
Abstract
There is limited evidence on family reintegration for children who have been in residential care within the African context. The goal of this study is to find out what factors impact reintegrated institutionalized children’s desire to remain with their biological parents or extended family. The dataset included records for 659 interviewed children and their guardians. However, the analyses were limited to 408 cases with complete data on the dependent and independent variables. Most of the children in the study (73%) preferred to remain with their relatives. The age of the child, length of time spent in residential care, and having a case file, were all factors linked to the children’s wish to stay with their family. Based on the findings of the study, social workers should do a full assessment and documentation to decide if reintegration is appropriate, prepare the child and family, and give follow-up assistance to ensure stable reintegration. Social workers must also link reunified families to long-term support such as enrollment on the Livelihood Empowerment against Poverty social protection program, and they should monitor placements to improve the stability of the reintegration.
Introduction
Around the world, estimates suggest that between two and nine million children live in residential homes for children (RHC) such as orphanages and children’s homes (Desmond et al., 2020; Petrowski et al., 2017). Most RHCs are in developing countries in Africa, Asia, and Latin America, where they are the main formal alternative care option for orphans and separated children (OSC) despite data, particularly from industrialized countries, showing that they hinder healthy child development and cause significant delays in several developmental areas (Roche, 2019; Van IJzendoorn et al., 2020).
Because of their harmful effects on children, international and national child welfare laws (such as the UN Convention on the Rights of the Child and Ghana’s 1998 Children’s Act) emphasize that OSC in institutional care should be returned to their parents and families as soon as possible. To actualize the tenets of the UNCRC for children in alternative care, the UN Guidelines for the Alternative Care of Children recommends that, when it is in their best interest, children in care should live in a family environment, either through family reintegration or placement in a foster or adoptive family. As a result, several African countries, including Kenya, Rwanda, and Malawi, have restructured their child welfare systems. The reforms attempt to shift the focus away from residential care and onto family-based care as an alternative to residential care for OSC (Davidson et al., 2017; Frimpong-Manso, 2014; Horvath et al., 2019; Murthi and Jayasooriya, 2020).
Child welfare reform in Ghana began in 2006, following a government survey that found a fast growth in the number of children in residential care despite placement in these institutions intended to be a last resort among the alternative care options prescribed by the Children’s Act (Frimpong-Manso, 2014). Residential care is a temporary placement for children (below the age of 18 years). As most children in RHCs have at least one living parent or extended family member, family reintegration is an important aspect of the reform. The RHC, therefore, has a duty to actively participate in DSW’s activities to reunify the children in their care with their parents. According to the most recent numbers, the Department of Social Welfare (DSW), which handles the care and protection of children in Ghana, has reintegrated 1577 OSC in RHC (Better Care Network & UNICEF, 2015).
The nascent research on African countries (e.g., Frimpong-Manso and Bugyei, 2019; Gomera and Mutambara, 2020; James et al., 2017; Severine et al., 2020) show that children in institutions who reunify with their families often experience physical and socio-economic challenges, including educational issues, inadequate living conditions, and stigma. Several factors cause the problems faced by the reunified families. Pressure from international organizations and donors to carry out non-institutionalized care has led to family reunification when the children, their families, and childcare systems are not yet ready (Frimpong-Manso, 2014; Murthi and Jayasooriya, 2020). During the reintegration process, the child’s wishes are often not considered (Frimpong-Manso and Bugyei, 2019; Mahuntse, 2015), and social workers lack financial and human resources to offer follow-up services to the reunited families (Chadambuka and Chikadzi, 2020; Potgieter and Hoosain, 2018). These challenges lead to repeated separations and re-institutionalization of reunified children (Bunkers and Keshavarzian, 2015).
Although reintegration of children from RHC into families has received frequent scholarly attention in other parts of the world, the same conclusions are hard to be drawn on the subject in sub-Saharan Africa. In Ghana, which is the setting for this study, investigations into the factors that influence the stability of family reintegration for children who have been in residential care are limited. For example, we know little about the factors that impact whether children want to stay with their reintegrated families or return to residential care. The goal of this study is to find out what factors impact reintegrated institutionalized children’s desire to remain with their biological parents or extended family.
