
Abstract
A 2019 census of residential care facilities in Guatemala found 3863 children in residential care and that 97% of these children had at least one living relative. The census clearly indicates that children in the facilities are not orphans and the possibility of reunification, if appropriate processes and services are in place to support the child and parent/caregiver before, during, and after reunification, is possible. We (the authors) played a key role in designing a case management process to support the reunification of children from residential care back into families with the end goal being successful reintegration. A series of wellbeing domains were designed to help understand and measure what successful reintegration would include within the case management system. Informed by a case review of 36 Guatemalan children supported to reintegrate into families, and interviews with social workers and psychologists engaged in the process, this article explores the role of the “community connectedness” wellbeing domain. We explore how community connectedness or lack thereof, can contribute to child and parent/caregiver wellbeing and successful reintegration—the different types of community connectedness and who/what was involved in establishing and fostering these connections. With growing interest in reintegration efforts globally, efforts to better understand the unique role that community connectedness has in overall family wellbeing is well timed. Whilst the topic has been explored in post conflict settings with children and youth previously engaged in armed conflict, experiences of reintegration from residential care facilities in non-emergency contexts is limited, including in Spanish speaking contexts.
Background
Moving away from residential care
For the past two decades, there has been increasing discussion about and evidence collected highlighting the negative effects of residential care on child development and wellbeing (Nelson et al., 2014; van Ijzendoorn et al., 2020). The negative effects on children’s socio-emotional, cognitive, and physical development are particularly intense during early childhood and increase the longer a child remains in care (Bunkers et al., 2014; National Scientific Council on the Developing Child, 2012; van Ijzendoorn et al., 2020). There is increasing evidence that illustrates improved outcomes for children who have spent time in residential care but are subsequently reintegrated into some form of family-based care including biological, kinship, foster, or adoptive (van Ijzendoorn et al., 2020). Recent evidence demonstrates that millions of children are separated from families and living in residential care making the need for evidence-based reintegration and families strengthening programs more critical than ever (Desmond et al., 2020; Goldman et al., 2020).
This increasing awareness has resulted in a global movement focused on influencing governments, organizations, faith-based actors, academic institutions, and members of the child protection workforce to focus resources, technical assistance, and systems change toward decreased reliance on residential care as the primary care option for children toward family-based care (Goldman et al., 2020; United Nations General Assembly 74/133 Rights of the Child, 2019; van Ijzendoorn et al., 2020). The process of moving a system away from residential care to one that prioritizes family-based care is often referred to as care reform. The authors understand care reform as the changes to the systems and mechanisms that promote and strengthen the capacity of families and communities to care for their children, address the care and protection needs of vulnerable or at-risk children to prevent separation from their families, decrease reliance on residential care, promote the reintegration of children, and ensure appropriate family-based alternative care options are available. There are three core areas of care reform, and these are all understood and implemented within a systems framework (Changing the Way We Care, 2021). The first element of a care reform approach focuses on strengthening families to prevent separation. This is done via interventions that address the root causes of separation including economic support to address poverty, positive parenting courses to address violence, and facilitating access to critical social services such as health, education, and services for those with a disability. The second component includes the expansion of family-based alternative care such as kinship care and foster care. The third component focuses on interventions that assist children and adolescents currently in residential care to exit and be placed into families. This component also includes the transformation of residential care into family or community-based service models (Better Care Network, 2019; Goldman et al., 2020; United Nations General Assembly, 2019).
Reintegration into family care
Whilst some care reform efforts were initiated more than two decades ago, in Eastern Europe for example, others are nascent. These include reform in both humanitarian and development contexts. However, despite this significant effort taking place in many contexts around the world, there remains limited evidence documenting the reintegration experience and related outcomes of children and their families after the act of reunification takes place. The evidence and documentation that does exist is primarily related to the negative impact of residential care on children’s development and across the lifespan. Evidence also exists highlighting developmental improvements of children moving from residential care to foster care or adoption, especially the seminal research coming out of Romania (Nelson et al., 2014; van Ijzendoorn et al., 2020). Much less has been documented on the process of reunifying children with their biological or extended families and the developmental outcomes for children in that situation. More specifically, there are evidence gaps around the unique experiences, challenges, and successes involved in re-establishing emotional bonds and creating attachment between a child and his or her parents/primary caregivers and the broader community (understood as neighbors, community leaders, religious organizations, and school environments) and how this aspect contributes to the success or failure of this process. Informed by Bronfenbrenner’s (1979) ecological framework demonstrating the interface between a child, his or her family, and their community, this article explores how a sense of belonging to something outside of self and the family, understood within this article as community connection, has played a pivotal role in reintegration outcomes for a cohort of 36 Guatemalan children and their families. The authors believe that including community connection as an indicator of success and designing tools and processes to facilitate it, should be a core part of any reintegration approach.
