
Abstract
Background:
This study was conducted to determine the impacts of medication adherence on hospitalization and direct healthcare cost in patients with schizophrenia in Thailand.
Methods:
A retrospective study was undertaken. Patients with schizophrenia aged 18–65 years who visited a University hospital and received antipsychotics from April 2011 to October 2011 were included. Propensity score–adjusted logistic regression was used to determine the impacts of medication adherence on schizophrenia-related and all-cause hospitalizations.
Results:
A total of 582 patients were included. Three out of 224 patients (1.3%) were hospitalized with schizophrenia in optimal adherence group, while 10 of 140 (7.1%) were hospitalized in under-adherence group, and 7 of 218 (3.2%) were hospitalized in over-adherence group. Based on propensity score–adjusted multivariate logistic regression, the adjusted odds ratio was 5.86 (95% confidence interval = 1.53–22.50) for schizophrenia-related hospitalization and 8.04 (95% confidence interval = 2.20–29.40) for all-cause hospitalization. The average annual direct healthcare costs in patients with optimal adherence, under-adherence, and over-adherence were US$371 ± US$836, US$386 ± US$734, and US$508 ± US$2168, respectively.
Conclusion:
An initiation of interventions to maintain optimal adherence in patients with schizophrenia would significantly impact the healthcare system.
Background
Schizophrenia is a severe mental disorder which affects more than 21 million people worldwide. 1 It is a chronic disease associated with long-lasting health, social, and financial burdens. The chronic nature of the illness and a need for recurrent hospitalization also contribute to increasing cost.2,3
Adherence to medication is crucial in clinical outcomes of patients with schizophrenia. The average rate of non-adherence with antipsychotic medication in patients with schizophrenia ranged from 40% to 60%. 4 The lack of medication adherence has been studied and is associated with an increased risk of hospitalization. 5 This poses a major concern to all stakeholders including healthcare professionals, administrators, and patients. Several factors associated with re-hospitalization have been studied including short duration of admission, medication non-adherence, poor post-discharge services, and younger age.6–9 It is estimated that over US$100 billion total cost per year is due to medication non-adherence resulting in hospitalization and repeated doctor visits in the United States. 10 However, it should be noted that not only under-adherence is associated with an increased risk of hospitalization and healthcare cost. Over-adherence is also associated with an increased risk of hospitalization and healthcare costs.11,12
To our knowledge, no study has been conducted to determine the impacts of antipsychotic adherence on hospitalization in patients with schizophrenia and healthcare cost in Asia. A study assessed outcomes and factors associated with re-hospitalization in patients with schizophrenia in Malaysia, but did not report the impact of antipsychotic adherence on hospitalization. 13 In Thailand, no study has been conducted to determine the impacts of antipsychotic adherence on hospitalization and cost in patients with schizophrenia. Conducting such studies in Thailand will facilitate and inform healthcare decision-makers among all stakeholders to allocate limited healthcare resource to this particular population effectively. Therefore, this study aimed to determine the clinical and economic impacts of antipsychotic adherence on hospitalization and healthcare cost in patients with schizophrenia, using Thailand as an example.
Method
Setting and data sources
A retrospective cohort study using electronic databases from a 1000-bed university affiliated hospital in Bangkok, Thailand was conducted. The databases consisted of inpatient and outpatient databases, a pharmacy database, and a charge database. Patients’ demographic information (e.g. age, gender) and diagnosis code (International Classification of Diseases version 10; ICD-10) were extracted from the inpatient and outpatient databases. Information on drugs’ names and days’ supply of medication were extracted from the pharmacy database. Information on date of payment, type of payment, and medical charges (medication, medical services, laboratory charges, and radiology charges) were extracted from the charge database. Information was available for all patients who visited outpatient department or were hospitalized from October 2010 to September 2013. Patients were longitudinally tracked for two years. The study was approved by Ethics Committee of Ramathibodi hospital, Thailand.
Patient selection and study period
Patients who visited outpatient department of the hospital and met the following criteria were included in this study. The inclusion criteria were (1) diagnosed with schizophrenia (defined by ICD-10: F20.xx) from April 2011 through September 2011; (2) aged 18–65 years; (3) no history of receiving any antipsychotics within six months before the first schizophrenia-related diagnosis; and (4) received antipsychotics at least two times within 6 months after the index date. The index date was defined as the first date antipsychotic was received. Patients who had missing data on medication administration were excluded. Included patients were tracked for two years after the index date. Data from six months before index date of each patient were used to estimate propensity score (PS) for each patient. Data from the first year after index date were used to determine medication adherence, while data from the following year were used to determine outcomes of interest.
