
Abstract
Background:
People bereaved due to COVID-19 may face mental health challenges and posttraumatic growth opportunities. Resilience, as an inherent trait or ability, may protect the bereaved from developing mental health problems and facilitate growth. The Dual Process Model (DPM) is an important framework for understanding adaptation after bereavement. However, little is known about whether resilience could help with adjusting to COVID-19 bereavement and whether dual process coping plays a part in the relationship between resilience and mental health among COVID-19 bereaved individuals.
Objective:
We aim to examine the relationship between resilience and symptoms of prolonged grief, posttraumatic stress, anxiety, depression, and posttraumatic growth following COVID-19 bereavement, and to investigate the role of dual process coping, which includes loss-oriented (LO) coping, restoration-oriented (RO) coping, and oscillation between LO coping and RO coping in this relationship.
Design:
This is an online cross-sectional survey.
Method:
A total of 408 Chinese participants who lost a close person due to COVID-19 participated in the study from September to October 2020. Demographic and loss-related information was collected. Resilience, dual process coping, symptoms of prolonged grief, posttraumatic stress, anxiety, depression, and posttraumatic growth were measured. Correlation analyses and mediation analyses were conducted to analyze the data.
Results:
Resilience was negatively correlated with anxiety and depressive symptoms and positively correlated with posttraumatic growth. In the relationship between LO coping, RO coping, oscillation, and mental health, LO coping was positively associated with prolonged grief, posttraumatic stress, anxiety, and depressive symptoms, as well as posttraumatic growth; RO coping was negatively associated with prolonged grief symptoms and posttraumatic growth, and positively associated with anxiety and depressive symptoms; oscillation was negatively associated with prolonged grief, posttraumatic stress, anxiety, and depressive symptoms. In addition, mediation analysis showed that oscillation mediated the relationship between resilience and anxiety and depressive symptoms, and RO coping mediated the relationship between resilience and depressive symptoms and posttraumatic growth.
Conclusion:
Our findings indicate that among individuals who have experienced bereavement due to COVID-19, RO coping serves a protective role in the relationship between resilience and depressive symptoms and a facilitative role in the relationship between resilience and posttraumatic growth. Additionally, oscillation plays a protective role in the association between resilience and symptoms of anxiety and depression. Professionals should consider the bereaved individuals’ resilience, LO coping, RO coping, and oscillation when providing support to those bereaved by COVID-19.
Introduction
COVID-19 bereavement has brought bereaved people a number of mental health problems. Prolonged grief disorder (PGD),1,2 previously known as pathological grief, 3 complicated grief, 4 and dysfunctional grief, 5 is one of the main challenges that COVID-19 bereaved people may face, with a prevalence of 9.8% worldwide and 8.9% in China.6,7 In addition, psychological distress beyond grief was also reported among the general population experiencing COVID-19 bereavement, including posttraumatic stress symptoms (22%–83%),8,9 anxiety symptoms (58.5%–70%),8–10 and depressive symptoms (62.3%–74.3%).8–10 As with the general population, psychological distress was equally present in bereaved individuals with a previous history of mental disorders, as evidenced by COVID-19 bereavement exacerbated their psychiatric symptoms. 11
Meanwhile, positive changes following COVID-19 bereavement have been observed. As early as the beginning of the COVID-19 outbreak, scholars pointed out that the adaptation of 20.1% of the COVID-19 bereaved people in their study exhibit characteristics of growth, 12 suggesting that it is worthwhile to examine factors associated with mental health outcomes following COVID-19 bereavement from a strength-based perspective.
Resilience and mental health following bereavement
Resilience has been conceptualized as a process, trait, and outcome.13–15 When facing stressful life events such as bereavement, resilience serves as an inherent trait or ability to flexibly adapt to changing external circumstances 14 and protects people from developing mental health problems. Resilience includes positive traits such as trust, control, acceptance of change, and optimism, 16 as well as the ability to cope with, overcome, and adapt to traumatic experiences, 17 can help bereaved individuals to positively cope with the adverse emotional reactions to bereavement. 18 and give bereaved individuals a more positive outlook and better adaptation. 19 Specifically, as a protective factor, resilience can alleviate mental health problems of bereavement, including grief,20,21 anxiety symptoms, 18 depressive symptoms,18,22–24 loneliness, 22 and psychological distress. 25 Meanwhile, resilience can promote positive outcomes of bereavement, including facilitating posttraumatic growth 26 and increasing life satisfaction. 22
Although the idea of improving the mental health of COVID-19 bereaved individuals by enhancing resilience has been raised, 27 only one empirical study to date has examined the relationship between resilience and mental health in this group of people, reporting that higher levels of resilience were associated with lower levels of pandemic grief. 28 As such, the relationship between resilience and other commonly observed mental health problems and positive psychological changes, including prolonged grief, posttraumatic stress, anxiety, depressive symptoms, and posttraumatic growth in COVID-19 bereaved people, remains to be explored.