The terms reunification and reintegration are used throughout this article and the concepts of each term heavily influence its content. The authors have adopted the definitions provided by the Inter-Agency Group on Children’s Reintegration (2016). Reunification is understood as the physical reuniting of a separated child and his or her family or previous caregiver. Reintegration is when a separated child makes what is anticipated to be a permanent transition back to his/her immediate or extended family and the community (usually of origin), to receive protection and care and to potentially find a sense of belonging and purpose in all spheres of life.
The existing evidence base on the impact on children’s development of reintegration into a family from residential care is heavily weighted toward the experiences of children placed in intercountry adoption or of children reintegrated from the foster care system in the United States or the United Kingdom (Hellerstedt et al., 2008; Maltais et al., 2019; van Ijzendoorn et al., 2005, 2020). Research specifically exploring the outcomes for children reintegrated from residential care back into biological or extended families in low socioeconomic contexts remains limited. Efforts to define and measure elements of successful reintegration are also limited, especially in low- and middle-income countries. In the global South, most of the evidence that does exist around reintegration from residential care back into family has primarily focused on the process involved rather than the outcomes for children and families (Inter-Agency Group on Children’s Reintegration, 2016; McMillan and Herrera, 2014; Wedge et al., 2013). There is some evidence from African countries that explores reintegration outcomes for children recruited into armed conflict and their return to family and community (Akello et al., 2006; Betancourt et al., 2010). These studies offer useful insight into the reintegration experience, including exploring beyond reintegration into the family by also looking at community and how it’s acceptance or refusal of the child or young person impacts reintegration.
With a growing evidence base as a foundation and justification, policy makers, practitioners and those with care experience are pushing governments and other actors to decrease reliance on and use of residential care for children. Yet together with this effort, is the need to develop tools, processes, services, and evidence that helps the sector determine which elements or interventions contribute to successful reintegration outcomes for children and families. If residential care is closed or transitioned to non-residential services, this will result in a significant number of children in care being reunified into families. Therefore, practitioners and policy makers need tools and processes in place that are designed to support both a safe initial process and a successful outcome. Simply taking a child back, into a family is not enough. The sector needs to hold itself accountable, supporting children and families to reintegrate fully and safely, and be able to measure and demonstrate that a reintegration is successful.
Reintegration work is greatly informed by an ecological framework (Bronfenbrenner, 1979). This recognizes that a community is a dynamic system, constantly changing and interacting with other systems, such as the family. It is made up of people who share certain customs, attitudes, communication codes, beliefs, cultural patterns, and expectations. According to these ideas, when analyzing the development of children, one cannot look at a child in isolation, but also as a part of and influenced by the family and the community in which s/he develops. The relationships and intersections between the child, the family and the community are understood as a central factor for integral development (www.CampusEducación.com). This thinking has informed, for example, the different domains of the Star Model of Child and Family Wellbeing, which includes different elements of wellbeing recognizing the intersections between child/family/community across many of those domains (Catholic Relief Services, 2017; Changing the Way We Care, 2020; Goldman et al., 2020).
The Star Model of Child and Family Wellbeing was used by Retrak in Uganda and later adapted for use in Uganda by Catholic Relief Services for the Keeping Children in Healthy and Protective Families project (Catholic Relief Services, 2017; Goldman et al., 2020). In 2019, it was further contextualized for use in Kenya and then in Guatemala. In each context there are six domains of child and family wellbeing, however, they vary slightly in terms of domain names and indicators of success in each of those domains. The six domains include: child health and development; child protection and safety; education access, quality and achievement, psychosocial health of child and parent/caregiver; child-parent/caregiver relationship and attachment; and social and community acceptance. (Catholic Relief Services, 2017; Changing the Way We Care, 2020; Goldman et al., 2020). In the case of Guatemala (Figure 1), two domains were slightly different than the above: one focused on psychosocial wellbeing and community connection and another one addressed economic stability (Changing the Way We Care, 2020).
