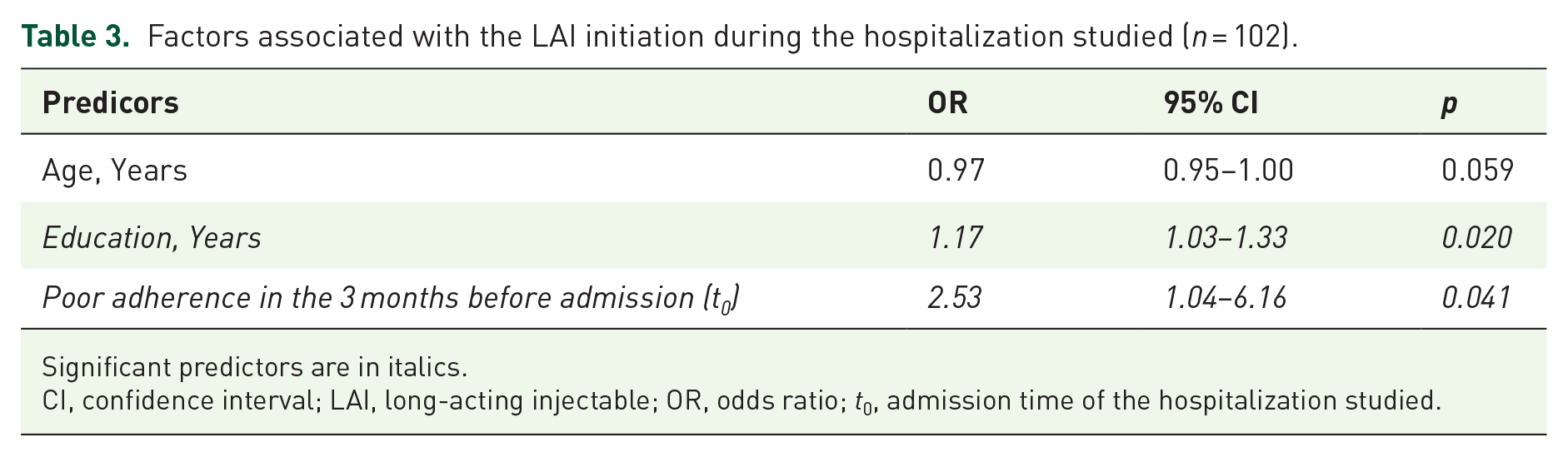
Significant predictors are in italics.
CI, confidence interval; LAI, long-acting injectable; OR, odds ratio; t0, admission time of the hospitalization studied.
Using a threshold of p < 0.05, in the second regression model, only LAI use was associated with fewer readmissions within 3 months (17% LAI antipsychotics vs 57% oral antipsychotics, OR 0.19, 95% CI 0.7–0.55, p = 0.002) Table 4 shows the significant result of the second regression: LAI administration during the hospitalization studied was a negative predictor of readmission during the 3 months after discharge: 5/39 (13%) patients prescribed an LAI antipsychotic were readmitted within 3 months compared with 25/51 (49%) prescribed an oral antipsychotic medication (OR = 0.19, p = 0.002). This result suggests that the introduction of an LAI antipsychotic during hospitalization reduces the risk of early readmission.
Predictors of readmission within 3 months (n = 90).

Significant predictors are in italics.
CI, confidence interval; LAI, long-acting injectable; OR, odds ratio; t0, admission time of the hospitalization studied.
Discussion
The prevalence of LAI use among patients with schizophrenia in our acute inpatient psychiatric unit was 41%. LAI initiation during hospitalization was significantly associated with two predictors: poor adherence to oral antipsychotics in the 3 months before admission and higher levels of education. Moreover, inpatients who received LAI antipsychotic treatment during their hospital stay had a lower risk of readmission in the 3 months following discharge.
The first result, concerning LAI prescription rates, aligns with an Italian observational study that reported a prevalence of inpatients with schizophrenia spectrum disorder treated with LAI antipsychotics at the end of a stay in an acute ward of 46%, regardless of whether LAI therapy was present or not upon admission to the ward. 29 In contrast, several other studies on inpatient populations report significantly lower rates, ranging from 8.9% to 13.9%.11,20–22 This variability may depend on the high heterogeneity between studies regarding settings, healthcare systems, cohort characteristics, and sociodemographic profiles.11,17–19,23,29,30 Despite these differences, similar prescription rates have been observed across studies with distinct designs, which might still suggest that factors such as local clinical traditions and prescribing habits may play a significant role in determining LAI utilization.11,17–19,23,29,30 Thus, further research is needed to explore how these factors, alongside the clinical context, affect the implementation of LAIs in inpatient settings across diverse environments.
Our study also identified predictors associated with LAI initiation during hospitalization. A large Italian observational study reported that aripiprazole LAI was more frequently prescribed to patients with higher levels of education. 31 While no specific explanation was provided for this association, our findings confirm a significantly greater use of LAIs among inpatients with higher educational attainment. Notably, there is limited evidence in the literature addressing the role of education in LAI initiation. We hypothesize that higher inpatients’ education may influence the patients themselves, clinicians, and the doctor-patient therapeutic relationship in terms of discussion about initiating a LAI antipsychotic treatment during the acute phase of illness: on one hand, more educated inpatients might better comprehend the long-term benefits of LAIs and advocate for themselves better; on the other, clinicians may find it easier to begins the conversation about whether to initiate an LAI and fell more secure to obtain a fully informed consent for LAI treatment from these patients.