Dual process coping and mental health following bereavement
When understanding the process of adapting to bereavement, the Dual Process Model (DPM) proposed by Stroebe and Schut provides an important perspective. 29 DPM states that after the death of a close person, the bereaved person faces stressors originating from both the loss and restoration of life and therefore needs to address and cope with both stressors and challenges simultaneously during the bereavement adaptation process. First, there are loss-oriented (LO) stressors, which refer to the stressful experiences linked to the death of a loved one. For example, an individual in mourning may repeatedly contemplate the events that took place before, during, and shortly after the death, trying to comprehend and manage their loss. Second, restoration-oriented (RO) stressors encompass various experiences that emerge as a (secondary) result of the bereavement event, including taking over the original responsibilities of the deceased, organizing life without the deceased, and developing a new identity. The inclusion of these RO stressors is a crucial and defining feature of the DPM. 30 Therefore, LO coping is associated with focusing on and dealing with certain aspects of the experience of loss, especially those related to the deceased. And RO coping is concerned with coping with changes in life. The two coping processes alternate without a sequential pattern, and there is oscillation between LO and RO coping, which involves alternating and shifting between confrontation and avoidance of different stressors associated with loss. 29 Importantly, those who are grieving need to address both LO and RO stressors, but are not able to attend to both at the same time, so they need to shift their attention (i.e., oscillate) between the two orientations, rather than fixating on just one aspect. In this model, an important postulation is that oscillation is necessary for adaptive coping. 31
LO coping, RO coping, and oscillation play distinct roles in relation to mental health outcomes following bereavement. In most cases, LO coping was maladaptive, as it was positively associated with grief in people who have experienced spousal bereavement,32,33 as well as in parents who have lost their children. 34 In addition, LO coping can also predict more severe anxiety and depressive symptoms.34,35 RO coping, in contrast, was more adaptive, as it enhanced the sense of self-efficacy and personal growth following bereavement, 36 was positively associated with psychological well-being, 20 and negatively associated with grief and depression. 34 More importantly, when bereaved individuals are able to oscillate freely between loss- and recovery-oriented coping, it is the ideal state of adjustment to grief. Oscillation can’t be measured directly, but when the oscillation balance was calculated by calculating the difference in scores between RO coping and LO coping, we observed that oscillation reduced levels of grief of bereaved people and increased their coping self-efficacy. 32 In addition, if they were able to freely and effectively manage the shifts between the emotions associated with loss and daily life without the deceased, they would experience less grief and more positive affect, 33 and would successfully adapt their life after bereavement.
After the COVID-19 outbreak, the DPM was used for understanding the bereavement and adaptation processes of those bereaved by the pandemic, 37 as it allows for a more systematic assessment of loss and restoration-related challenges for the bereaved. For example, under the framework of DPM, we can understand the psychological state of hospice family caregivers when facing COVID-19 bereavement, 38 and to better understand the complexity of the impact of the pandemic on bereaved people, 39 especially their LO and RO stressors and coping strategies.
In conclusion, LO coping, RO coping, and oscillation are important to understand the mechanism of the relationship between protective factors (i.e., resilience in this study) and post-bereavement mental health.
Mediating role of LO coping, RO coping, and oscillation
We are also interested in whether LO coping, RO coping, and oscillation can serve as mediator variables in the relationship between resilience and mental health that affect bereavement adaptation. Several intervention studies have shown that enhancing RO coping can alleviate grief and anxiety symptoms.32,40 Furthermore, research that directly examined LO coping and RO coping as mediator variables indicated that LO coping fully mediated the relationship between risk factors (i.e., subjective traumatic level) and depressive symptoms. 41 The above evidence reveals the feasibility of utilizing LO coping, RO coping, and oscillation as mediator variables.
If people have resilience as a predisposing protective factor, they are more likely to adopt adaptive coping strategies when in crisis or stressful situations. 14 Under the framework of DPM, bereaved individuals with higher levels of resilience tended to employ RO coping, while those with lower levels of resilience tended to rely on LO coping. 20 Moreover, individuals with a greater capacity for resilience may be able to engage in the shifting between LO coping and RO coping more effectively. 42
Based on the above, we propose that LO coping, RO coping, and oscillation may mediate the relationship between resilience and mental health (i.e., prolonged grief, posttraumatic stress, anxiety, depressive symptoms, and posttraumatic growth) in persons bereaved due to COVID-19.