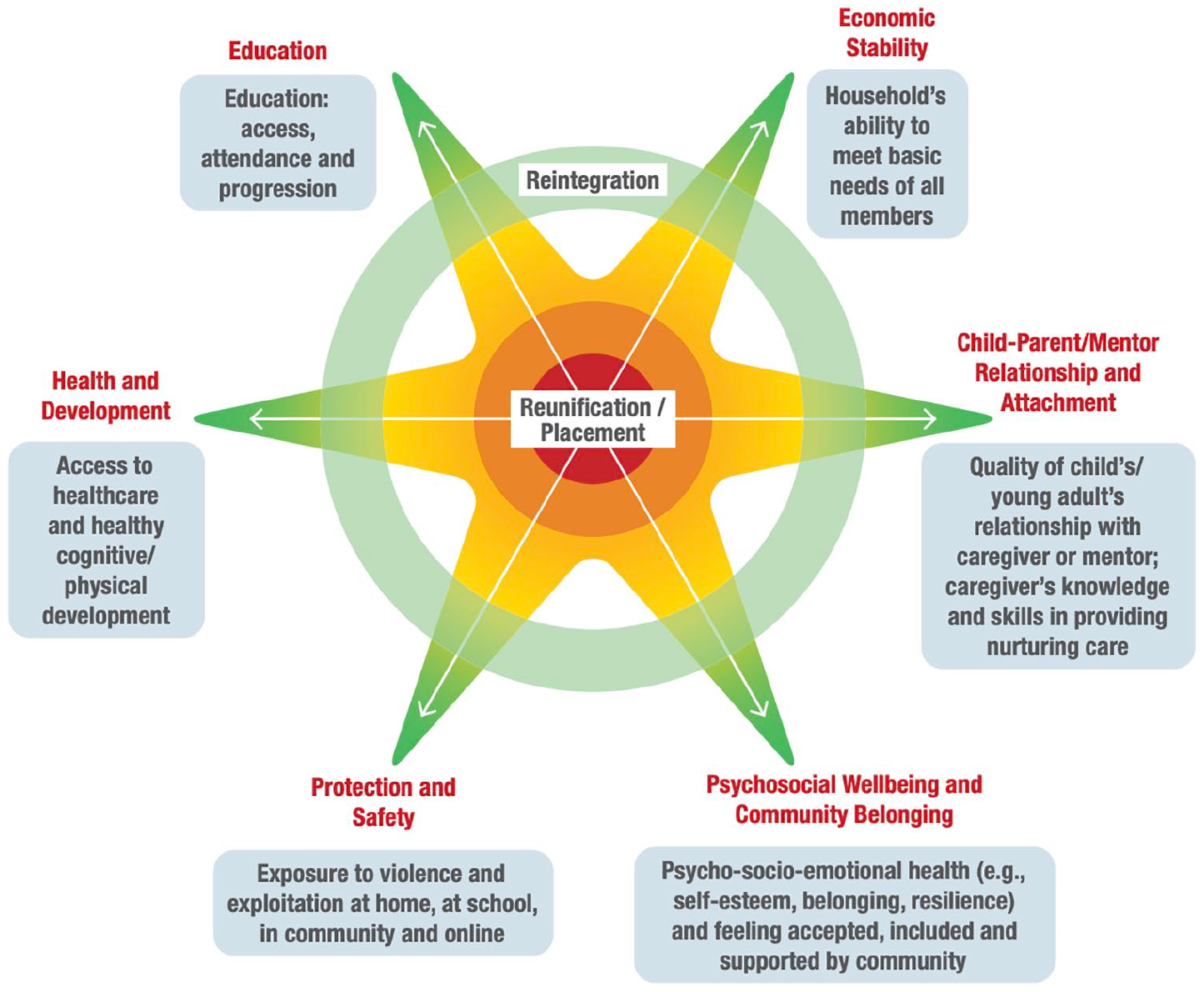
Star model of child and family wellbeing.