International literature on family reintegration
Family reintegration is regarded as the best way out of the alternative care system for children (Chartier and Blavier, 2021). Because reintegration is intended to serve the best interests of the children, social workers and other experts involved in the process must make difficult decisions concerning its suitability and feasibility (Biehal et al., 2015). Several studies conducted on family reunification of children in care outside Africa have investigated the factors associated with reintegration. The available international research implies that a child’s age affects family reunification, although the evidence is conflicting. While some research implies that younger children have a reduced chance of reuniting with their families (e.g. López et al., 2013; Neil et al., 2020), other research suggests that older children have a lower chance of reuniting with their families (e.g. Murphy and Fairtlough, 2015; Žunić-Pavlović et al., 2021).
Furthermore, family reunification occurs at a higher rate within the first few years (up to 3 years) of a child’s placement in care (Goemans et al., 2016; Martin et al., 2020), especially when placements are stable (Murphy and Fairtlough, 2015). Other factors that increase the likelihood of reunification include the child’s parent’s access and engagement with pre-reunification services (e.g. problem-targeted parenting classes and counseling services) (D’Andrade and Nguyen, 2014; Giallo et al., 2020). Evidence from some African countries have shown that children in care are more likely to be reintegrated when community sensitization about the negative effects of institutionalization is undertaken, the children and their families accept the reintegration, and the families are economically empowered (Catholic Relief Services, 2016; Kuehr, 2015). According to Delap and Wedge (2016), casework and case management are crucial approaches and evidence-based practices in the reintegration of children. They entail assigning a social worker to the child and family, who provides individualized support and documents the process.
Farmer and Wijedasa (2013) define a stable reintegration as when a child continues to live with the parent or family for at least 2 years. However, not all family reintegration is stable, as some children re-enter care or become separated because of several risk factors. Child-related factors associated with unstable reintegration comprise children’s emotional and behavioral challenges and unhealthy relationships with parents (Akin et al., 2017; Brown et al., 2020; Font et al., 2018). According to several authors (Hébert et al., 2018; Mc Grath-Lone et al., 2017), reunification after a brief term in care rarely allows for resolving hazards at home, which contributes to re-entry into care.
Many children return to parents who have several co-occurring problems, such as poverty, substance abuse, and housing challenges, which are unresolved and lower the probability of the reintegration being stable (Marcenko et al., 2011). This situation often happens when reunification occurs against the advice of social workers (Goering and Shaw, 2017) or there is a lack of services (Stephens et al., 2017). However, access to professional services and trusted social support is one criterion that ensures stable family reintegration (Balsells et al., 2015; Giallo et al., 2020; Lietz et al., 2011).
Formal services (e.g. home visiting and family coach) provide instructional, information, and advocacy support that help parents overcome personal and structural barriers that impede reintegration (Akin et al., 2017; Lalayants, 2020). For example, Rushovich et al. (2021) reviewed the success coach post-reunification program in North Carolina in the US. The authors found that just one child out of nine who enrolled and received the intervention re-entered care and that the parents were very positive about the services they received. Other characteristics that prevent re-entry into care include the child’s ability to maintain constant contact with their parents during their time in care, the willingness and preparedness of the child and parent to reunite, and adequate preparation before reunification (Farmer and Wijedasa, 2013; Jedwab et al., 2018; LaBrenz et al., 2020).
Methods
The Social History and Post-reunification Survey of Children Reintegrated by DSW dataset was used (SHPSCR-DSW). The survey’s purpose was to learn what factors influence reintegrated institutionalized children’s desire to stay with their original parents or extended family. 659 children and their guardians were contacted and interviewed in total.
Data collection
Between 2013 and 2017, the DSW and UNICEF-Ghana, cooperating with two Ghanaian NGOs, tracked and gathered statistics on children reintegrated into their nuclear or extended families. To locate the reintegrated children, the two NGOs hired and trained enumerators and partnered with DSW and RHCs. Data collection occurred between June and October of 2017. We conducted separate interviews with the children and their guardians. At all times, we respected the privacy of the participants. Prior to interviewing the children, we gained their assent while the adults provided consent. The interview lasted between 45 minutes and an hour on average.
Analytic sample
We restricted the analyses to completed respondents’ data on the dependent and independent variables. Therefore, the analytic sample size for the study was 408.