The current study
This study proposed a mediation model that aims to explain how resilience could contribute to prolonged grief, posttraumatic stress, anxiety, depressive symptoms, and posttraumatic growth following COVID-19 bereavement. Specifically, this study aimed to examine the mediating role of LO coping, RO coping, and oscillation in the relationship between resilience and symptoms of prolonged grief, posttraumatic stress, anxiety, depression, and posttraumatic growth (see Figure 1).
In line with the study objective, the current study hypothesized that:
H1: Resilience would be negatively related to prolonged grief, posttraumatic stress, anxiety, and depressive symptoms, while positively related to posttraumatic growth in COVID-19 bereaved people.
H2: Dual process coping, including LO coping, RO coping, and oscillation, would mediate the relationship between resilience and prolonged grief, posttraumatic stress, anxiety, depressive symptoms, and posttraumatic growth in COVID-19 bereaved people.
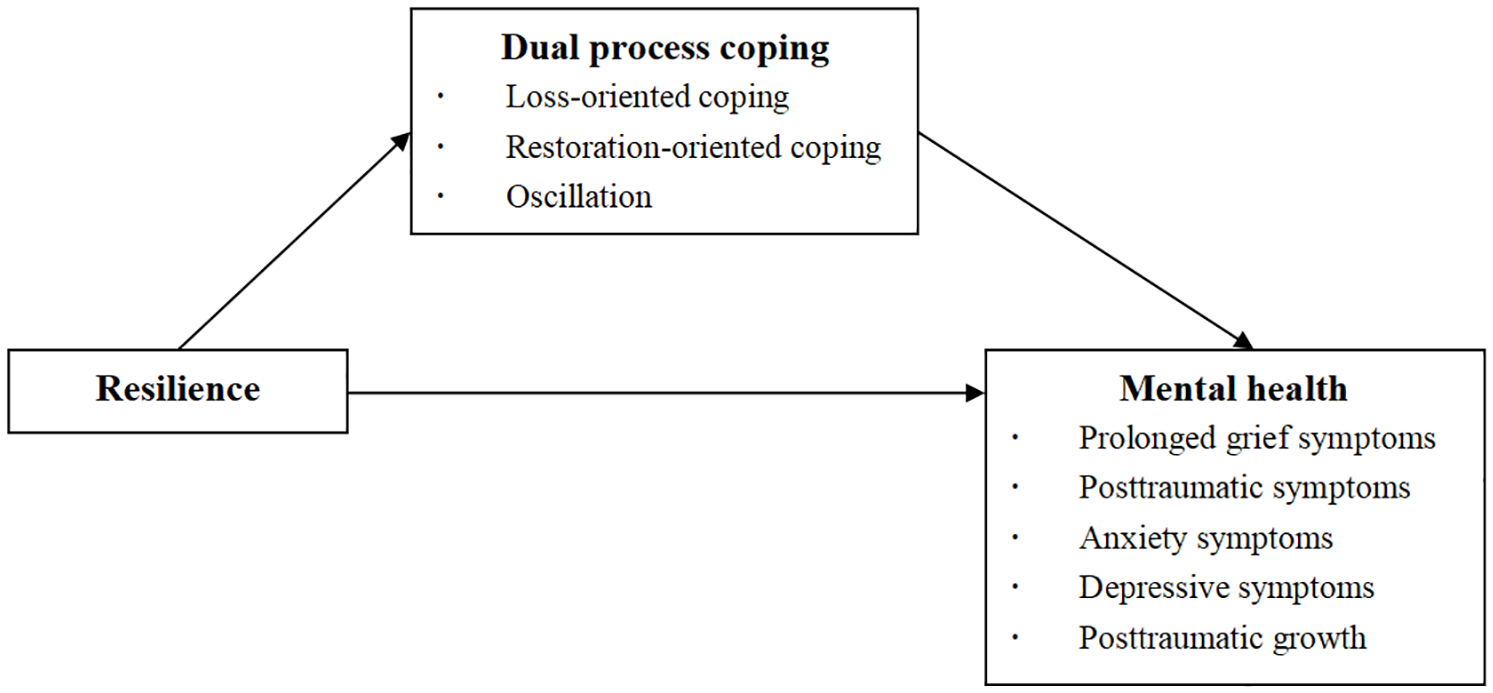
The hypothesized mediation model.
Method
Study design and participants
This study employed a cross-sectional survey design, collecting data from 476 participants via an online questionnaire between September and October 2020. Participants were required to meet the following study eligibility criteria, that is, be at least 18 years of age and bereaved due to COVID-19. For the following reasons, 68 participants were eliminated from the study due to noncompliance with the inclusion criteria: having been bereaved for more than 9 months (n = 11), experiencing a death from a cause other than COVID-19 (n = 14), providing inconsistent information regarding the deceased (n = 15), taking less than 5 min to respond (n = 21), and giving patterned responses (n = 8). Ultimately, data from 408 participants were analyzed.
