
Abstract
Background:
The use of continuing antipsychotic medication is an established evidence-based strategy for preventing relapse in people with schizophrenia, but medication adherence is known to be suboptimal. Covert non-adherence can be eliminated by the use of long-acting injectable (LAI) formulations. We sought to (1) raise awareness among clinicians of the potential benefits of LAI antipsychotic formulations, (2) increase use of these formulations for the treatment of schizophrenia in routine clinical practice and thereby (3) reduce the number of relapses requiring hospitalisation in patients with schizophrenia under our care.
Method:
Educational initiatives, promotion of reflective practice and patient-specific reminders were used to prompt increased use of LAI antipsychotic medication for patients with schizophrenia. Data relating to the use of these medications and the number of acute admissions for schizophrenia spectrum disorders (F20-29, ICD-10) over time were extracted from existing clinical information systems.
Results:
Over the 3-year time frame of our local initiative, the use of LAI antipsychotic preparations increased by 11%, the number of acute admissions for schizophrenia/schizoaffective disorder (F20 and F25) decreased by 26% and the number of acute bed days occupied by patients with these diagnoses decreased by 8%. The number of admissions for other psychosis diagnoses (F21-24 and F28-29) did not show the same pattern of improvement.
Conclusion:
In our health care organisation, raising clinicians’ awareness of the evidence base relating to the potentially favourable benefit–risk balance for LAI antipsychotic medication compared with oral formulations resulted in more use of the former. There were accompanying reductions in acute admissions and occupied bed days for patients with schizophrenia.
Introduction
Continuing treatment with antipsychotic medication reduces the risk of relapse in patients with schizophrenia by two-thirds, 1 and discontinuation studies suggest that more than half of those who stop antipsychotic treatment will relapse within a year.1,2 Furthermore, poor adherence to antipsychotic medication in patients with schizophrenia is an established clinical problem, being the most common cause of relapse and increasing the risk of hospital admission up to fourfold. 3 Where medication delivery can be assured by the use of long-acting injectable antipsychotic medications (LAIs), evidence from randomised controlled trials,4,5 as well as naturalistic4,6 and mirror image studies,4,7 suggests that there are benefits with respect to reduced relapse requiring hospitalisation compared with use of the oral formulations of antipsychotic medication. Clinical guidelines for the treatment of schizophrenia therefore recommend that the use of LAI formulations should be considered where the need to monitor medication adherence is a priority or the patient prefers the convenience of this approach.3,8
National Health Service (NHS) RightCare uses routinely collected NHS data in England to highlight variations between clinical commissioning groups (CCGs) in health care resource utilisation as well as the provision of selected interventions and patient outcomes. Its aim is to use these benchmarked data to inform and stimulate discussions within health care provider organisations and ultimately lead to improvements in both patient outcomes and the use of resources. 9 In 2017, RightCare published a mental health conditions pack, 10 customised by benchmarking each CCG against its 10 most demographically similar CCGs in England. Each mental health provider organisation (trust) in the United Kingdom provides care for the population of several CCGs.
Oxleas NHS Foundation Trust provides mental health services for the London boroughs of Bexley, Bromley and Greenwich on behalf of the CCGs in these boroughs. The RightCare benchmarked data for these CCG populations revealed that hospital admissions for severe mental health conditions were 40–70% higher than the mean value for demographically similar populations in England, and that these differences were statistically significant. Furthermore, compulsory admissions under mental health legislation were 30–60% higher. These figures suggest that local reflection was required to understand the potential reasons for these differences, followed by actions to reduce relapse and hospital admission in patients with severe mental illness. We chose to focus early efforts on the care of patients with schizophrenia as such patients occupy a large proportion of our acute adult beds; there are established evidence-based guidelines for the management of this condition;3,8 and a number of clinical studies report better outcomes when medication adherence is guaranteed through the use of LAI antipsychotic formulations. 4
The aims of our work were therefore to (1) raise awareness among clinicians of the evidence base relating to the potential benefits of LAIs in patients with schizophrenia, (2) increase the use of these formulations in routine clinical practice and thereby (3) reduce the risk of relapse requiring hospitalisation in patients with schizophrenia under our care.