Measures
Dependent variable
We have identified the following variable as a proxy for reintegrated children’s preference for staying with their families over the RHC: child prefer the RHC to their current family with a “Yes” or “No” response.
Independent variables
The following variables were identified as potential explanatory factors associated with children who are more likely to declare their preference for staying with their families after their reintegration: child-level factors (gender, age, duration of stay at RHC, preparation of the child before reunification—receipt of reintegration certificate, availability of a case file on the child), caregiver factors (receipt of reintegration package, supervisory activity from Department of Social Welfare), home factors (sanitation facilities, child’s engagement in income generating activity at home), and community factors (child’s participation in community activities). The content of the reintegration package depends on the family situation of the reunified child and the capacity of the organization offering it, usually the residential care facility. It can contain non-perishable food items (e.g. rice, oil, and biscuits), school items, cooking pots, mattresses, clothes, and sanitary pads).
Each child in a RHC should have a case file that includes the following documents: court order, social enquiry report/assessment, emergency contact information for parents/family, care plan with reviews and updates, case notes, school progress reports, medical records and important health information on the child, birth certificate; and any other relevant documents. A reintegration certificate verifies the DSW has reunited a child with his or her family.
Data analysis
Frequency and percentages were used to describe study sample. We assessed the relationship between the dependent variable and the independent variables using the Chi-Square test of independence. Both chi-square test of independence (to generate a cross-tabulated frequencies) and bivariable robust Poisson regression were used to determine the association between the outcome variable and thirteen potential explanatory variables. A p-value of 0.05 was used to identify the explanatory variables from the bivariable robust Poisson regression analysis to build a multivariable regression model. We build our multivariable model using a log-linear model implemented through a Poisson regression model with a robust variance estimator (also known as modified Poisson regression) (Zou, 2004). This is recommended over the go-to binary logistic regression when the prevalence of interest in the dependent variable exceeds the threshold of 13% (Barros and Hirakata, 2003; Santos et al., 2008; Zou and Donner, 2013). Using the binary logistic regression in the forgoing situation often results in bias estimation of the standard errors and the interpretation of the odds ratios can be misleading (Barros and Hirakata, 2003; Santos et al., 2008; Zou and Donner, 2013).
Results
Sample description
Table 1 presents the description of the sample using cross-tabulation (frequencies and percentages) and results from the chi-square test of independence. About seven out of ten reintegrated children (73%) prefer to stay with their families than returned to the RHC. The males (53.19%) in the sample were more than the female (46.81%). The proportion of females (75.92%) who prefer staying with the reintegrated family was slightly higher than that of males (70.05%). Most of the reintegrated children were in school (88.48%). Approximately eight out of ten children were reunited with their primary carers. Many of the children had been in a RHC for 4 years (30%). When children spend more years at the RHC, the percentage of youngsters who prefer their family to the RHC falls. Most of the youngsters (65.44%) take part in household income-generating activities, community events, and activities (80.15%). Almost half of the children in the sample had a file with the RHC (45.59%). The case file is a folder containing the case management forms and a series of documents related to the child (e.g. Police extract, court order, insurance cards, reports from school, birth certificates, medical reports, etc.)
Summary statistics of study variables.