Procedure
Participants were invited to participate in our study through social network websites (e.g., Baidu and Weibo) as well as mobile applications (e.g., WeChat). The introduction of the study and the inclusion criteria were presented to participants in our recruitment poster, along with a link to the online survey. The informed consent form is included in the link and relates to the purpose of the study, voluntariness of participation, confidentiality, and grief support resources. Participants were only entered into the formal survey if they checked “I understand the above information and agree to participate in this study.” At the end of the survey, a list of support resources specifically for bereaved individuals during COVID-19 was listed, including information on free counseling and grief counseling, self-help resources, and books.
Measures
Demographic and loss-related information
Demographics included sex, age, education, and religious belief. In addition, loss-related information included relationship to the deceased (i.e., partner, child, parent, grandparent, relative, friend, and other relationship), sex of the deceased, age of the deceased, and times since loss in months.
Resilience
Resilience was measured via the Connor-Davidson Resilience Scale (CD-RISC) developed by Connor and Davidson. 16 The original scale consisted of 25 items, 10 of which were extracted by Campbell-Sills and Stein to develop a simplified version of the Psychological Resilience Scale (CD-RISC-10), 43 and the Chinese version of the CD-RISC-10 has been revised and examined. 44 Participants are asked to answer questions on a 5-point Likert scale, ranging from 0 (never) to 4 (almost always). A higher sum score reflects greater resilience. In the present study, the internal consistency coefficient Cronbach α was 0.86.
Dual process coping
The Dual Coping Inventory developed by Meij and colleagues was used to assess two different coping orientations in bereaved people in the past week. 34 The Chinese version has been revised and utilized among Chinese bereaved individuals. 41 The scale consists of seven items, with the LO coping and RO coping subscales containing 3 and 4 entries, respectively. These 7 self-report items are rated from 1 (not at all) to 5 (very much), with a higher sum score indicating that individuals are more inclined to use a particular oriented coping. In the present study, the internal consistency coefficients of Cronbach’s α were 0.80 (LO subscale) and 0.75 (RO subscale), respectively. Moreover, a single self-constructed question on the oscillation between LO and RO coping was asked, namely “I was able to shift my attention between the loss-related thoughts and emotions and the restoration-related thoughts and emotions over the past week.” Participants rated on a 5-point Likert scale that ranged between 1 (extremely difficult to do so) and 5 (extremely easy to do so).
Prolonged grief symptoms
The Chinese version of the International Prolonged Grief Disorder Scale (IPGDS) developed by Killikelly and colleagues was used to assess the severity of prolonged grief symptoms in individuals in the past month. 45 The standard scale of the IPGDS contains 13 items about the yearning, preoccupation, emotional distress, and functioning impairment after losing a close person, and one cultural screening item. A 5-point Likert scale ranging from 1 (almost never) to 5 (always) was used to assess how often participants experienced these symptoms in the past month. The total score of the scale represents the symptom level of PGD, with higher scores indicating higher symptom levels, but with this excluding cultural screening items. In the present study, the internal consistency coefficient of Cronbach’s α was 0.89.
Posttraumatic stress symptoms
The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5) developed by Blevins and colleagues was used to assess the severity of posttraumatic stress symptoms in individuals in the past month. 46 The Chinese version has been revised and applied to healthcare workers during the pandemic. 47 The scale contains 20 items that are rated from 0 (not at all) to 4 (extremely), with a higher sum score suggesting more serious symptoms. In the present study, the internal consistency coefficient of Cronbach’s α was 0.94.
Anxiety symptoms and depressive symptoms
The Hospital Anxiety and Depression Scale developed by Zigmond and Snaith was used to assess individuals’ anxiety and depressive symptoms in the past month. 48 The Chinese version of which has been revised and verified. 49 The scale contains 14 items, with 7 entries for each of the anxiety and depression subscales that are rated on a 4-point Likert scale. Higher sum score reflects more serious symptoms. In the present study, the internal consistency coefficients of Cronbach’s α for the anxiety and depression subscales were 0.77 and 0.75, respectively.
Posttraumatic growth
Posttraumatic growth was measured via the Posttraumatic Growth Inventory (PTGI) developed by Tedeschi and Calhoun. 50 The Chinese version was applied in the study. 51 A 6-point Likert scale ranging from 0 (I have not experienced this kind of change after the loss) to 5 (I have experienced this kind of change to a very great extent after the loss) was used to assess the degree of change experienced by the participants after bereavement. Higher total scores indicated greater positive change following bereavement. In the present study, the internal consistency coefficient of Cronbach’s α was 0.93.