Each domain includes a set of discrete indicators that illustrate what “success” looks like under the domain and is informed by context. In the case of Kenya and Guatemala, those indicators were designed in a participatory manner by key actors engaged in child protection and care (Changing the Way We Care, 2020). In the case of psychosocial wellbeing and community belonging, referred to as community connection throughout this article, the domain is defined as children’s and caregivers’ psychological health and wellbeing, and socio-emotional functioning, including self-esteem, resilience, and belonging. Additionally, the domain looks at child and caregiver’s feelings of acceptance, belonging, inclusion, and support within the community, and issues of stigma or discrimination that might inhibit a child’s active engagement and inclusion in the family and community.
The care system in Guatemala
A 2019 national census of residential care facilities identified 3863 children in residential care (Organismo Judicial y la Procuraderia General de la Nacion, 2019). The top reasons for placement were poverty, social risk, negligence, and violence. Furthermore, the census identified that 97% of children in residential care had at least one living relative, clearly indicating the possibility of reintegration if appropriate processes and services are in place to support the child and family before, during and after reintegration (Organismo Judicial y la Procuraderia General de la Nacion, 2019).
Whilst Guatemala has a rights-based legal framework that provides a critical set of building blocks for a comprehensive child protection system (Congreso de Guatemala, 2003; United Nations General Assembly, 1989), placement of children into residential care is still used as a frequent response to child vulnerability. The Law for the Comprehensive Protection of Children and Adolescents (passed in 2003 and henceforth referred to by its Spanish acronym the PINA Law), delineates the role of the State in strengthening families and protecting children. The PINA Law establishes a broad array of rights for Guatemala’s children, which include both protection from violence and the right to a family. Despite these legal tools, there remain significant gaps in terms of addressing the root causes that drive children to be separated, preventing that separation, and strengthening family-based care.
Over the past 15 years, Guatemala has had several internationally funded projects focused on the reintegration of children. However, these have primarily been implemented by non-governmental organizations or UNICEF and have not been national in scope. The projects have been designed to focus on a specific geographic area or a specific group of children (e.g. 0–3 years). Awareness of the dire situation of children in residential care in Guatemala was brought to the forefront after the deadly fire at a government residential care facility in 2017 in which 42 girls died (Wirtz and Ahmed, March 8, 2017).
The Changing the Way We Care initiative (CTWWC) is implemented by Catholic Relief Services and Maestral International, along with other global, national, and local partners working together to change the way we care for children around the world. In Guatemala, the initiative started work on reintegration in the eastern part of Guatemala in the department of Zacapa, in 2019. The initiative utilizes a case management process to guide the identification, assessment, planning, follow up and eventual closure of cases from preparation for reunification, the actual process of reunification, and a completed successful reintegration (Changing the Way We Care, 2020; Global Social Service Workforce Alliance, 2018; Inter-Agency Group on Children’s Reintegration, 2016). The case management tools, standard operating procedures and case worker training have been informed by and designed to reflect the different domains of the Star Model and include 18–24 months of follow up with the child and family to ensure that all the domains are sustainable for the family. The care plan is used as a road map and is updated based on the strengths and needs of the family and the process toward reaching the agreed-upon domains (Changing the Way We Care, 2020).
An important element in the case management process is protective factors within the family and within the community. Informed by evidence as well as experience, the way in which a community responds to and accepts a child and family who are reintegrating can influence the self-esteem of the reunified child. One study found that caseworkers often paid particular attention to acceptance by and integration of the child and family into the community (Akello et al., 2006; Betancourt et al., 2010; Pryce et al., 2015). Feeling a part of something bigger and having a sense of connectedness with and acceptance by the school, church, neighbors, peer groups, other parents/caregivers, or community leaders can contribute to successful reintegration outcomes and counter those that can hinder the process. This study aimed to look more in depth at the role that community connectedness played within the lives of 36 Guatemalan children and their families. Community connectedness was explored both as part of the initial separation of the child as well as during the reintegration process.