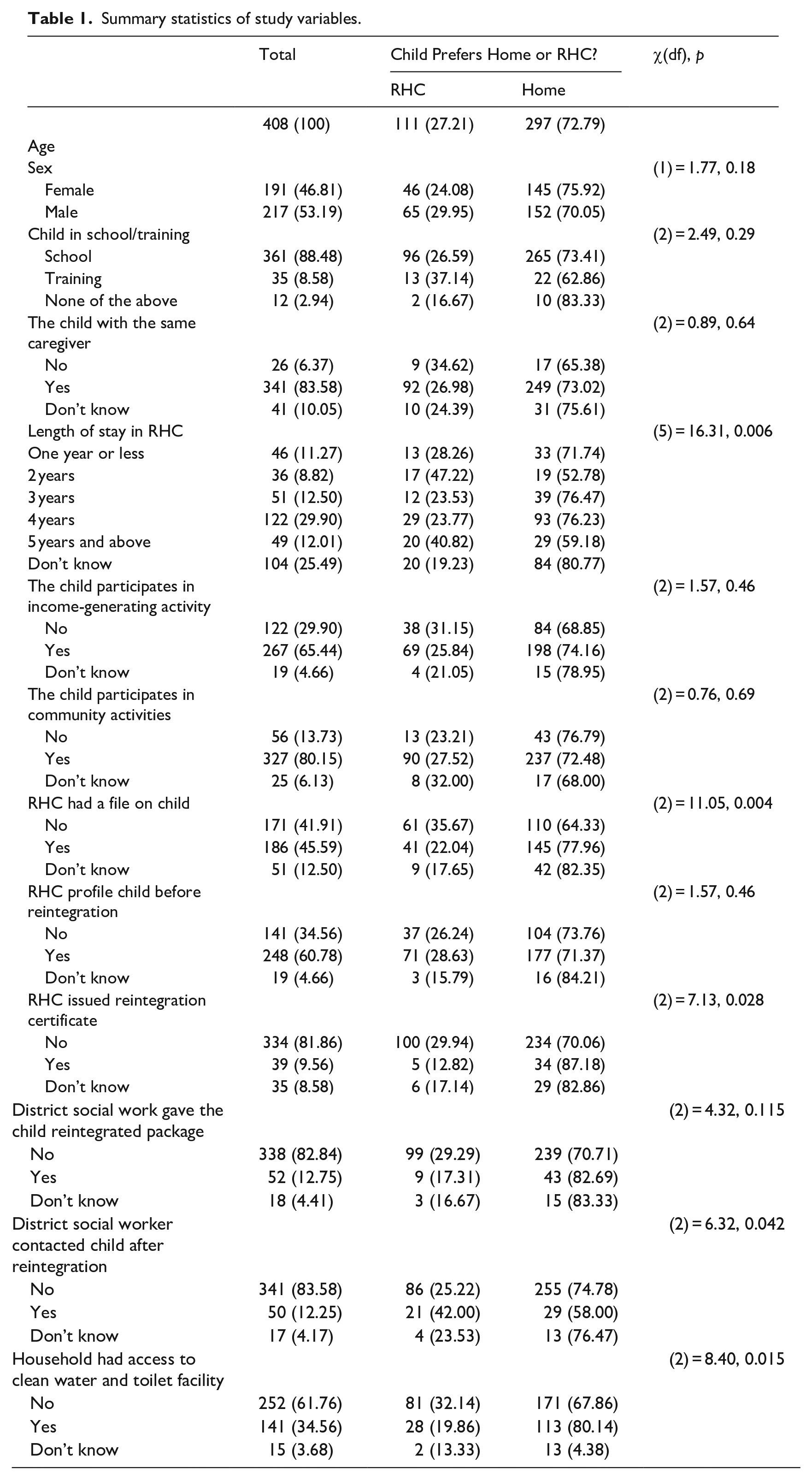
The proportion of children with a file at an RHC (77.96%) who preferred the family to the RHC was slightly higher than those without a file (64.33%). About six out of ten children were profiled before reintegration with their families. The DSW issued only 39 out of 408 children with a reintegration certificate. Out of 408 reunified children, 52 received a reintegration package. A district social worker followed up on 50 of the reunified children. Approximately 34% of the reintegrated children lived in families with running water and toilets, and most of them (80%) prefer their home to the RHC.
The tests of association results indicated that the following explanatory variables met the statistical significance threshold: sex of the age (Table 2 used modified Poisson regression), sex, length of stay in an RHC, children who had a file at an RHC, children who were issued reintegration certificate, district social work gave child reintegrated package, district social worker contacted child after reintegration, and household had access to clean water and toilet facility (Table 1).
Correlates of reintegrated children’s preference for home over the RHC.