Data analysis
Both SPSS 21.0 and SPSS Macro Process version 3.3 were used for data analysis. First, we conducted a descriptive analysis of demographic and loss-related information about the study participants. Second, we performed Harman’s one-factor test to examine common method bias. Third, Pearson’s correlations were used to analyze correlations between resilience, prolonged grief, posttraumatic stress, anxiety, depressive symptoms, posttraumatic growth, LO coping, RO coping, and oscillation. Finally, utilizing the bootstrap method with Model 4 52 from the SPSS Macro Process program, we conducted an analysis of five mediation models based on the number of dependent variables. In these models, resilience served as the independent variable, while prolonged grief, posttraumatic stress, anxiety, depressive symptoms, and posttraumatic growth were the dependent variables. In addition, LO coping, RO coping, and oscillation were included as mediation variables. A bias-corrected percentile bootstrap method was employed, extracting 5000 bootstrap samples with a confidence interval set at 95%. A significant result was indicated by a confidence interval that does not include 0. The mediation effect size was calculated by dividing the mediation effect value by the total effect value.
The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology statement 53 (see Supplemental Materials). In addition, the questionnaire is also presented in the Supplemental Materials.
Results
Sample characteristics
Demographic and loss-related information are shown in Table 1. The sample included 408 participants who were bereaved due to COVID-19 deaths. Participants were on average 33 years old (mean = 32.87, SD = 9.41). More than half were male (55.1%, n = 225). The majority reported no religious beliefs (93.4%, n = 381). On average, the deceased was 48 years old (mean = 47.42, SD = 21.61). Participants had lost a partner (34.1%, n = 139), child (5.9%, n = 26), parent (23%, n = 94), grandparent (16.2%, n = 66), other relative (4.2%, n = 17), friend (15%, n = 61), or another relationship (1.7%, n = 7). On average, the time since the loss was 5 months (mean = 5.10, SD = 1.74).
Demographic characteristics and loss-related characteristics.

Religious belief included Buddhism (n = 17), Taoism (n = 3), Catholicism (n = 3), Christianism (n = 3), and Islamism (n = 1).
Relative included uncle (n = 5), aunt (n = 4), cousin (n = 4), grandaunt (n = 3), granduncle (n = 1), great grandmother (n = 1), and not specified (n = 4).
Other relationship included colleagues (n = 4), acquaintance (n = 2), and not specified (n = 1).
Common method bias
Given that item characteristics, identical raters, and the same testing context may lead to artificial covariation and thus distort measurements, 54 we employed Harman’s single-factor test to evaluate the presence of common method bias. The findings revealed that there were 16 factors with eigenvalues exceeding 1. The first factor accounted for only 21.99% of the variance, which was below the threshold of 40%, suggesting that our study did not exhibit significant common method bias.
Correlation analysis
Resilience was negatively correlated with both anxiety and depressive symptoms and positively correlated with posttraumatic growth, RO coping, and oscillation. In addition, RO coping was negatively associated with posttraumatic growth, and positively associated with depressive symptoms; oscillation was negatively associated with anxiety and depressive symptoms. The detailed descriptive statistics results and correlation matrix are described in Table 2. Since resilience is not related to LO coping, so we excluded the possibility of LO coping as a mediator variable.
Descriptive statistics results and correlation matrix.

p < 0.05. **p < 0.01. ***p < 0.001.
Mediation analyses
The mediating role of oscillation between resilience and anxiety symptoms
Our findings indicated that the model explained 32% of the variance of anxiety symptoms when using oscillation as the mediator variable (F = 16.11, p < 0.001). As seen in Figure 2, resilience positively predicted oscillation (β = 0.17, t = 3.66, p < 0.01), oscillation negatively predicted anxiety symptoms (β = −0.18, t = −4.41, p < 0.01), and resilience negatively predicted anxiety symptoms (β = −0.21, t = −4.95, p < 0.01). Moreover, bootstrap analysis showed that the direct effect of resilience on anxiety symptoms was −0.11, which accounted for 87% of the total effect. In addition, the indirect effect of resilience on anxiety symptoms via oscillation was −0.02, with confidence intervals that did not include 0, accounting for 13% of the total effect (see Table 3). The above analysis showed that oscillation in dual process coping played a significant partial mediating role between resilience and anxiety symptoms. This finding suggested that relatively higher levels of resilience contributed to oscillation levels, which, in turn, were linked to lower anxiety symptoms.

The mediating role of dual process coping between resilience and anxiety symptoms. (1) Coefficients are standardized regression coefficients; (2) solid lines indicate that the effect is significant and dashed lines indicate that the effect is not significant.
Bootstrap analysis of dual process coping in the relationship between resilience and mental health.

CI, confidence interval; LO, loss-oriented; RO, restoration-oriented.