Assessment of adherence and cutoff level
Medication possession ratio (MPR) is widely used and well accepted worldwide to determine medication adherence in various diseases.14–16 In this study, MPR was calculated to measure medication adherence using the pharmacy database. The MPR of each medication of each patient was calculated by the following equation 17

Patients were classified into three groups as under-adherence (MPR < 0.8), optimal adherence (MPR = 0.8–1.2), and over-adherence (MPR > 1.2). MPR of patients who received at least two antipsychotics was averaged. We selected MPR < 0.8 as the threshold of under-adherence based on our literature review.12,18 Several studies suggested that the therapeutic response to treatment for chronic conditions was preserved when patients took at least 80% of the prescribed medications.19,20 We selected MPR > 1.2 as the threshold of over-adherence based on previous studies.11,21 We believe that the 20% difference of perfect adherence would be meaningful for both under-adherence and over-adherence.
Outcomes of interest
Schizophrenia-related hospitalization was the primary outcome of this study. It was defined as any hospitalization with an ICD-10 code as F20.xx. The secondary outcomes were all-cause hospitalization and healthcare cost. All-cause hospitalization was defined as any hospitalization occurring during the second year of follow-up (the outcome measuring period). Healthcare cost was only direct medical cost incurred in the hospital due to hospital perspective. Direct non-medical and indirect cost were not included in this study. Costs were calculated based on charges using average cost-to-charge ratio of university hospital in Thailand which was 0.73. 22
Data analysis
Descriptive statistics (e.g. mean, standard deviation, percentage, and frequency) were used to describe patients’ demographics. PS was estimated using logistic regression based on covariates including age, gender, health insurance, comorbidities (bipolar, dementia, depression, and anxiety), and concurrent medications (antidepressants, antianxiety, mood stabilizers). Multivariable logistic regression analysis was used to evaluate the association of medication adherence level and hospitalization, adjusting for PS, types of antipsychotic use, and other potential confounders. The generalized linear model with log-link function and gamma distribution was used to evaluate the association of medication adherence level and healthcare cost, adjusting for PS, types of antipsychotic use, and other potential confounders. The healthcare costs were reported in 2013 value and were converted to US$ using an exchange rate of 33.02 Baht/US$. 23 Data analyses were performed using STATA version 11.0 (College Station, TX).
Results
Patient characteristics
A total of 1944 patients were diagnosed with schizophrenia during the study period. A total of 582 patients met inclusion criteria and were included in this study (Figure 1). Demographic data were described in Table 1. Patients’ average age was 44.4 ± 11.0 years. A majority of patients were females (56.7%). Approximately, 55.2% received typical antipsychotics, 29.7% received atypical antipsychotics, and 15.1% received both typical and atypical antipsychotics. Health insurance scheme for individuals were 14.2%, 3.4%, and 12.4% for universal coverage, social security scheme, and civil servants medical benefit scheme, respectively. In total, 70% of included patients had no information on health insurance.

Patient selection flow diagram.
Demographic data and relationship between adherence and hospitalization.

UC: universal coverage; SSS: social security scheme; CSMBS: civil servants medical benefit scheme; MPR: medication possession ratio; N/A: not applicable; SD: standard deviation; ANOVA: analysis of variance.
Calculated by ANOVA.
Calculated by chi-square test.
Calculated by Fisher’s exact test.
US$1 = 33.02 Thai Baht.
Medication adherence associated with hospitalization
Among 582 patients, 224 patients (38.5%) were optimal adherence, 140 patients (24.1%) were under-adherence, and 218 patients (37.5%) were over-adherence (Table 1).
A total of 20 patients (3.44%) were hospitalized with schizophrenia. Patients with under-adherence had the highest rate of hospitalization (14 and 10 for all-cause and schizophrenia-related hospitalizations, respectively). Patients with under-adherence had a significantly longer length of hospitalization stays (LOS) than patients with optimal adherence (0.56 ± 2.64 days vs. 0.06 ± 0.57 days; p < 0.01). Patients with over-adherence also tended to have longer LOS than patients with optimal adherence (0.37 ± 2.58 days vs. 0.06 ± 0.57 days; p = 0.067), but it was not statistically significant. Both under-adherence and over-adherence had longer LOS of all-cause hospitalizations than patients with optimal adherence (0.75 ± 2.90 days for under-adherence, 0.38 ± 2.51 days for over-adherence, and 0.06 ± 0.57 days for optimal adherence, p = 0.011) (Table 1).