Method
Raising awareness among clinicians of the evidence base relating to the potential benefits of LAIs in patients with schizophrenia
A range of general educational approaches were used, including dissemination to clinicians (predominantly doctors) of ‘seven key messages’ (a locally produced two-page summary of the literature addressing the use of antipsychotic medication for relapse prevention in people with schizophrenia), revision of the local ‘positive practice prompts’ factsheet for schizophrenia (a one-page summary of the key recommendations in the National Institute for Health and Care Excellence (NICE) schizophrenia guidelines 8 highlighting recommendations relating to the use of LAIs and their place in the care pathway) and the inclusion of brief items in the monthly pharmacy newsletter drawing attention to relevant new key publications. In addition, tailored presentations were delivered at academic meetings, discussions facilitated at clinicians’ peer-review groups and clinicians who prescribed LAIs less often than their peers were visited individually to discuss the clinical evidence. Caseloads were reviewed with community psychiatric nurses in some clinical teams to identify patients who might benefit from treatment with an LAI. Finally, patient-specific reminders were used by pharmacists to draw attention to individual patients who might benefit from treatment with an LAI.
Data relating to the use of LAIs and the number of acute admissions for schizophrenia spectrum disorders were extracted from existing clinical information systems as described below.
Quantifying the usage of LAIs in routine clinical practice
In our health care organisation, high-use, low-monetary-value items such as first-generation antipsychotic (FGA) LAIs are issued as bulk stocks to inpatient areas and community mental health teams via the pharmacy stock control system (Emis-web 11 ). Annual issue data were used to estimate the number of patients receiving treatment with these medications as follows: LAI flupentixol, LAI zuclopenthixol and LAI fluphenazine were assumed to be administered every 2 weeks, while LAI haloperidol and LAI pipotiazine were assumed to be administered every 4 weeks; these assumptions are consistent with the median and modal dosage intervals for these preparations identified in a large national audit conducted by the Prescribing Observatory for Mental Health. 12 One vial or ampoule was assumed to be one dose. While it is likely that more than one ampoule was used for a small proportion of doses, it is unlikely that this proportion changed over time; differences in estimated usage therefore are likely to be real.
The number of patient-years of LAI treatment was calculated using issue data for FGA LAIs whereby one patient-year of treatment was determined as 26 two-weekly doses or 13 four-weekly doses. Issues for second-generation antipsychotic (SGA) LAIs are made against prescriptions, so the exact number of patient-years of treatment with LAI aripiprazole, LAI risperidone, LAI paliperidone and LAI olanzapine was known.
Measuring admissions for, and acute bed occupancy by, patients with schizophrenia
Data relating to patients with diagnostic ICD-10 codes 13 in the F20-29 category (schizophrenia spectrum disorders) were extracted from the organisations electronic clinical records system (Rio 14 ). These were divided into two subgroups as follows: (1) data relating to patients with a documented diagnosis of schizophrenia (F20) or schizoaffective disorder (F25), and (2) data relating to patients with diagnoses (F21-24 and F28-29) other than schizophrenia or schizoaffective disorder. The diagnoses in the second subgroup were acute and transient psychotic disorders and delusional disorders, diagnoses for which an LAI was considered unlikely to be indicated.
Data for the financial year 2016–2017 (April 2016–March 2017) were used to determine the baseline position. Year 1 was 2017–2018, year 2, 2018–2019 and year 3, 2019–2020.
Results
Usage of LAIs over time
In 2016–2017, an estimated 799 patient-years of LAI prescriptions were issued. By 2019–2020, this number was 889 – an increase of 11%. Over the same time period, the proportion of such prescriptions that was for SGA LAIs increased from 18% to 33%. The discontinuation of both LAI pipotiazine and LAI fluphenazine contributed to this change (see Table 1). The overall pattern of change in the use of LAIs can be seen in Figure 1.

Estimated number of patient-years of treatment with an LAI antipsychotic medication at baseline and in the three subsequent years.
Estimated number of patient-years of treatment with each LAI antipsychotic medication at baseline (2016–2017) and in the three subsequent years.

LAI, long-acting injectable.
Number of admissions for schizophrenia/schizoaffective disorder and other F20-29 diagnoses
The number of admissions each year for those patients with a diagnosis of schizophrenia/schizoaffective disorder decreased from 617 at baseline to 459 in year 3 (a reduction of 26%). The annual decrease in such admissions over this period is shown in Figure 2, along with the data relating to admissions for patients with diagnoses other than schizophrenia/schizoaffective disorder.