The mediating role of RO coping between resilience and depressive symptoms
Our findings indicated that the model explained 25% of the variance of depression when using RO coping (F = 11.50, p < 0.001) as the mediator variable. As seen in Figure 3, resilience positively predicted RO coping (β = 0.48, t = 10.72, p < 0.01), RO coping negatively predicted depressive symptoms (β = −0.12, t = −2.89, p < 0.05), and resilience negatively predicted depressive symptoms (β = −0.24, t = −5.57, p < 0.01). Moreover, bootstrap analysis showed that the direct effect of resilience on depressive symptoms was −0.11, which accounted for 78% of the total effect. In addition, the indirect effect of resilience on depressive symptoms via RO coping was −0.03, which accounted for 19% of the total effect, with confidence intervals that did not include 0 (see Table 3). The above analysis indicated that RO coping played a significant partial mediating role between resilience and depressive symptoms. This finding suggested that relatively higher levels of resilience contributed to RO coping levels, which, in turn, were linked to lower depressive symptoms.
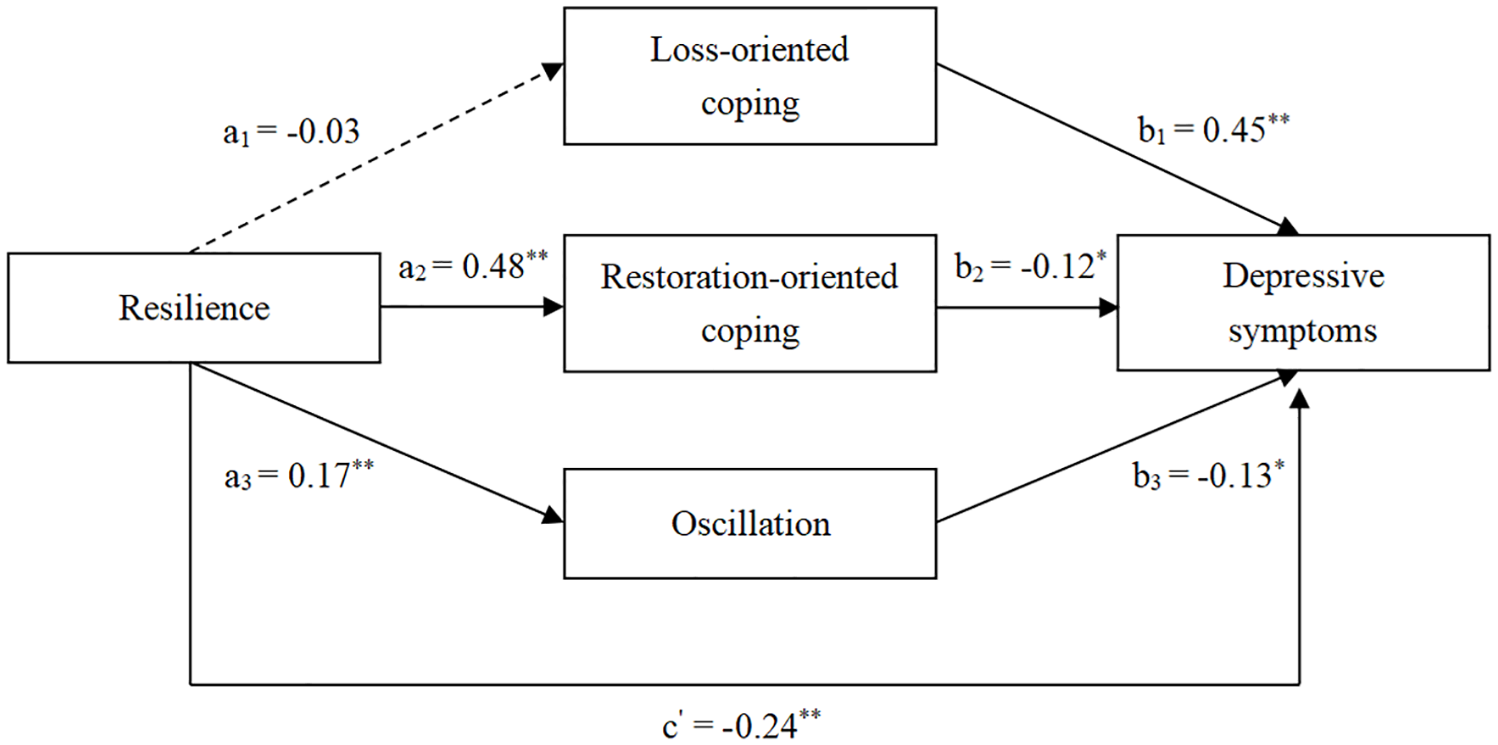
The mediating role of dual process coping between resilience and depressive symptoms. (1) Coefficients are standardized regression coefficients; (2) solid lines indicate that the effect is significant and dashed lines indicate that the effect is not significant.
