
Abstract
Accurate data on the extent to which residential homes for children in Ghana are in compliance with national standards for quality of care and case management are lacking. To begin to address this gap, a census of residential homes and an enumeration of the child population were undertaken in 2019, followed by a survey on a representative sample of children living in such homes. Data were gathered on the types and characteristics of all 139 residential homes operating in the country at the time and the demographic profiles and well-being of children living in such facilities. The purpose of this article is to provide information on the residential care facilities that operate in Ghana in terms of their licensing status, staffing, child safeguarding, and protection policies, as well as the safety and suitability of the premises. The article also describes the demographic profiles of the children who live in such facilities and provides an overview of the care they received and their well-being. The paper concludes with a discussion of the implications of the findings within the national context and policies on children in residential care in order to demonstrate how results are being used to inform care reform efforts and systems strengthening in Ghana.
Introduction
The Guidelines for the Alternative Care of Children, welcomed by the UN General Assembly in 2009, encourage efforts to keep children with their families where possible (United Nations General Assembly, 2009). When this is not in the child’s best interest—or when children become separated from their families for reasons of poverty, household conflict, abuse, health issues or any of a number of possible stressors—it is the responsibility of the State to step in and provide temporary or permanent care for children deprived of a family environment (United Nations General Assembly, 1989). In such situations, the State must protect the rights of the child and ensure a range of alternative care options that promote child well-being, from family-based care such as kinship and foster care to residential care or supervised independent living. Across this spectrum of care options, preference should be given to quality family-based care arrangements when available and feasible. Recourse to institutional care should be viewed as a last resort and used as a temporary measure, with the aim of finding a stable and safe long-term placement in a family setting, including, where possible, reuniting the child with his/her family. The potential harm and risks of institutionalization to child development are well-documented (Berens and Nelson, 2015; van IJzendoorn et al., 2020), particularly for very young children who remain in such settings beyond the age of 6 months (Rutter, 1998).
Nevertheless, many countries continue to rely on institutional care in situations where family-based options are not readily available or feasible. Such is the case in Ghana where, in the absence of a formal alternative care system established by the Government, different models have emerged, notably residential care (Ghana Department of Social Welfare, 2005). This is despite the fact that, historically, the country’s social welfare system was largely communal with strong cultural values emphasizing the family unit. As such, children without parental care were viewed, even if informally, as being the responsibility of the extended family and community (Frimpong-Manso, 2014). However, with the country’s changing landscape to a more modernized society, coupled with a higher cost of living and limited economic opportunities, this traditional approach to alternative care has weakened (Frimpong-Manso, 2014; Nukunya, 2003) and residential care facilities have proliferated. Poverty has been noted as a key driver of institutionalization (Ghana Department of Social Welfare and UNICEF Ghana, 2018b), although the UN Guidelines for the Alternative Care of Children state that this should never be the only justification for placing a child into residential care (United Nations General Assembly, 1989). Rather, the Government should find ways to appropriately support families, whether monetarily or through the provision of services, that allow children to stay within their families.
In 1949, the Child Care Society, a charitable organization, established the first facility in Ghana to take care of orphans and abandoned children (Frimpong-Manso, 2014). In 1985, only three residential homes for children (RHCs) existed across the country, and all were run by the State (Messmer, 2014). By 1996, 13 such homes were operating, including 10 private facilities (Messmer, 2014). A decade later in 2006, the first national study (the Orphanage Census) conducted by the Department of Social Welfare (DSW) with Orphan Aid Africa (an international non-governmental organization) mapped 148 RHCs (Ghana Department of Social Welfare, 2005). Amid this tenfold increase in the number of homes were disturbing allegations of sexual and physical abuse, corruption, and human trafficking within several of the institutions. Additionally, the vast majority of children living in such homes were found not to be orphans but placed there because their families were poor. A subsequent national mapping conducted by DSW in 2012 again recorded 148 RHCs (UNICEF and Global Affairs Canada, 2015). These efforts yielded different counts of the number of children in institutional care from 4000 in 2006 to 4457 in 2012. In 2017, DSW and UNICEF undertook a review of the available database and identified 115 RHCs as of October 2016, housing an estimated 3586 children (Frimpong-Manso et al., 2018; Ghana Department of Social Welfare and UNICEF Ghana, 2018b). It is unclear whether these fluctuating figures reflected real changes in the size of the population of children living in institutions over the 10-year period or were rather an artifact of incomplete or inaccurate record-keeping and/or differing approaches to data collection.