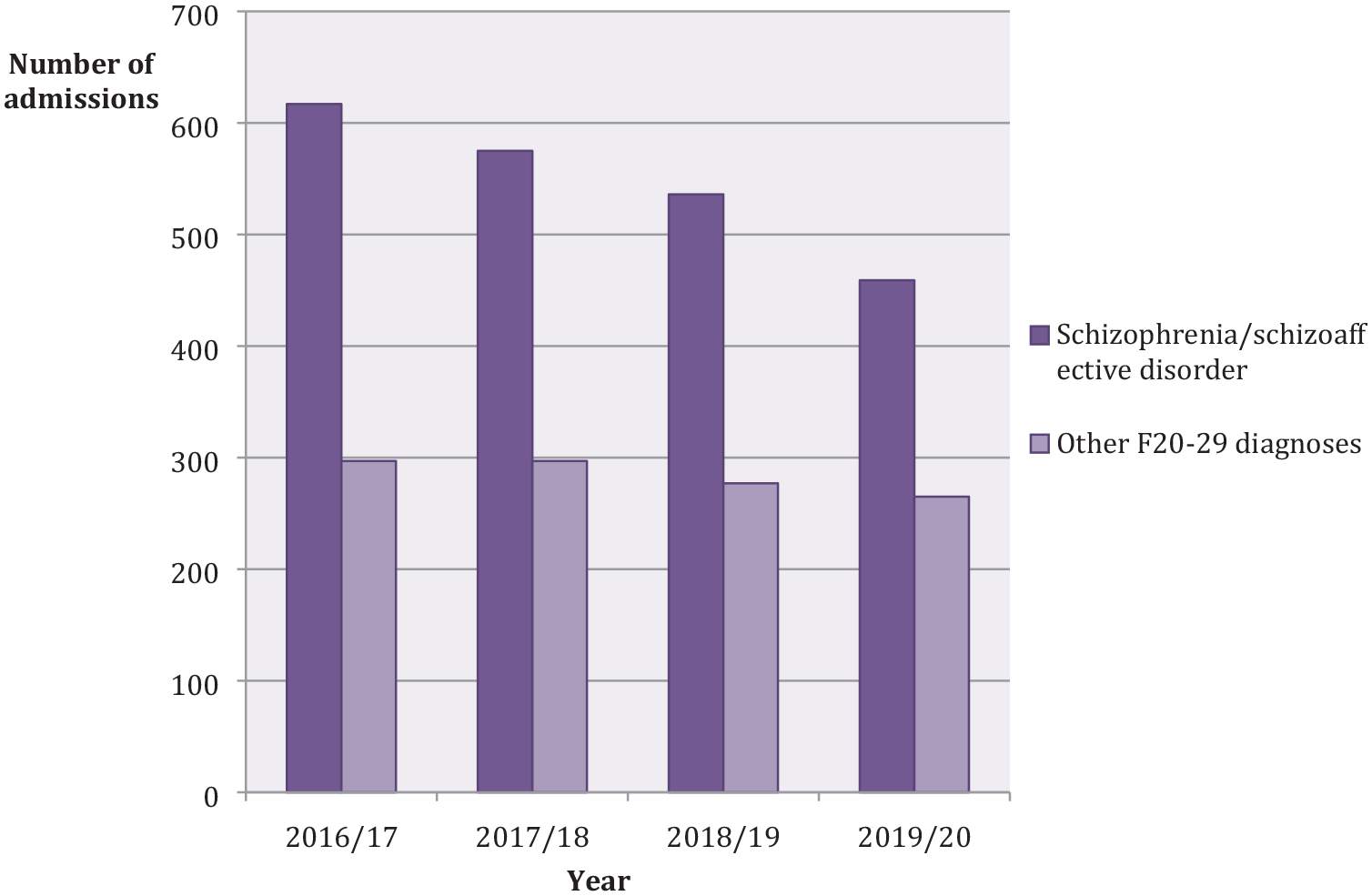
Number of admissions each year for patients with a diagnosis of schizophrenia/schizoaffective disorder and other F20-29 diagnoses at baseline and in the subsequent 3 years.
Number of occupied bed days for schizophrenia/schizoaffective disorder and other F20-29 diagnoses
The number of occupied bed days each year for those patients with a diagnosis of schizophrenia/schizoaffective disorder decreased from 31,788 at baseline to 29,213 (a reduction of 8%) in year 3. For those patients with F20-29 diagnoses other than schizophrenia/schizoaffective disorder, the respective figures were 8992 and 10,635; an increase of 18%. The annual change over the 3-year period can be seen in Figure 3.

Number of occupied bed days each year for schizophrenia/schizoaffective disorder and other F20-29 diagnoses at baseline and in the subsequent 3 years.
Discussion
Our strategies to raise awareness of the potentially favourable risk–benefit balance of LAIs compared with oral antipsychotic formulations were successful in increasing the use of LAIs in a single health care provider. In the 3 years of our initiative, there were incrementally fewer relapses requiring hospitalisation for patients with schizophrenia/schizoaffective disorder.