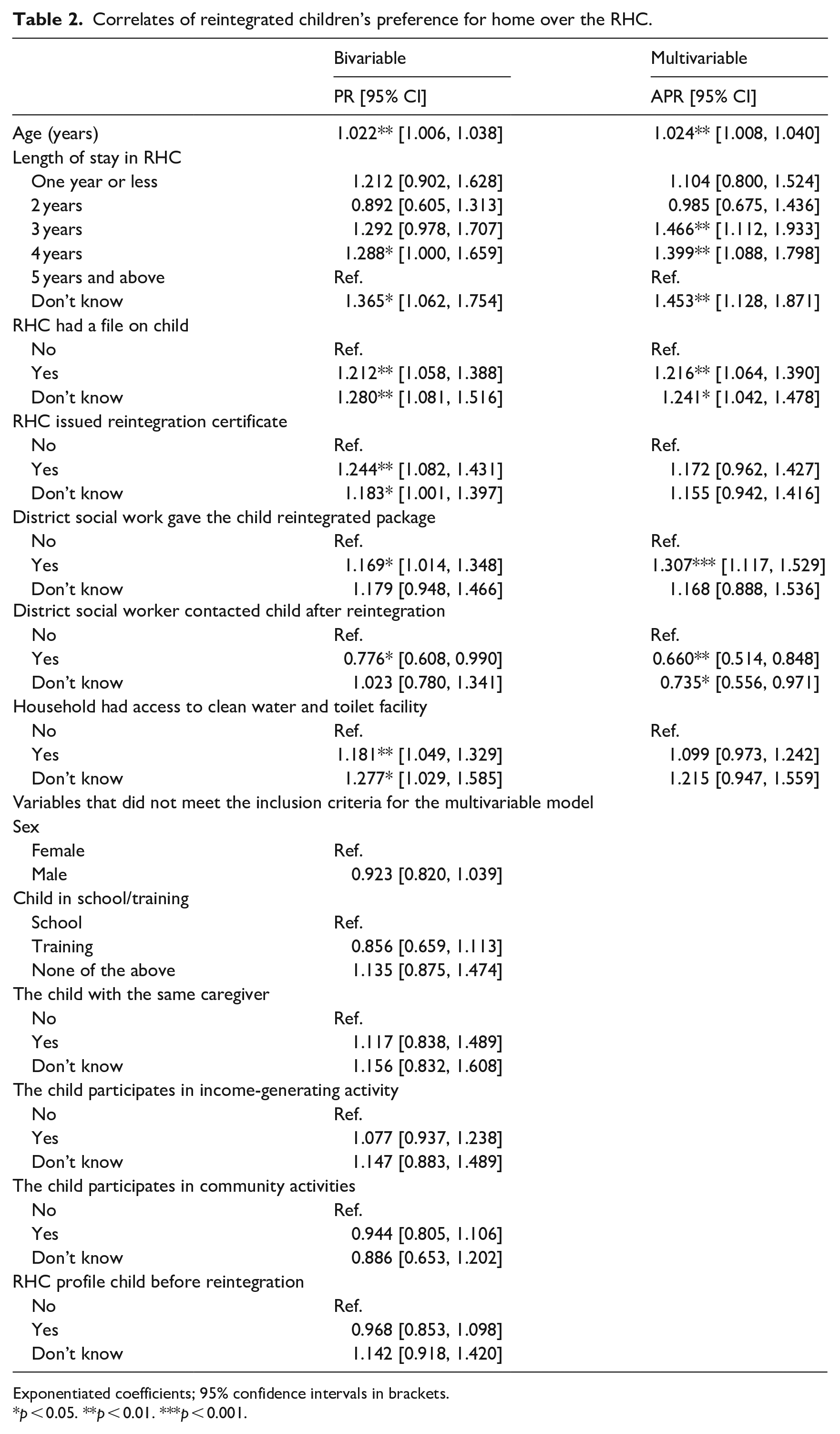
Exponentiated coefficients; 95% confidence intervals in brackets.
p < 0.05. **p < 0.01. ***p < 0.001.