Similarly, poor adherence to oral antipsychotics before admission emerged as a significant predictor of LAI initiation. This finding is consistent with current guidelines for the management of schizophrenia, which recommend LAIs for patients demonstrating poor adherence to oral treatments, particularly when this is accompanied by recurrent relapses.10,32,33
The percentage of readmitted patients within 3 months (33%) was similar to that reported by previous studies,34,35 highlighting the need to prevent the so-called revolving-door phenomenon. Several studies demonstrated that LAIs represent a valuable tool in reducing the risk of relapse and re-hospitalization, both in real settings abroad7,8,12–14,22,36–38 and in Italy.29,39 Notably, a recent large observational study emphasized that initiating LAI antipsychotic treatment earlier in the course of illness offers even greater protective effects against relapses and hospitalizations. 10 In our cohort, the LAI initiation was not an early intervention per se but, in many cases, a secondary response to poor adherence to oral antipsychotics (OAPs) and subsequent relapses that necessitated hospitalization. Nonetheless, this approach proved significantly more effective than oral therapies in preventing early readmissions. Consequently, proactively offering LAI treatment to all eligible patients and prioritizing antipsychotics with available LAI formulations should be integral to therapeutic shared decision-making.
To our knowledge, this is the first study to employ this specific experimental design in Europe, as previous studies that focus on both LAI initiation in inpatients and readmission rates after discharge were not conducted in Europe or adopted different experimental designs on different clinical populations. In particular, they described LAI utilization rates in hospitalized patients,11,21 focused on predictors of LAI treatment initiation during hospitalization in the United States, 23 or investigated the rates and speed of psychiatric readmission 29 or primary adherence and medication persistence to LAI antipsychotics following inpatient psychiatry hospitalization. 24
Conversely, a recent Taiwanese nationwide cohort study by Chen et al. 22 employed a design similar to the present work but focused on first-admission patients and spanning a 14-year period. In contrast, our study is based on a monocentric sample from an acute inpatient psychiatric unit in Europe. Our sample was not limited to first-admitted patients, and the data were more recent (up to 4 years ago). Consequently, our study provides additional information that is likely more generalizable to the current European context.
Strengths and limitations
The study design presents some strengths. Nearly all patients admitted to the psychiatric ward who met the inclusion criteria were enrolled, thereby minimizing selection bias. Moreover, the prospective observational design, unlike randomized controlled trials, provided the opportunity to assess the impact of LAI initiation on readmission in a real-world clinical setting, free from the limitations of strict inclusion criteria.
Despite these strengths, some limitations must be acknowledged. First, as this is an observational study, the absence of randomization means that we could not control for possible confounding factors. These could have influenced the decision of LAI treatment initiation or might have affected the risk of early readmission. Second, the relatively small sample size limits the methodological robustness and the clinical relevance of the study. Third, relying on clinical documentation for data collection limits our capacity to account for unmeasured variables, mainly symptom severity psychometric scales, that may have influenced treatment decisions or readmission outcomes. In particular, adherence assessment carried out by a clinician without a validated scale could lead to a high risk of errors in estimating adherence rates. Fourth, both the adherence assessment period prior to admission and the follow-up period after discharge are short: 3 months. Longer observation periods could lead to different results. Finally, the monocentric nature of the study limits the generalizability of these results to other clinical settings.
Conclusion
In conclusion, our findings suggest that initiating treatment with LAI antipsychotics during hospitalization significantly reduces the risk of early readmission, potentially reducing the revolving-door phenomenon in schizophrenia care, likely by improving adherence and, as a result, decreasing relapse rates. This therapeutic approach has the potential to not only improve the prognosis and quality of life of patients but also to reduce the direct and indirect costs associated with schizophrenia. Moreover, our study highlights key predictors of LAI initiation during hospitalization, including higher education and poor previous adherence to antipsychotics. However, given the broad benefits of treatment with LAIs across various outcomes, it may still be beneficial to consider their early introduction regardless of education level and independently from the evidence of past nonadherence. 10 These findings underscore the importance of integrating LAIs as a routine part of treatment strategies in inpatients with schizophrenia.
Supplemental Material
sj-doc-1-tpp-10.1177_20451253251367591 – Supplemental material for Use of long-acting injectable antipsychotics in an acute inpatient psychiatric unit and 90-day re-hospitalization rates: results of an observational prospective study
Supplemental material, sj-doc-1-tpp-10.1177_20451253251367591 for Use of long-acting injectable antipsychotics in an acute inpatient psychiatric unit and 90-day re-hospitalization rates: results of an observational prospective study by Claudio Brasso, Anna Maria Beoni, Gianluca Colli, Giulia Nicoletta Mariani and Paola Rocca in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.