Strategies used to inform and influence clinical decision making
The dissemination of printed educational materials such as nationally produced evidence-based clinical guidelines, guideline summaries, and publications in peer-reviewed journals and newsletters is a strategy commonly used in health care settings to improve clinical practice. 15 A systematic review of studies evaluating this ‘spray and pray’ approach concluded that it probably has a small effect on the practice of clinicians, but that there is insufficient evidence to determine whether this translates into better outcomes for patients. 15 But when guidelines are adapted locally, the content is built into continuing education programmes and patient-specific reminders are provided at the point of decision making, the likelihood of success increases. 16 We used all of these approaches to try to influence prescribing decisions.
The materials we circulated included locally developed summaries of the evidence-based guidelines relating to the treatment of schizophrenia developed by NICE 8 and the current evidence base relating to relapse prevention in schizophrenia. We backed this up with presentations at local academic meetings and facilitated discussions at clinicians’ peer-review groups focusing on how the key messages relating to the benefits of LAIs were received and what the barriers were to changing practice. Finally, pharmacists provided patient-specific prompts when care plans were being reviewed for patients with schizophrenia who had relapsed and been admitted to hospital.
Focus was maintained over time by the dissemination (via the pharmacy newsletter) of brief summaries of published key clinical papers relating to relapse prevention in patients with schizophrenia (e.g. the Forum article by Correll et al. 17 exploring the risk–benefit ratio of long-term antipsychotic medication for relapse prevention in schizophrenia and the accompanying commentaries 18 ), papers reporting on the beneficial effects of LAIs in preventing hospitalization for schizophrenia (e.g. the nationwide cohort study by Tiihonen et al. 6 ) and studies that suggest it is the LAI formulation rather than the particular antipsychotic medication that leads to this outcome (e.g. the randomised controlled trial (RCT) of LAI paliperidone versus LAI haloperidol for the maintenance treatment of schizophrenia which failed to find an efficacy advantage for the former 19 ).
Our interventions were provided as part of routine health care delivery; we did not check the accuracy of clinical coding nor control for prescriber turnover. Furthermore, we did not evaluate the effect of any of the individual components, nor the degree of clinicians’ engagement with the key messages nor whether the prescribing practice of individual clinicians changed over the 3-year period of our study. However, we could measure, at an organisational level, changes in prescribing practice, the number of acute admissions for schizophrenia and the number of occupied bed days for patients with this diagnosis.
Changing pattern of LAI antipsychotic usage use over time
The use of LAIs overall increased incrementally, reaching 11% by 3 years. LAI zuclopenthixol and LAI flupentixol were the most commonly used preparations, together accounting for around half of all LAI use; the number of patient-years of treatment with these medications remained stable from baseline through the following 3 years. A possible explanation for this finding is that a large proportion of patients receiving these medications have been stable on treatment for many years. There are some data to support better outcomes for LAI zuclopenthixol with respect to time to treatment discontinuation and hospital admission6,20,21 and this had led to this preparation being used selectively in local services for patients who are acutely unwell and hospitalised.
Most of the increased use of LAIs was attributable to LAI aripiprazole and LAI haloperidol, suggesting that these preparations were selectively used when initiating an LAI. Greater awareness of the relative side effects of antipsychotic medications, specifically the relatively lower liability of LAI aripiprazole to be associated with extrapyramidal and prolactin-related side effects and weight gain, 22 likely underpinned the increased use of this medication. The increased use of LAI haloperidol may have been secondary to local discussions relating to the findings of the RCT of LAI paliperidone versus LAI haloperidol, where no overall efficacy or tolerability advantage was found for the former. 19 It is also possible that patients who had presumably been tolerating the first-generation LAIs fluphenazine or pipotiazine were switched preferentially to LAI haloperidol when the former two preparations were discontinued. Both LAI haloperidol and aripiprazole are usually administered monthly.
With respect to other LAIs, the use of LAI paliperidone increased modestly, while for LAI risperidone, it decreased modestly; LAI paliperidone is a simpler preparation to use than LAI risperidone as the lengthy initial oral supplementation required for the latter is not required. 23 Furthermore, the injection interval is longer and there is no need for reconstitution or cold chain storage and distribution. 23 Use of LAI olanzapine has always been relatively low; the close monitoring that is required after each injection to detect and manage postinjection syndrome24,25 renders this preparation impractical to use routinely in many community mental health settings.