The mediating role of oscillation between resilience and depressive symptoms
Our findings indicated that the model explained 31% of the variance of depression when using oscillation (F = 14.82, p < 0.001) as the mediator variable. As seen in Figure 3, resilience positively predicted oscillation (β = 0.17, t = 3.66, p < 0.01), oscillation negatively predicted depressive symptoms (β = −0.13, t = −3.05, p < 0.01), and resilience negatively predicted depressive symptoms (β = −0.24, t = −5.57, p < 0.01). Moreover, bootstrap analysis showed that the direct effect of resilience on depressive symptoms was −0.11, which accounted for 78% of the total effect. In addition, the indirect effect of resilience on depressive symptoms via oscillation was −0.01, which accounted for 7% of the total effect, with confidence intervals that did not include 0 (see Table 3). The above analysis indicated that oscillation played a significant partial mediating role between resilience and depressive symptoms. This finding suggested that relatively higher levels of resilience contributed to oscillation levels, which, in turn, were linked to lower depressive symptoms.
The mediating role of RO coping between resilience and posttraumatic growth
Our findings indicated that the model explained 48% of the variance of posttraumatic growth when using RO coping as the mediator variable (F = 30.02, p < 0.001). As seen in Figure 4, resilience positively predicted RO coping (β = 0.48, t = 10.72, p < 0.01), RO coping positively predicted posttraumatic growth (β = 0.20, t = 5.18, p < 0.01), and resilience positively predicted posttraumatic growth (β = 0.56, t = 13.84, p < 0.01). Moreover, bootstrap analysis showed that the direct effect of resilience on posttraumatic growth was 1.39, which accounted for 85% of the total effect. In addition, the indirect effect of resilience on posttraumatic growth via RO coping was 0.24, with confidence intervals that did not include 0, accounting for 15% of the total effect (see Table 3). The above analysis suggested that RO coping played a significant partial mediating role between resilience and posttraumatic growth. This finding suggests that relatively higher levels of resilience contribute to RO coping levels, which, in turn, are linked to higher posttraumatic growth.

The mediating role of dual process coping between resilience and posttraumatic growth. (1) Coefficients are standardized regression coefficients; (2) solid lines indicate that the effect is significant and dashed lines indicate that the effect is not significant.
Discussion
This study is the first to examine the relationship between resilience and prolonged grief, posttraumatic stress, anxiety, depressive symptoms, and posttraumatic growth among bereaved people of COVID-19, as well as the mediating role of LO coping, RO coping, and oscillation. The findings provide empirical support for researchers and practitioners to understand how resilience and coping styles of pandemic-bereaved people are related to post-bereavement adjustment.
Resilience and mental health after bereavement
Resilience is a protective factor for pandemic-bereaved individuals in coping with symptoms of anxiety and depression, and individuals with higher levels of resilience are less likely to face anxiety and depressive symptoms after bereavement, a finding in the present study that is consistent with previous research. 18
In addition, consistent with findings in previous research conducted in Germany on people who have experienced bereavement during the COVID-19 pandemic, 55 the present study did not find a relationship between resilience and prolonged grief symptoms and posttraumatic stress symptoms, which may be related to the unique characteristics of bereavement in the COVID-19 pandemic. Fear of the contagiousness of COVID-19 56 and guilt 57 due to the isolation of the pandemic resulting in the bereaved not being able to say goodbye to their loved ones, not being able to organize funeral ceremonies, and not being able to keep important relics, 58 pandemic-bereaved people may be difficult to enhance their resilience to cope with grief. 28 This suggests that resilience may have a limited effect on prolonged grief symptoms and posttraumatic stress symptoms resulting from pandemic bereavement.
Resilience and dual process coping
The present study focused on the relationship between resilience and dual process coping, especially for the bereaved population of the COVID-19 pandemic. Resilience was positively associated with RO coping and oscillation, which is consistent with the results of previous studies on an international sample of widows and widowers aged less than 50 years old. 20 However, resilience was not associated with LO coping, possibly because resilience is more concerned with adjusting to life changes than with bereavement itself.
The expected new finding is that higher resilience gives pandemic-bereaved individuals the ability to comfortably oscillate between LO coping and RO coping. Perhaps it is because individuals with higher levels of resilience have more adaptive emotion regulation strategies such as refocus on planning and positive reappraisal which contribute to good adaptation after bereavement. 59
Previous research has shown that individuals with higher levels of resilience will use less LO coping, 20 which means there is a negative correlation between resilience and LO coping, but this relationship was not found in the present study. Higher levels of resilience do contribute to individuals to take more positive actions and more proactive strategies to adjust their physical and mental states, 60 but at the same time, they also possess the ability to cope flexibly and strike a balance between grief experience and real-life situations.