Methodology
This study is based on the analysis of 20 case files, involving 36 children, of whom 22 were boys, and 14 were girls. Some files included sibling groups recorded in the same file. The children were aged between one and 16 years old. Of the 36 children, 27 have been reunified with biological parent(s), eight with extended family, and one child with “fictive kin” that is, a person well known to the child and biological family. There were 23 parents or caregivers caring for the children, comprised of 15 women aged 23 to 50 years old, three women aged 60 years and older, three men aged 28–50 years old, and two men aged 60 years and older. All the children and their families were part of the Changing the Way We Care initiative in Guatemala. They were selected because they were the first completed cases of reintegration. At the time of writing, all the cases had been in the case management process for 18 months or more. The authors were directly involved in the design and oversight of the case management system and tools.
The sample size included in this study is small and is from only one geographic area in Guatemala. The data are therefore not representative of the cultural and ethnic diversity of Guatemala but only of one small sub-section. Furthermore, the analysis has been drawn from existing case files, rather than through a formal data collection process. The findings are drawn from the professional experience of those involved in the process.
Data collection included a review of each case file and individual interviews with members of the multidisciplinary teams (social worker and psychologist) responsible for managing each case. Each file included a child identification form, psychological evaluation of the child, socioeconomic and psychological evaluations of the parents or caregivers with whom the child was reunified, a child and family/caregiver care plan, and follow-up forms. Child placement processes and decisions are led by the court, including reunification. Legal documents including copies of the judicial orders were included in the file review. Because the case files were dense, the document review was conducted using a targeted lens on community connectedness with the following questions to guide the process:
▪ What was the cause of family separation?
▪ Did the child or parent/caregiver have connections to community? If so, with whom?
▪ During the case management process, were actions identified to create or strengthen links to community support and if so, which type was identified?
▪ Was community support essential in the success of the reintegration and how?
▪ Do children demonstrate belonging to their family and community environment and if so, how?
After the document review, key informant interviews were held with the social workers and psychologists who directly engaged with sample children and families. The interview questions explored issues related to success factors, use of the reintegration criteria, challenges, successes, and lessons learned during the reintegration process and key competencies required for those working with children and families who have been separated.
Findings and discussion
Causes of separation and placement into residential care
Reason for admission into residential care is an important consideration in this research study, as it informs the type of interventions needed and issues to be addressed before, during and after the reintegration process. It can show if disconnect from community contributed to separation. Of the 36 cases, negligence was the primary cause of entry into the residential care; two cases had “social risk” as the main reason, and one was physical abuse. Social risk is defined as “the conditions of the child’s environment that present an imminent risk of suffering if the child remains here. These risks often involve economic conditions, environmental pollution, drug use, poor access to social services, street life or gang affiliation, among others (Porto and Gardey, 2014).
Among the causes influencing eventual separation and placement into care, three cases had main causes that in some ways were connected to limited community knowledge about or engagement with the parent/caregiver. In these cases, children were left alone when the parent/caregiver went to work. The neighbors were concerned and called the authorities who declared neglect and removed the children from the family. Whilst it is important to acknowledge that the children were left alone, what is also important, if viewed through a community connectedness lens, is that the there was no connection between the parent, child, and neighbors. The neighbors were not aware of the unique situation of the parent, nor did the parent try to get to know the neighbors, explain the situation, and potentially ask for help in watching the children. As will be discussed further in this article, when the children were reunified an important part of the process was helping the parent/caregiver establish relationships with neighbors and community leaders. Ensuring that the children also have connections with members of their community has become an important part of the reintegration plan as a social safety net that could be called upon for support, if needed.
Community connectedness in case planning
Each of the 36 cases had individualized care plans. The domains that were the most cited as in need of strengthening were protection and security, education, and affective bonding. However, the multidisciplinary team involved in the cases recognized community belonging as its own domain, but also found elements of community connections are woven throughout the other domains. Community connectedness is cross cutting. When the multidisciplinary team reviewed each of the domains within the case plan and during follow up, they used a community connectedness lens. For example, the protection and safety domains are one of the ways to determine if children are safe. With a community connectedness lens, this becomes about knowing who neighbors are, identifying risky and safe locations within the neighborhood, and ensuring that the child and the parent/caregiver knows how to get help and from whom (police, child hotline, etc.) should a protection issue arise. All the cases had actions related to ensuring a protective environment and a relationship with neighbors as a core indicator. In the health and development domain, multidisciplinary teams would ensure that the child and parent/caregiver were connected to the local health center, for example. In communities where health centers did not exist, the team ensured linkages with community-based health workers, often accompanying the family to make introductions. Finally, the domain of healthy child-caregiver bonds is of critical importance and should be prioritized for strengthening before, during and after placement of the child back into a family environment. The team noted that this domain was achieved easier and faster for families who had established relationships with neighbors and extended family before the reunification took place. For some reasons, which should be explored further, this seemed to correlate with easier and faster attachment between the child and the parent/caregiver.