This lack of an accurate and reliable baseline figure on the number of children living in residential care is not unique to Ghana. Despite the fact that, under the United Nations Convention on the Rights of the Child and most national laws, every child without parental care is the responsibility of the State, many countries do not have systems in place to gather the data necessary for monitoring the situation of children in institutional care. In fact, the 2019 United Nations General Assembly Resolution on the Rights of the Child urged States to improve data collection, information management and reporting systems related to children without parental care in order to close existing data gaps and develop global and national baselines (United Nations General Assembly, 2020). Official records often capture only a small fraction of the actual number of children in residential care, and children living in such settings are often not represented in available national statistics, which typically rely heavily on data collected through household surveys. Therefore, high-quality and robust data on these children’s status when it comes to some standardized measures of well-being in health, nutrition, education, and protection are lacking. This represents a serious data gap, hinders the ability of countries to monitor this vulnerable population of children and limits efforts to ensure no one is left behind within global monitoring frameworks such as the Sustainable Development Goals (SDGs).
To begin to address this gap, UNICEF developed a data collection protocol and tools for mapping residential care facilities, enumerating the children living in them and conducting a survey of their well-being that can be replicated and adapted in a variety of country contexts (United Nations Childrens Fund [UNICEF], 2020). The first application and testing of the methodology was carried out in Ghana in 2019. The data collection was implemented by the Ghana Statistical Service, under the guidance of a national Technical Working Group composed of representatives from relevant government departments.
The purpose of this article is to provide information on the residential care facilities that operate in Ghana in terms of their licensing status, staffing, child safeguarding, and protection policies, as well as the safety and suitability of the premises. The article also describes the demographic profiles of the children who live in such facilities and provides an overview of the care they received and their well-being. Results are discussed in light of the national standards for residential homes (Ghana Department of Social Welfare and UNICEF Ghana, 2018a), which are intended to guide the planning and provision of residential care services as well as standard operating procedures (SOPs) for the inspection and monitoring of RHCs (Ghana Department of Social Welfare, 2018). The paper concludes with a discussion of the findings with regard to the national context and policies on children in residential care in order to demonstrate how results are being used to inform care reform efforts and systems strengthening in Ghana.
Methods
Study design and sample
The national census, enumeration and survey of well-being were achieved through two phases of data collection. Phase One aimed to collect data on the number, location and basic characteristics of all residential homes for children in Ghana as well as the number and basic characteristics of all children living in these institutions. Phase Two was a follow-up survey on a representative sample of children living in RHCs to collect data on selected measures of well-being. The results presented in this paper are focused primarily on data generated in Phase One and some selected indicators collected in Phase Two that are within the scope of the intended objectives. A report with detailed results from both phases of data collection is available (Ghana Department of Social Welfare and UNICEF, 2021).
The administrative records maintained by the DSW were used as starting point to identify all RHCs in the country. In Ghana, RHCs are defined as facilities that provide alternative care in a non-family-based group setting, including shelters for emergency or temporary care, places of safety, transit centers, orphanages, children’s homes and villages and homes for children with disabilities (Ghana Department of Social Welfare, 2018). The list was reviewed, verified and updated in consultation with district social welfare officers. This exercise resulted in the identification of 146 RHCs across the country. As part of the data collection in Phase One, RHC directors were asked whether they were aware of any other homes operating in the immediate area. This approach led to the identification of two additional homes during the fieldwork that had not been among those listed in the administrative records. Therefore, a total of 148 RHCs were visited during Phase One. Of these, 139 were found to be eligible (eight had closed and one only had residents over age 18). Residents and staff in all 139 homes were successfully interviewed for a response rate of 100%.
The census frame of 139 RHCs and 3530 children generated in Phase One was used to select a sample of homes and children for Phase Two. The final frame used to draw the sample consisted of 130 eligible homes (nine were excluded as they had fewer than five children) with 3505 children. For Phase Two, a two-stage stratified sampling approach was used. Details on sample design and weighting procedures are documented elsewhere (Ghana Department of Social Welfare and UNICEF, 2021). A total of 552 children were selected for Phase Two: 128 children aged 0–4 years, 239 children aged 5–14 years, and 185 adolescents aged 15–17 years. The response rates were as follows: 92% for children under age 5, 90% for children between the ages of 5 and 14 years and 75% for adolescents aged 15–17 years. The lower response rate among this latter age group was primarily due to the fact that a number of sampled adolescents were found to no longer be eligible due to their age at the time of Phase Two data collection. The response rate among social workers (for children of all ages) was 92%.
Questionnaires/tools
During Phase One, the director or other designated official of the RHC was interviewed using four questionnaires/tools (see Table 1). Phase Two also involved the application of four questionnaires, but respondents differed across the tools. The questionnaires for children under 5 and children 5–14 years were administered to caregivers (i.e. staff of the RHC) of randomly selected children, while the Questionnaire for Adolescents 15–17 Years was directly administered to randomly selected adolescents. The Questionnaire on Children’s Case History was administered to the social worker or assigned caseworker for each randomly selected child and adolescent aged 0–17 years. In all cases, questionnaires were administered via in-person interviews.