Correlates of reintegrated children’s preference for home over the RHC
Table 2 shows the unadjusted and adjusted models of the correlates of reintegrated children’s preference for home over the RHC. An unadjusted model of regression analysis between the dependent variable and one independent variable. An adjusted model is a regression analysis between the dependent variable and multiple variables in the model. The significant results from the adjusted models are interpreted here. One unit increase in age was associated with a higher likelihood of a reintegrated child preferring to stay with the family over the RHC (APR = 1.024, 95% CI: 1.008, 1.040). Compared to children who had spent 5 years and more in an RHC, those who spent 3 years (APR = 1.466, 95% CI: 1.112, 1.933) or 4 years (APR = 1.399, 95% CI: 1.088, 1.798) were more likely to report that they prefer to stay with their family over the RHC. Compared to children on whom there was no file at the RHC, children who had a file at the RHC were more likely to report a preference to stay with their family over the RHC (APR = 1.216, 95% CI: 1.064, 1.390). Children who received a reintegration package from the district social welfare department were more likely to prefer staying with the family over the RHC (APR = 1.307, 95% CI: 1.117, 1.529) compared to those who did not receive a package. Compared to children who were not contacted by a social worker after the reintegration, those who were contacted were associated with a lower likelihood of reporting a preference for staying with the family over the RHC (APR = 0.660, 95% CI: 0.514, 0.848).
Discussion
This research sought to find out the factors that impacted reintegrated institutionalized children’s desire to remain with their biological parents or extended family. Most of the children in the survey (73%) prefer to live with their families and not in residential homes. From the findings, the age of the child, length of stay in the RHC, existence of the child’s case file, receipt of a reunification package, and social worker monitoring visits are factors that influence reintegration stability. Children were more likely to want to stay with their families if they were older. It is probable that the older children value and appreciate the independence that reuniting with their parents or extended families provides, as opposed to the rigid timetables that many RHCs impose (Islam and Fulcher, 2021). The families the children reintegrate to may accept the older ones more with the consideration that they can contribute to income-generating activities of the family. An interesting finding was that children monitored by a social worker were rather the ones who wanted to return to the RHC, a finding that contradicts existing research which shows that social workers positively support the reintegration process (e.g. Akin et al., 2017; Lalayants, 2020). It is probable that the social workers’ visits reminded the children of the RHC and rekindled their hope for a return, especially if they lacked essential resources like food and education, which is an issue for many reunified children in Ghana (James et al., 2017). Earlier Ghanaian research (Frimpong-Manso and Bugyei, 2019;) has shown that social workers often cannot also provide these basic resources to reunified families because of limited financial resources. Another possible reason is that, because monitoring of the reunification is mostly done by RHC social workers in Ghana and other developing countries (De Bruin Cardoso et al., 2020), those opposed to deinstitutionalization and reunifications may be encouraging the children to want to return to the residential institutions. This finding, however, requires more investigation in a qualitative study.
Another finding was that the length of the child’s stay in residential care was related to his or her preference for staying with the family rather than in an RHC. Similar to existing research (Martin et al., 2020; Murphy and Fairtlough, 2015; Žunić-Pavlović et al., 2021), those who spent less time in care were more likely to choose to remain at home with their parents and extended families than in a residential home. Some African studies (e.g., Horvath, 2019; Potgieter and Hoosain, 2018; Severine et al., 2020) demonstrate that children who stay in care for an extended period have less contact with their parents and extended family members. Because the institutions are frequently located outside of the children’s local neighborhoods, and other logistical obstacles, such as the lack of telephones, make communication difficult, this predicament arises. This situation results in weaker emotional ties and relationships between the children and their biological families and parents who feel less responsible for raising the child, making it difficult for the child to adjust after reunification. This finding supports the use of alternative care for children for short periods of time, as proposed by both the Ghanaian Children’s Act of 1998 and in the UN Guidelines for the Alternative Care of Children (2010)
To achieve this, social workers working in both the RHCs and the district assembly should support the child and the family at each step of the case management from when the case is open and immediately after a child’s placement in care by to the time when there is a stable reintegration and the case can be closed. Several factors relating to the reunification process also influenced whether the children wanted to stay at home or return to the residential home. If children had a case file and were granted a reunification certificate before leaving care, they were more likely to desire to stay with their family after reintegration, comparable to the findings of Farmer and Wijedasa (2013) in the UK. Farmer and Wijedasa explain that children with case files have rigorous consideration and planning involving preparation which ensures resolution of all major issues before reunification. The participants also linked the provision of a reintegration package with a stable reintegration. Reunification support is critical in reuniting children with their families, particularly in low-income nations, because many of the families with whom the children reunify face financial challenges and have large families. This implies they frequently cannot meet the children’s basic requirements (e.g. education, health, and food), which increases the likelihood of children being abused or exploited (Frimpong-Manso and Bugyei, 2019; James et al., 2017).