This final domain includes positive social-emotional functioning of the child and parent/caregiver, including self-esteem, resilience, and a sense of belonging. It looks at feelings of acceptance, inclusion, and support of the child and family within the community. The multidisciplinary team conducts an in-depth review of the community in which the child will be reunified, with the aim of achieving or strengthening the sense of belonging in the community. This is especially important in cases where the child has been separated from his or her family and community environment for a long time. The issue of stigma or discrimination against the child because he or she was in residential care and therefore assumed to be delinquent or was presumed to have a challenging behavior is something that must be addressed. The multidisciplinary team works closely with the family, extended family, schools, and other community actors to dispel these beliefs and work toward creating positive attitudes about the child and promoting compassion and understanding about the situation.
When care planning begins, the multidisciplinary teams conduct home visits to locate the family home within its community. The team visits the nearest school and health center. The team also locates churches, community development committees, and community leaders and volunteers that might be a possible support to the family during the reintegration process. These individuals, groups and organizations can provide support in an emergency, offer guidance on specific issues, watch for issues and proactively intervene, or address potential stigma toward the parent/caregiver or child as that is common amongst families who have been engaged with the protection system. Creating a conducive environment within the family home and the community is a critical part of the preparation stage and is reflected in the care plan.
“The identification of community support networks is critical for the reunification and reintegration of a child in safe family environments, even more so in those cases where reunification has been difficult because of the long time the child has been separated. In those cases, the community becomes a vital support for families and children.”
Marta Xico, social worker
The case file review and interviews found that community connectedness was often a factor missing and potentially exacerbated the child being separated. It was also a critical factor in terms of supporting families in the process of reintegration. Specifically, establishing connections with neighbors, faith-based groups, schools, and community leaders was recognized as helpful and contributed to the success of the reintegration process. In the cases where neglect was the reason for the initial separation, the multidisciplinary team engaged and worked closely with the neighbors who saw the family as “bad” because they had left their children alone. The multidisciplinary team also worked with the parent/caregiver to build their own skills and knowledge about positive parenting and child development. In one specific case where the neighbors had reported the parent for neglect, which resulted in the separation, the team reached out directly to a couple that lived in the neighborhood and were well respected. With time and perseverance, a bond was established between the two families and the neighbor family became a mentor to the parent/caregiver providing parenting advice and support. In the end, the relationship was mutually beneficial and has been an incredible support to the parent/caregiver and the child. In another case, a connection was fostered with a pastor at the church the family attended. The pastor not only helped to deliver messages about the importance of being a responsible parent, but also helped to foster a church environment that was safe, welcoming, and non-judgmental; a critical part of the family feeling accepted within and part of their community.
“The success of working with children, adolescents and families is empathy, showing that we have the same interests, guiding and re-educating parents by changing habits that can put their children at risk and the essential thing, the construction of affective bonds with their children”
Lilian López, psychologist
Examples such as these show the important role that feeling accepted by, and part of a community in its many facets, plays in terms of supporting a reintegration process. This is true for children as well as the parent/caregiver. Knowing that you are part of something bigger, you “belong” and that there are others to turn to in time of need, appears to help promote a sense of wellbeing thus contributing to a positive reintegration process. Understanding the role that community connectedness plays in reintegration can also help us better understand how a lack of it might contribute to or even exacerbate the risks of separation. In the cases explored in this article, isolation from neighbors and a lack of connection to other types of community groups seemed to be present prior to the separation of the child from his or her parent/caregiver illustrating that lack of community connection can exacerbate risks to separation. And conversely, the presence of community connectedness contributed to greater reintegration success in these cases.