Based on PS-adjusted multivariate logistic regression, under-adherence had a significant higher risk for schizophrenia-related hospitalization than optimal adherence (adjusted odds ratio (OR) = 6.52; 95% confidence interval (CI) = 1.68–25.27). The adjusted OR for all-cause hospitalization was 7.83 (95% CI = 2.08–29.50) for patients with under-adherence. For patients with over-adherence compared to patients with optimal adherence, the adjusted OR for schizophrenia-related hospitalization was 2.66 (95% CI = 0.67–10.61), while the adjusted OR for all-cause hospitalization was 3.06 (95% CI = 0.79–11.91) (Table 2). Both were not statistically significant. The associations of medication adherence level, hospitalization, and LOS by types of antipsychotics are presented in Tables 3 and 4.
The effects of medication adherence on schizophrenia-related and all-cause hospitalizations compared with optimal adherence.

MPR: medication possession ratio; CI: confidence interval.
Covariates in this model included propensity score, age, and gender.
Suboptimal adherence is either under-adhernce or over-adherence.
Logistic regression analysis of association of hospitalization among schizophrenia patients, by type of antipsychotic.
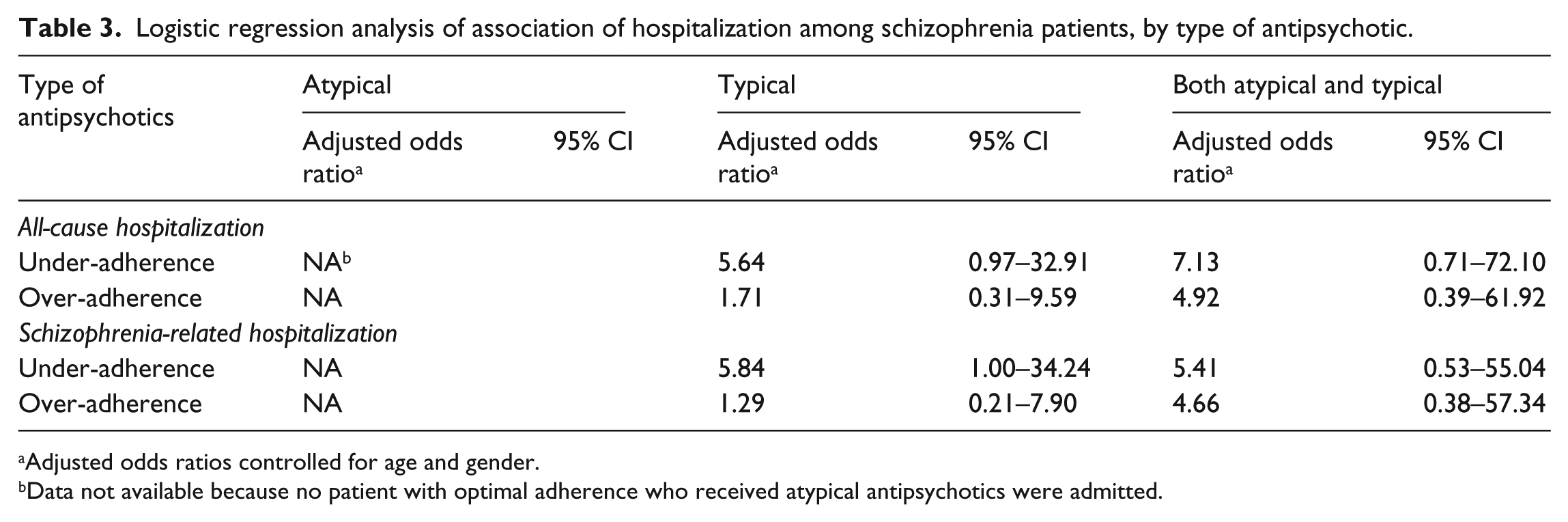
Adjusted odds ratios controlled for age and gender.
Data not available because no patient with optimal adherence who received atypical antipsychotics were admitted.
The association of adherence level, type of antipsychotics, and annual healthcare costs.

US$1 = 33.02 Thai Baht.
Medication adherence associated with healthcare cost
The average direct annual healthcare cost in patients with under-adherence was US$386 ± US$734. The average direct annual healthcare cost of US$508 ± US$2168 in patients with over-adherence, while it was US$371 ± US$836 in patients with optimal adherence (Table 1).
Based on a PS-adjusted multivariate generalized linear model, healthcare cost in patients with under-adherence was US$143 higher than that in patients with optimal adherence (95% CI = US$ -258 to US$544). Healthcare cost in patients with over-adherence was US$116 higher than that in patients with optimal adherence (95% CI = US$ -162 to US$394). However, they were not statistically significant.