The quality of care and case management services, provided by social workers at the residential homes and at the district level, were proxies for adequate preparation before reunification. These findings are testaments of the proven belief that adequate preparation before reunification can prove positive. Case management is an important approach in realizing stable reintegration efforts because it involves the assignment of a caseworker to the child and family to provide individualized support and to document the reintegration process (Inter-agency group on Children’s Reintegration 2016).
However, evidence shows that only half of the children in RHCs have an assigned caseworker from DSW while about one-third are without an individual care plan, and one of three children still do not have a court order for their placement in residential care (DSW and UNICEF, 2021). The lack of casework practice and involvement of the District social welfare officers in the case management of children in RHC and their participation in the development of care plans undermines the possibility of these children being reintegrated in their family (Frimpong-Manso and Bugyei, 2019). Similar research in Ghana (Frimpong-Manso and Bugyei, 2019) found that children and their families were ill-prepared for reunification.
Limitations
Because the study’s main findings are correlational, we must interpret them considering this constraint. The 251 children eliminated from the study due to considerably inadequate data may have altered the dynamics of the estimated prevalence and the coefficients of the relationships. We consider the conclusions based on the total data provided as a preliminary insight because data on the subject under inquiry is scarce. As a result, we propose a well-planned study with few missing instances. To the best of the authors’ knowledge, this is the first study to look at the factors that influence the stability of family reunion in a developing country, such as reintegrated children’s preference for staying with their families versus a residential care facility. As a result, policymakers and experts working in deinstitutionalization and reunification efforts in Ghana and other countries with similar socioeconomic situations will find the ideas valuable.
Recommendations and conclusion
In Ghana, child welfare regulations emphasize that a safe family presents the best setting for children’s growth and development. As a result, one of the targets of Ghana’s care reform project is to reduce the number of children in institutions and, when feasible, reintegrate them into their families. The outcomes of this study emphasize the significance of enhancing the current case management system, which assists children and families at every stage of the reintegration process.
Caseworkers of the DSW and Community Development at a decentralized level and the social workers at the residential care facilities need to be actively involved in all steps of the case management (assessment, case planning, monitoring) to ensure stable reintegration. It necessitates pre-reintegration casework with children and families, a thorough assessment to determine the appropriateness of reintegration, child and family preparation, reunification, and follow-up assistance. The children’s capacity to reintegrate permanently with their families and communities is jeopardized if sufficient case management services are not provided. The government should ensure that the DSW’s workload is manageable so that case management work can be completed and stable reunifications can be achieved.
District social workers must ensure that each child undergoing reunification receives a discharge package suited to their personal and family requirements, based on the findings of this study. This could include enrolling reunified families in long-term support programs (e.g. cash transfers through LEAP and health insurance) as well as other community-based resources like extended family support, which has been shown to improve the capacity of vulnerable Ghanaian families to care for their children and avoid unwanted separation (Frimpong-Manso and Bugyei, 2019).
Social workers within the districts where the children are reunified should regularly monitor them to ensure they are safe and track progress. Given that social workers often struggle to undertake this task due to limited staffing, funding, and other resources such as transportation (Chadambuka and Chikadzi, 2020). Social workers can therefore partner with local NGOs and faith-based agencies who have the resources to undertake this task. In terms of research implications, future studies could look into whether there is a statistical difference between reintegrating with family members from whom the child was removed and reintegrating with extended relatives with whom the child is being cared for the first time.
Role of the authors in generating the data and its analyses
The first author is a senior lecturer with the Department of Social Work at the University of Ghana. He holds a PhD in Social Work from Queen’s University of Belfast and has taught social work at the University of Ghana for the past 15 years. His research interests are in children and families, alternative care for children, care leaving and deinstitutionalization. The second author is a staff of UNICEF-Ghana. He holds a PhD in Sociology from the University of Louvain in Belgium. He was involved in the design of the data collection instruments and supervised the work of the two NGOs that were hired to undertake the data collection. The third author has a degree in social work and a master’s degree in health promotion. He was responsible for the cleaning and analyses of the data. He was not involved in the data collection and could not influence how the data were collected. Also, he is not a practicing social worker.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.