Implications for practice
These initial findings from Guatemala provide insight into the role that community connectedness plays in facilitating reintegration. Recognizing the role that acceptance by, inclusion in, and engagement with different community actors and organizations or the lack thereof plays in increased risk of separation is important in designing interventions that aim to prevent child and family separation. The learning provided by these 36 cases shows that community connectedness and belonging for both the child and the parent/caregiver is an element that should be included in interventions, case management and counseling tools, case planning, and as an indicator of wellbeing to determine success. The experience from Guatemala can help governments and non-governmental organizations engaged in reintegration and prevention of separation efforts to better plan, design, monitor and implement approaches that promote, and intentionally include and foster community connectedness in all phases and in all interventions.
The Star Model has six domains of wellbeing helpful in guiding the case management process used for reintegration. It can be contextualized to reflect the unique circumstances of each context. In the case of Guatemala, using the Star Model to help define domains of wellbeing and including those elements throughout the case management process has been extremely helpful in providing practitioners with a concrete way to ensure a holistic approach to reintegration. Having the domains and ways to monitor for success has also helped the multidisciplinary teams and their supervisors to be more intentional about engaging with and fostering community connections. This has increased successful service referrals and helped organizations to work effectively together. As actors in the sector continue to move toward reintegration as part of broader care reform efforts, using tools such as the Star Model to help measure wellbeing and reintegration success will be an important part of accountability. The use of such models contributes to better practice and facilitates success for families and children.
Reintegration must be grounded in a case management process. Community connectedness can be integrated into the different steps of the case management process and their related tools. For example, specific questions about community involvement and support systems should be added to the assessment of the child and parent/caregiver. Gathering information about connections before the separation will provide insight into how to better design prevention interventions around community connectedness. Multidisciplinary teams can look at the connections that existed prior to the separation and strengthen them. Identifying new linkages helps the family prepare for reunification. The team can help the family and parent/caregiver understand why a connection to community is important to overall wellbeing and to their reintegration plan.
When developing the case plan, the multidisciplinary team can actively engage the parent/caregiver and children in identifying potential community actors or organizations with whom to connect. This can include schools, health centers, neighbors, community groups, faith institutions, and cultural groups. Once these are identified, helping the family to engage with those individuals or groups will foster the relationship between child and parent/caregiver and the community. It is important to be aware of and address any stigma and discrimination by community members about children and families who have been in the protection system through awareness raising activities, such as community dialogs. In Guatemala, there was often the perception that children who had been in residential care were “delinquent” or “bad” and that parents who had children in residential care were also “bad” or “criminal.” It is important to address these misconceptions. In several instances in Guatemala, it was also helpful to engage community members so that they felt they were part of solution.
Including community connectedness as part of the follow-up processes proved an integral part of the work in Guatemala. Highlighting how community connections supported positive outcomes not only for the family but also for the community have informed the way in which Changing the Way We Care is supporting new families in the reintegration process. It has also influenced the way in which prevention interventions are designed.
Several of the cases in Guatemala illustrated how isolation from or not engaging with neighbors can potentially contribute to separation. This area could benefit from more targeted research that explores how connection to communities might reduce cases of separation. Family support research show social connection as an important protective factor (Center for Social Policy, 2017). Similarly, there is a need to design research that looks at how and which types of community connections are most impactful to reintegration outcomes for children and families. For example, does being connected to neighbors result in better outcomes for families as compared to connections to a faith-based community? Or are outcomes better if there are connections to both? Similarly, better understanding what children view as important in terms of community connectedness would greatly contribute to a more comprehensive and child-informed approach to both prevention and reintegration programs.
Conclusion
Initial findings from reintegrated children and families in Guatemala illustrate the importance of including a holistic understanding of wellbeing, such as the Star Model, to help guide a case management process and determine or measure the success of a reintegration process. One critical element within this process, is community connectedness. Better understanding of what this looks like, which individuals, groups, or organizations should be involved, and how professionals can work intentionally to foster these connections will benefit those engaged in care reform broadly and in reintegration specifically—not only program managers and social workers, but the families themselves. Recognizing that a child is not only reintegrated back into a family but also into a community and designing interventions that foster positive connections is an important consideration for future reintegration work. Whilst more information is needed in terms of which connections are most important in terms of positive outcomes and building protective factors, what is clear is that a sense of connectedness and the establishment of concrete linkages to community actors and groups contributes to child and parent/caregivers’ wellbeing, which in turn leads to sustainable and safe reintegration.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.