Hospital admissions and bed occupancy
By year 3, the number of admissions for patients with schizophrenia/schizoaffective disorder had decreased by 26% and the number of bed days occupied by these patients had reduced by 8%. We expected only modest early benefits within the health care system as a whole from the increased use of LAIs but for these benefits to accrue over time; the greater the number of patients receiving LAIs, the fewer the number of relapses due to non-adherence we expected. This was indeed the pattern of improvement that was seen, with a small reduction in admissions in year 1 that increased incrementally over time. The number of occupied bed days also fell, but gains were more modest. The most likely explanation for this differential effect is that while LAIs may reduce relapse rates as a consequence of better medication adherence, this will have little effect on the illness trajectory of those patients who have complex and/or treatment-refractory illness; multi-episode illness can become increasingly treatment resistant and be associated with greater social decline, issues that can be time-consuming to address. 3 Around a quarter of patients with a diagnosis of schizophrenia have a treatment-refractory illness from the first episode,26,27 and in a further 16–30%, the illness becomes treatment refractory over time. 27
Avoidance of relapse and associated hospitalisation are undoubtedly important outcomes for patients with schizophrenia. 28 Such patients who receive an LAI antipsychotic can and do relapse despite guaranteed medication delivery, 29 but given that there is some evidence to suggest that one patient in every six who relapses does not regain their previous level of functioning, 30 any strategy that has the potential to reduce relapse may also decrease the risk of evolving treatment-resistant illness in some patients. This hypothesis is worthy of further exploration.
From the perspective of a health care provider, the increased use of LAIs is also likely to yield benefits. Munro et al. 31 reported that in one London health care provider, three-quarters of hospital admissions for relapse of schizophrenia were associated with non-adherence with prescribed antipsychotic medication and the mean cost per admission was around £25,000. We found 158 fewer admissions in year 3 compared with baseline; using the figures of Munro et al., 31 this would equate to an estimated saving of almost £4 million in service delivery costs in a single year. Further incremental benefits are likely to accrue over time.
The reductions in admissions and occupied bed days we found were relatively specific to those patients with a diagnosis of schizophrenia/schizoaffective disorder and were not generalisable to patients with other psychotic disorders for which LAIs are not routinely indicated. This suggests that the benefits seen may be attributable to the increased use of LAIs rather than any wider changes in service delivery such as community crisis support or hospital admission criteria.
Limitations of the study
The number of patient-years of LAI antipsychotic treatment provided in each year of our study was estimated using pharmacy issue data along with assumptions about dosage and dosage frequency. However, our estimates were based on the findings from a large national audit of LAI prescribing and so are likely to be robust. 12
It is unlikely that the increased use of LAIs that was seen over time was wholly explained by increased use in patients with schizophrenia. However, in UK mental health services the proportion of patients prescribed an LAI antipsychotic who have a diagnosis of schizophrenia has remained consistent over time, at around 80%. 8 This suggests that most of the increased use we report was accounted for by prescriptions for patients with schizophrenia.
We used routinely collected clinical data and did not follow up a cohort of patients. Data relating to relative outcomes with different LAIs are therefore not available.
Continuing antipsychotic medication is not the only protective factor against relapse requiring hospitalisation in patients with schizophrenia. We did not control for changes to service provision or models of care, but the reductions in admissions and acute bed occupancy found for patients with schizophrenia were not apparent for those patients with other psychotic spectrum disorders, for which the use of an LAI is unlikely to be indicated. This suggests that the outcomes seen for those with a diagnosis of schizophrenia/schizoaffective disorder may be attributable to increased use of LAIs.
Key points
Research studies have shown that, compared with oral antipsychotic medication, LAI preparations are associated with fewer relapses and hospital admissions.
It is possible to increase the use of LAIs in routine clinical practice at the level of a health care provider.
Such increased use is associated with fewer admissions and less occupied bed days for schizophrenia – outcomes that are beneficial to both patients and providers of health care.
Benefits accrue over time.
Footnotes
Acknowledgements
Acknowledgements are due to the clinicians and clinical pharmacists in Oxleas NHS Foundation Trust who supported this work, to Lynn Gathercole for help with data extraction from the pharmacy stock control system and Hector Kurtyanek for his help with data extraction from Rio. Thanks are also due to Dr Stania Kamara for her help in supporting community psychiatric nurses to identify patients on their caseload who might benefit from long-acting injectable (LAI) antipsychotic medication.
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was carried out by the authors as part of their employment with Oxleas NHS Foundation Trust.
Ethical statement
The work reported in this paper did not involve anything being done to patients beyond their normal clinical management and therefore does not require formal ethical approval.