Questionnaires/tools used in the two phases of data collection.
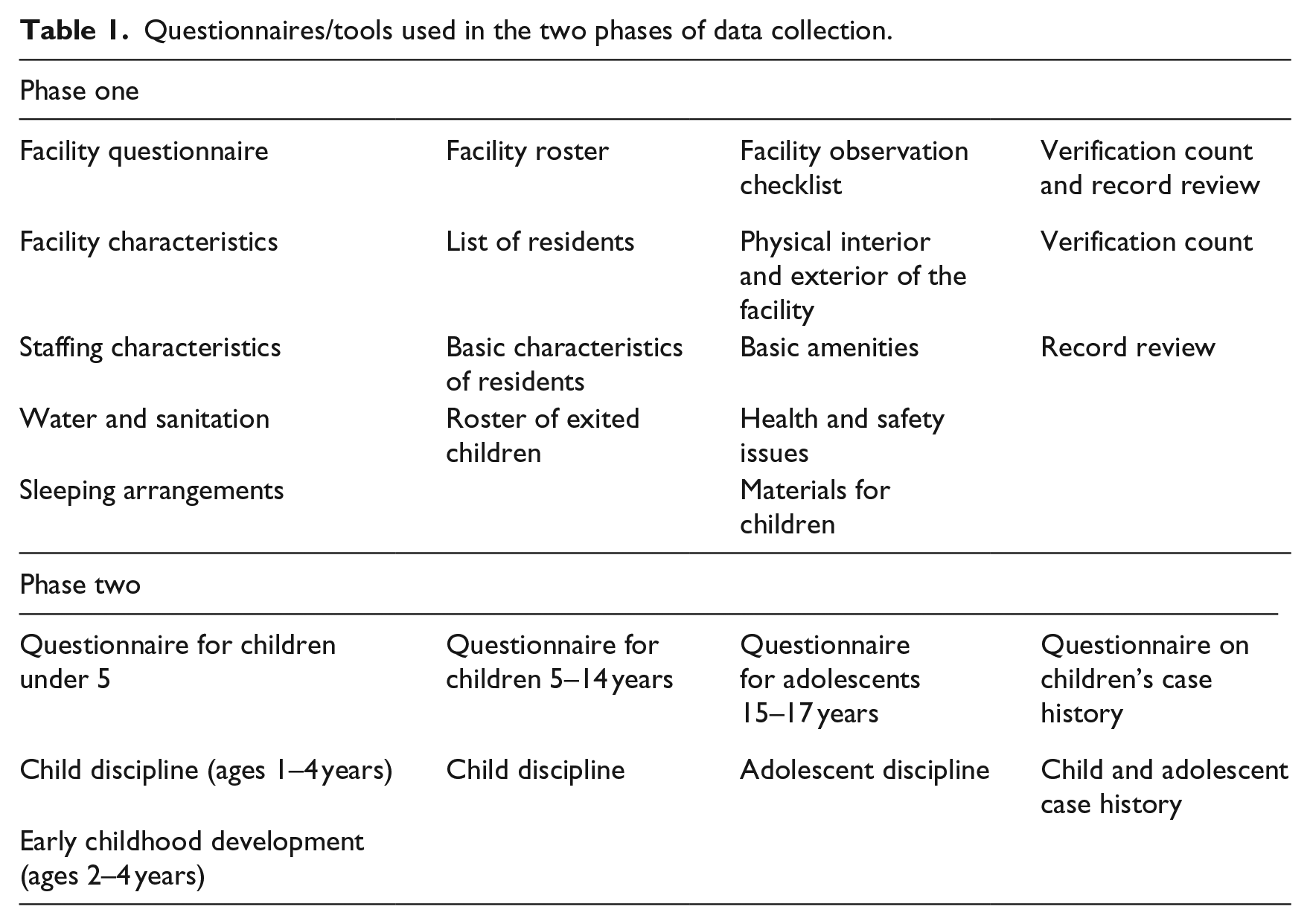
Most of the modules included in the Phase Two questionnaires were adapted from the standard questionnaires used for the sixth round of the Multiple Indicator Cluster Surveys (MICS6), which is an international household survey program that collects data on key indicators about the health and well-being of women and children. While the questionnaires covered a wide range of topics from child functioning to resilience, this paper reports on the disciplinary methods (including both violent and non-violent) used with children and adolescents aged 1–17 years in the 1 month preceding the survey, children’s exposure to early stimulation and responsive care by staff and volunteers of the RHC (among children aged 2–4 years) and children’s developmental status (for children aged 3–4 years). Information on children’s experience of disciplinary methods was provided by caregivers for children under the age of 15 and by children themselves if older. All the information related to children’s exposure to early stimulation and responsive care and children’s developmental status was obtained through caregivers.