Discussion
Among studies measuring medication adherence, this is the first study in Asia-Pacific region to determine the impacts of medication adherence on hospitalization and healthcare cost. Based on our analysis, suboptimal adherence of antipsychotics (both under-adherence and over-adherence) was associated with an increased risk of hospitalization and healthcare cost. Our study reveals that less than 40% of patients adhered to antipsychotics, resulting in a higher risk of hospitalization and annual healthcare cost. These findings emphasize the impacts of suboptimal adherence on clinical and economic outcomes. Interventions or policies should be developed to minimize these dilemmas.
Our findings are consistent with previous studies which revealed the association of suboptimal adherence and a risk of hospitalization and healthcare costs.12,18 It is well known that under-adherence leads to an increased risk of hospitalization and healthcare cost. 24 We found that patients with under-adherence had higher number of hospitalization, longer hospital stays, and higher annual healthcare cost than those with optimal adherence.
Our multivariate analysis indicated that patients with under-adherence had a higher risk of hospitalization than those with optimal adherence or with over-adherence. Compared to optimal adherence, patients with under-adherence had more than five times higher risk of schizophrenia-related hospitalization, and all-cause hospitalization. Similarly, the risk of hospitalization was two times higher in patients with under-adherence than those with over-adherence. The observed hospitalizations may have resulted from subsequent relapses. However, some potential predictors of hospitalizations (confounders) could not be captured in our analyses and they might affect our findings.
Interestingly, we found a higher number of patients with over-adherence than those with under-adherence. The over-adherence was associated with a higher risk of hospitalization compared to optimal adherence. The findings in this study were similar to a previous study which indicated that blood pressure deteriorated when MPR greater than 1. 25 These findings might reflect that the optimal MPR threshold also contributed to the most effective outcomes in patients with schizophrenia. Moreover, direct healthcare cost was highest in patients with over-adherence. Such cost incurred in patients with over-adherence was substantially higher than those in any other groups. High MPR could be one of the markers for less stable patients. Thus, this might alert physician to pay special attention to a group of patients with over-adherence. Basically, the reason why over-adherence leads to an increased risk of hospitalization and healthcare cost remains unclear. Additional studies to determine the causes of over-adherence and its consequences in patients with over-adherence are warranted.
Some limitations of this study should be discussed. First, due to the limitation of available databases used in this study, some important aspects were not addressed including the impacts of health insurance on adherence, the impacts of adherence on quality of life, and indirect cost associated with schizophrenia and hospitalization. Second, our findings cannot be generalized to other populations or countries. However, the findings can be used as a guideline to other populations particularly in Asia-Pacific region. Third, we were not able to address the different risks of hospitalization between patients taking typical and atypical antipsychotics because no patient with optimal adherence who received atypical antipsychotics was hospitalized.
Further studies in large population are needed to determine the impacts of possible healthcare system or organization factors associated with differences in adherence, hospitalization, and healthcare cost including indirect cost. Such studies would help clarify and determine ways to resolve this issue.
Conclusion
There is a consensus in literature that under-adherence leads to poor health and economic outcomes.24,26 In this study, we identified that not only under-adherence was associated with an increased risk of hospitalization and healthcare cost but also over-adherence. We found substantial healthcare cost associated with suboptimal adherence. Targeting to suboptimal adherence patients specifically would improve patient outcomes and lower healthcare cost. Utilization of our findings to develop interventions or policies to maintain optimal adherence in patients with schizophrenia would significantly impact the healthcare system particularly in countries where resources are limited.
Footnotes
Acknowledgements
The authors would like to thank Ramathibodi hospital for providing data for this study. The authors would also like to thank Janssen-Cilag (Thailand) for the supporting financial grant through the education research.
Declaration of conflicting interests
Prof. Nathorn Chaiyakunapruk received a research grant from Janssen Cilag (Regional Office, Singapore; December 2013–November 2014) on Estimating Monetary Burden, Identifying Risk Factors Associated with Poor Adherence and Re-hospitalization in Schizophrenia, and Assessing Current Situation of Electronic Medical Record (EMR) Development, Integration, Utilization, and Availability in Asia-Pacific Countries. This research grant is not directly involved with the work of this presentation. The other authors declared no conflict of interest with this study.
Ethical approval
Ethical approval for this study was obtained from the Ethics Committee of Ramathibodi Hospital, Thailand (approval no. MURA 2013/710).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
This study was conducted using a retrospective database analysis of databases from a 1000-bed university affiliated hospital. Patient identifiers contained in the databases are encrypted. Researchers could not track back to any patients. The need for informed consent was waived by the Ethics Committee of Ramathibodi Hospital.