The mediating role of RO coping and oscillation
The present study further explored the mediating role of RO coping and oscillation between resilience and mental health. Pandemic-bereaved individuals with high resilience possess the ability to cope flexibly, meaning that individuals can attenuate their emotional intensity about loss, and possess the ability to manage currently unwanted internal experiences (e.g., thoughts, memories, and bodily sensations), as well as perceive and seek social support to cope with real-life stressors. 61 At the same time, they can proactively adjust their behavior and coping strategies, 62 oscillating flexibly between LO coping and RO coping, which reduces anxiety symptoms. Consistent with previous research,18,34 resilience among pandemic-bereaved individuals can help them adopt proactive strategies to positively confront real-world stressors in their restoration orientation. By increasing the processing of real-world activities, including self-monitoring of their mental health status, and arrangements for funerals and memorial services, they have more opportunities to act and exposure to beneficial experiences, thereby alleviating the depressive symptoms associated with bereavement. 63 In addition to alleviating mental health problems, individuals exhibiting high levels of resilience also demonstrate enhanced cognitive flexibility. This refers to their ability to adjust their cognitive schema following traumatic or stressful events, such as bereavement. 64 They actively employ strategies to effectively navigate RO stressors, which encompass reintegration into daily life for a more profound life experience, adjustment to new roles and identity transformations to cultivate more meaningful relationships, and acquisition of coping skills and experiences to manage loss. Consequently, these individuals are more likely to achieve a higher level of posttraumatic growth.26,65,66
Limitations
The present study has the following limitations. First, convenience sampling in the form of online data collection through social media affected the representativeness of the sample and findings. For example, due to the younger skew of social media users and differences in stressors faced by bereavement coping at different ages, 24 resulting in the present study potentially failing to gain a greater understanding of the relationship between resilience, coping styles, and mental health among older pandemic-bereaved individuals. Second, there may be some limitations to the measurement of dual process coping. For example, the measure of RO coping focused on understanding positive perceptions of the future rather than specific behaviors of the pandemic bereaved, and only one question was used to measure the ability to oscillate. Future research could do more to explore what practical coping measures bereaved people adopt when faced with RO real-life stressors and use methods with higher validity to explore bereaved people’s ability to oscillate, such as ecological momentary assessment, which involves measuring their coping strategies multiple times throughout the day to examine whether they switch between different coping strategies. Third, the adoption of a cross-sectional design for the study may also hinder the exploration of the relationship between resilience and mental health in terms of coping styles over time following bereavement. Fourth, the selection of samples in this study lacked the consideration of psychiatric diagnosis, which may have a certain impact on the research results. Future research will consider collecting psychiatric diagnostic information from the sample to better understand the adaptation of the bereaved population. Finally, the study focused solely on individual bereavement adjustment without considering family factors, that is, how families deal with grief. Future research will consider combining questionnaires and interviews to investigate the resilience, coping, and adaptation of bereaved individuals and bereaved families from multiple perspectives.
Conclusion
The current study suggested that (1) Resilience of COVID-19 bereaved persons is negatively associated with anxiety and depressive symptoms and positively associated with posttraumatic growth. (2) LO coping, RO coping and oscillation mediate the relationship between resilience and anxiety symptoms, depressive symptoms, and posttraumatic growth. Practitioners can work to improve the resilience of COVID-19 bereaved people and adjust their service focus according to their resilience levels and coping styles.
Supplemental Material
sj-doc-3-tpp-10.1177_20451253251328607 – Supplemental material for Relationship between resilience and mental health among COVID-19 bereaved people: the mediating role of dual process coping
Supplemental material, sj-doc-3-tpp-10.1177_20451253251328607 for Relationship between resilience and mental health among COVID-19 bereaved people: the mediating role of dual process coping by Liping Wu, Siying Chen and Suqin Tang in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-1-tpp-10.1177_20451253251328607 – Supplemental material for Relationship between resilience and mental health among COVID-19 bereaved people: the mediating role of dual process coping
Supplemental material, sj-docx-1-tpp-10.1177_20451253251328607 for Relationship between resilience and mental health among COVID-19 bereaved people: the mediating role of dual process coping by Liping Wu, Siying Chen and Suqin Tang in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-2-tpp-10.1177_20451253251328607 – Supplemental material for Relationship between resilience and mental health among COVID-19 bereaved people: the mediating role of dual process coping
Supplemental material, sj-docx-2-tpp-10.1177_20451253251328607 for Relationship between resilience and mental health among COVID-19 bereaved people: the mediating role of dual process coping by Liping Wu, Siying Chen and Suqin Tang in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.