The measure used to report on disciplinary practices is an adapted version of the Parent-Child Conflict Tactics Scale (Straus et al., 1998). To assess exposure to early stimulation and responsive care, respondents are asked whether they, or any other adult staff or volunteer in the home, has engaged with the target child in any of the following activities in the past 3 days: reading books to the child; telling stories to the child; singing songs to the child; taking the child outside the home; playing with the child; and naming, counting or drawing things with the child. Finally, developmental status was assessed using a 10-item index (the Early Childhood Development Index, or ECDI) that captures the achievement of some developmental milestones in terms of physical development, literacy-numeracy, learning and social-emotional development (Loizillon et al., 2017).
Data collection
The Ghana Statistical Service recruited members of the data collection teams from its existing pool of trained enumerators, all of whom had experience carrying out data collection for other large-scale surveys. Data were collected on tablets through the use of Computer-Assisted Personal Interviews (CAPI).
Training for Phase One fieldwork was conducted over 2 days in Winneba, Central Region in October 2019. Participants included all 48 members of the fieldwork teams (36 interviewers and 12 supervisors). This in-class training was followed by a 1-day pilot in a residential home located nearby. Training for Phase Two was conducted over 4 days, also in Winneba, in December 2019. A dedicated parallel training on anthropometry (height and weight measurements of children under age 5) was conducted as well as a 1-day hands-on standardization exercise with volunteer caregivers and children from the surrounding community. A 1-day pilot in two RHCs followed the training.
During Phase One, data were collected by 12 teams; each was comprised of three interviewers, one driver and a supervisor. Fieldwork lasted for approximately 2 weeks in November 2019. During Phase Two, the data were again collected by 12 teams, each comprised of two interviewers, one driver, one measurer, and a supervisor. Fieldwork was carried out for approximately 10 days in December 2019. Both phases of data collection included a number of fieldwork quality-control measures (see Ghana Department of Social Welfare and UNICEF, 2021).
Data analysis
Sample weights were calculated and added to the analysis files for Phase Two, and data were analyzed using the Statistical Package for Social Sciences. Confidence intervals (95%) were calculated to detect any significant differences in exposure to different disciplinary practices and aspects of early childhood development. The outcomes related to disciplinary practices were explored in relation to the facility’s licensing status, size and child-to-caregiver ratios; data on children’s exposure to early stimulation and responsive care and on children’s developmental status were examined in relation to the facility’s size and child-to-caregiver ratios.
Ethical review and protocol
The country protocol was submitted for ethical review and approved by the Ghana Health Service’s Ethics Review Committee in July 2019. For Phase One, written consent for the RHC to participate in data collection was obtained from the facility’s director or other appointed official. During Phase Two, verbal consent was obtained for individual interviews with caregivers about children under the age of 15 years. The facility’s director or other appointed official gave consent to directly interview adolescents aged 15–17 years and the adolescent respondents provided their written assent to be interviewed.
The introductory script in the Questionnaire for Adolescents 15–17 Years outlines the purpose of the data collection (in general terms) and advises respondents that some of the questions are personal and might be sensitive in nature. During the introduction, the interviewer also explains that respondents can choose not to answer any of the questions and/or stop the interview at any time. In addition, respondents are informed of the confidential and private nature of the interview and that the information provided will not impact their living situation in the facility or any decisions about placement outside of the facility. At the beginning of some of the more potentially sensitive modules, the adolescents were again reminded that their answers were private and would not be shared with anyone.
As an additional safeguarding procedure, the interviewer was required to read a short script at the end of the interview and to give the respondent a service information card. The card included phone numbers of local services (DSW and a hotline) that the respondent could contact if he or she wanted to speak with someone. These services are all free of charge and available/open 24 hours a day, 7 days a week (including holidays). Interviewers also asked respondents if they wanted to be linked directly to professional services. If the respondent expressed a desire to do so, the interviewer recorded details on the best and safest way and time to have professionals contact him or her for follow-up. Interviewers informed their supervisors when adolescent respondents requested a referral. The names and contact information of all those adolescent respondents who requested a referral were shared with the DSW to carry out the necessary follow-up. Roughly two thirds of all adolescents with completed interviews requested such referral.
Results
Residential homes for children
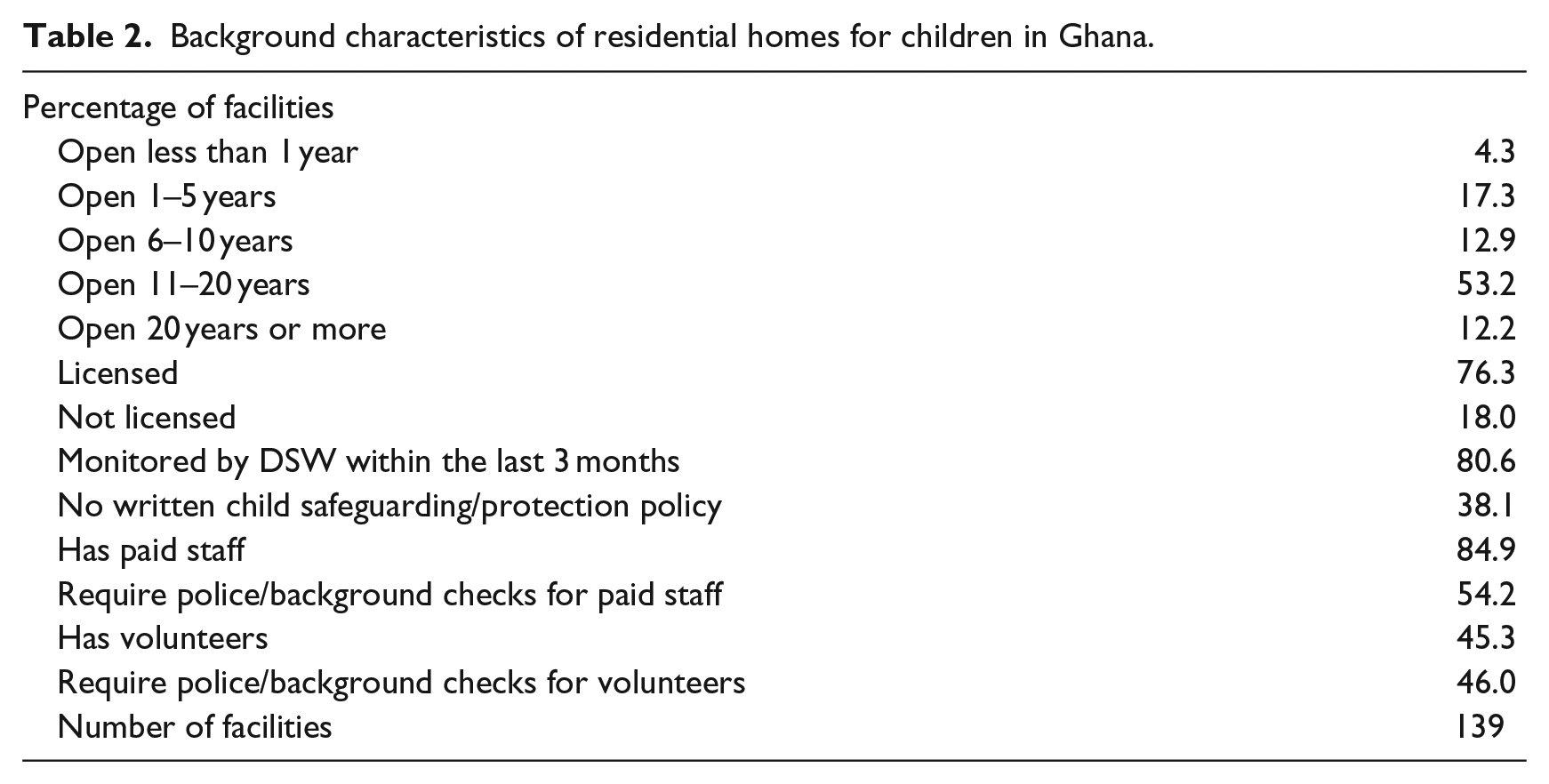
The national census carried out in Phase One identified 139 residential homes for children, the majority of which were located around the country’s capital city in the Greater Accra region. Most of the homes (78%) had been open for 6 years or more (Table 2). The others had been open for less than 6 years even though the DSW has not registered any new institutions since 2016. Two homes newly identified during the census were also clearly operating without the Department’s knowledge.
Background characteristics of residential homes for children in Ghana.
Despite the existence of a set of national standards and SOPs pertaining to residential care services in Ghana, the census revealed that many homes were not in compliance in a number of key areas.
Licensing and monitoring of residential homes
All residential homes for children must have a license with the DSW to operate as an approved residential home, and this must be renewed biennially. The census revealed that only about one third (31%) of RHCs had a valid license, 26% had a license that had expired, 19% were reported to have a license but its existence was not verified by interviewers, 18% were not licensed and 6% were missing information about the home’s licensing status.
The SOPs require that homes receive quarterly monitoring visits. While the majority of RHCs (80%) had received such monitoring by DSW within the past 3 months, around one third (35%) of these lacked documentation of this in the form of a monitoring report (which is supposed to be prepared within 2 weeks of the visit according to the SOPs).
Child safeguarding and protection
The national standards require all homes in Ghana to have a child safeguarding policy in place that includes a code of conduct and complaints procedure. However, the census revealed that slightly more than one third (38%) of homes did not have a written child safeguarding/protection policy. Moreover, of those homes with such a policy in place, only roughly one third (38%) were reported to contain both a code of conduct and a complaints procedure. The standards also stipulate that all staff and volunteers working in the home should sign the code of conduct; however, only slightly more than two thirds (69%) of those with a code of conduct said they kept signed copies on staff/volunteer files.
Staffing
Most RHCs (85%) had paid staff, while slightly less than half (45%) had volunteers. The standards stipulate that everyone working in the home needs documented clearance from the police (or two references from community members and a written self-declaration in the absence of this). However, only about half (54%) of homes reported that they conduct police/background checks on staff and 46% said this was done for volunteers. The standards are also very clear in stating that volunteers should never work as caregivers to children in the home. Despite this, around 1 in 7 RHCs (14%) were found to have only volunteers acting as the children’s caregivers.
Safety and suitability of the premises
The application of the Facility Observation Checklist was very telling and revealed that a number of conditions for ensuring the safety and suitability of the premises outlined in the standards were not being met.
Standards require all RHCs to have an accessible first aid kit on the premises, but interviewers observed that around 1 in 8 homes (13%) did not appear to have one. In Ghana, the use of mosquito nets is imperative given the existence of malaria in the country. Despite the fact that RHCs are supposed to have such nets in bedrooms and on windows, observations revealed that 29% were lacking these.
The standards stipulate that all RHCs should ensure that children have access to toys, games and play equipment as well as a selection of age-appropriate print materials such as books. Observations gathered through the checklist revealed that 3 in 4 homes (75%) had books that were accessible to the children; the remaining 25% either did not have books present or were observed to have some books but these could not easily be accessed by the children. A roughly similar proportion (73%) were observed to have toys, games, and/or play equipment that was in good condition available for the children’s use.
A few homes were observed to have some serious safety concerns. This included three homes that had sharp objects/implements/tools within children’s reach; nine homes where medication, alcohol, drugs, or detergents were left in reach of children; and three homes where children were observed to be locked in rooms or tied up.
Profile of children living in residential care
A total of 3530 children were found to be living in residential homes in Ghana (57% boys and 43% girls). This was considerably less than the roughly 4000 listed in the original administrative records maintained by DSW. Conducting the enumeration of children revealed that a primary reason for this discrepancy was that many residents in RHCs were actually over the age of 18 years and therefore not in fact children anymore.
The survey revealed that around two in three children living in residential care have at least one living biological parent (27% have both biological parents living and 36% have one biological parent alive). Despite living in an RHC, 60% of children still have contact (either in-person or over the phone, emails/letters etc.) with parents or some other relatives and around half (52%) have family living in the same region as the residential home.
Disciplinary practices
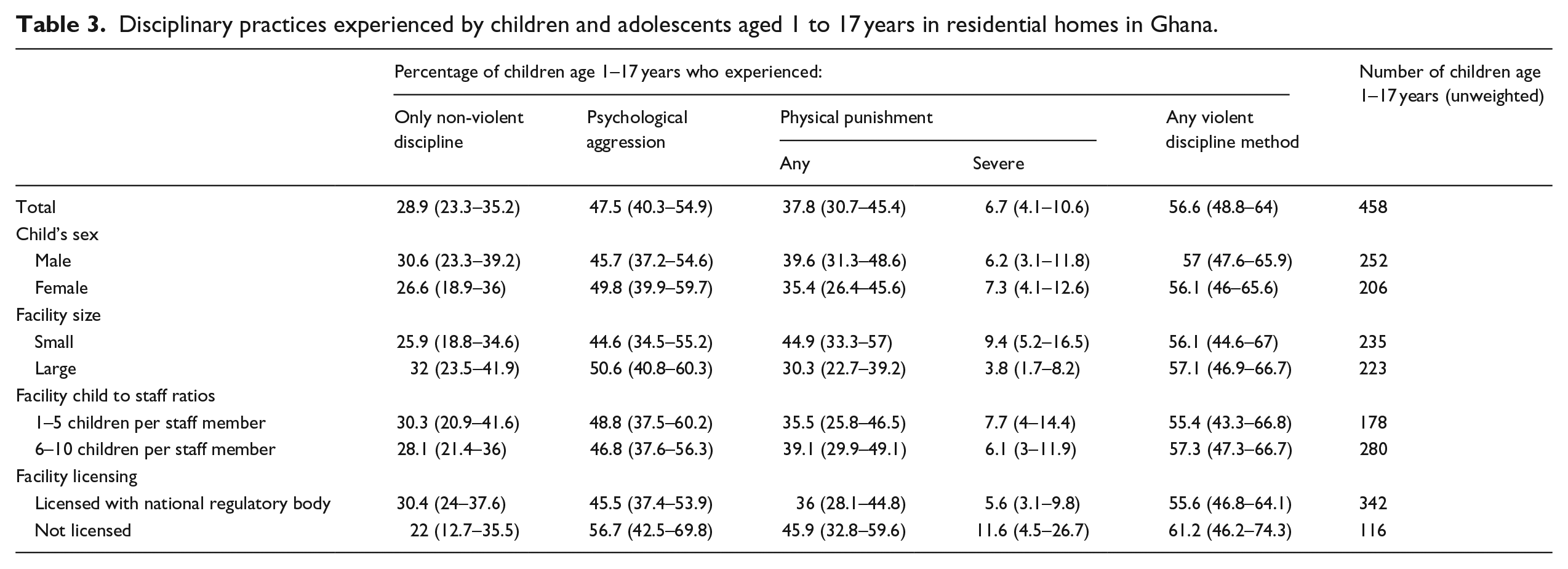
As shown in Table 3, 57% percent of children aged 1–17 years’ experience violent discipline (physical punishment or psychological aggression). Children in licensed RHCs were equally likely to be exposed to forms of violent discipline as those children living in unlicensed homes (56% and 61%, respectively). However, a higher proportion of children in licensed homes (30%) reportedly experienced non-violent forms of discipline exclusively (which includes having privileges taken away, explaining why a behavior is wrong or being given something else to do) than those in unlicensed homes (22%). This difference was not significant, however. Children in large RHCs (with 30 or more children) were equally likely to be exposed to forms of violent discipline as those children living in small homes with less than 30 children (57% and 56%, respectively).
Disciplinary practices experienced by children and adolescents aged 1 to 17 years in residential homes in Ghana.
Child development
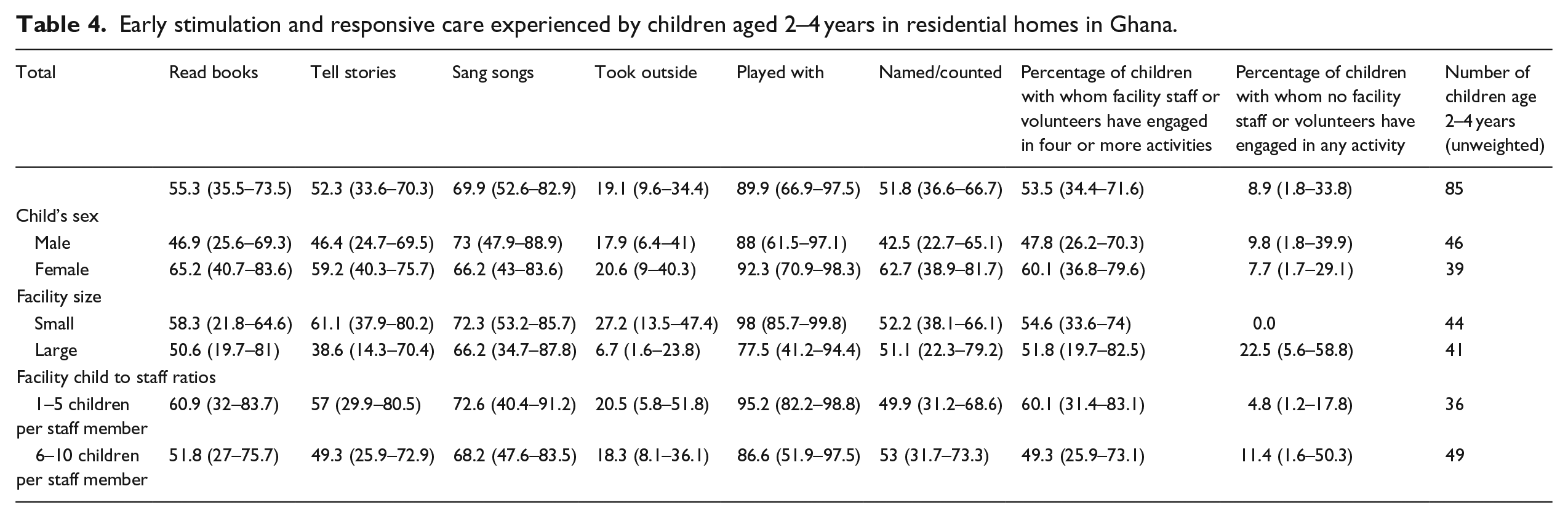
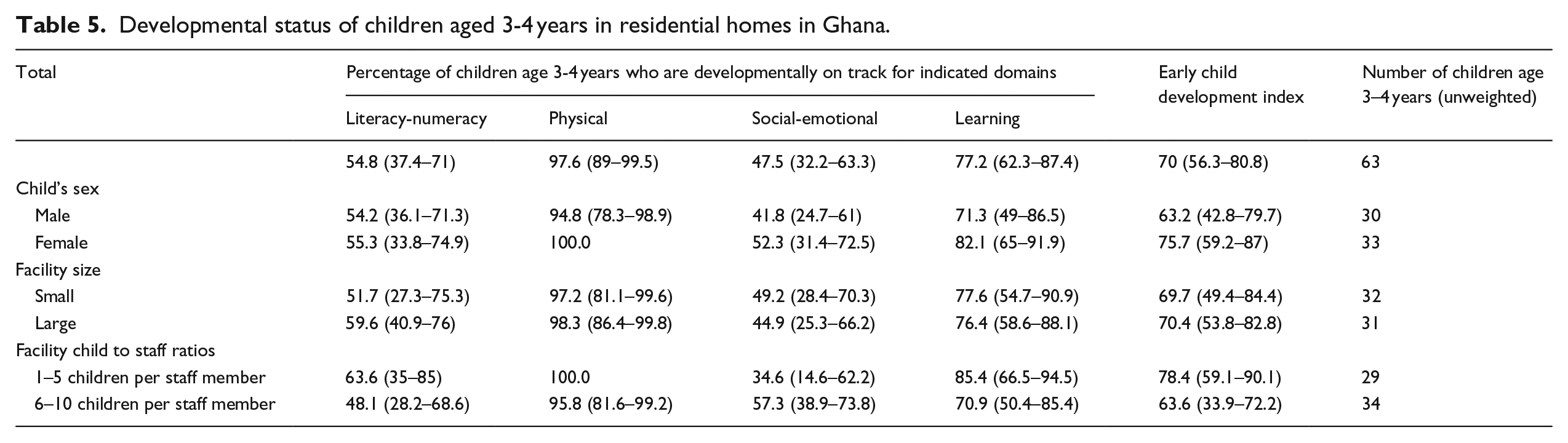
Results on some indicators of early childhood development are presented in Tables 4 and 5. Children aged 2–4 years in large homes were equally likely to be engaged in four or more activities for early stimulation and responsive care as those in small homes (52% and 55%, respectively). Larger differences in the percentages of children who received stimulation and responsive care were found depending on child-to-caregiver ratios (60% vs 49% in homes with a child-to-caregiver ratio of 1–5 children per caregiver vs 6–10), but this difference was not significant. The same proportion of children aged 3–4 years were classified as developmentally on-track in at least three of the four domains (physical, literacy-numeracy, learning, social-emotional) in large and small homes (70%). However, in homes with a child-to-caregiver ratio of 1–5 children per caregiver, such proportion is higher, that is, 78% vs 64% in homes with a child-to-caregiver ratio of 6–10 children per caregiver, although the difference is not significant. Child development outcomes by licensing status could not be reported due to small cell sizes.
Early stimulation and responsive care experienced by children aged 2–4 years in residential homes in Ghana.
Developmental status of children aged 3-4 years in residential homes in Ghana.
Case management
Practically all homes (97%) were in compliance with the requirement that all children have an individual case file. That said, only 69% of homes were found to be in compliance with storing such files in a secure location.
The standards require that all children remaining in RHCs for more than 7 days have a care order. The survey revealed that the vast majority (89%) of children living in the homes had been there for 6 months or longer but only around two thirds (64%) had been placed in the facility as a result of a care order.
All children in RHCs are supposed to have an individual care plan, but the survey found that about one third (36%) did not have such plan in place. The standards stipulate that these care plans should include a permanency plan for either reintegrating children into their families or placing them in some other alternative arrangement such as foster care. However, the survey found that among children with a care plan, around 1 in 8 (12%) did not include permanency planning.
Just over half (56%) of children were reported to have an assigned caseworker from the DSW.
Discussion
To inform the programs and policies regarding children in alternative care, reliable estimates of the numbers of children living in such settings are essential. For this reason, the DSW and its partners embarked on a nationwide mapping and census of RHCs, as one type of alternative care, and the children living in them as well as a survey of their well-being. The exercise was not exempt from some limitations. The cross-sectional nature of the data implies that the results reflect the state and condition of residential care in Ghana at the time of data collection. Additionally, an attempt was made to collect data on a wide range of issues and topics relevant to child well-being, but there were some constraints on what could reasonably and feasibly be captured within a survey of this nature. As a result, the available data do not capture the full experience of children living in residential care nor do they shed light on the long-term effects that institutionalization can have on children’s future health and well-being. It is difficult to know whether the high number of referrals requested by the adolescent respondents was due to the potentially upsetting nature of the interview itself or whether adolescents saw this as an opportunity to request some support and assistance with their situation more generally. In either case, it is clear that the inclusion of additional safeguarding procedures may be warranted and that many adolescents living in residential care do not feel adequately supported.
There was no way to independently verify the extent to which staff provided honest and accurate responses, particularly when it comes to reporting about child well-being. However, the assumption that respondents are being truthful is not unique to this survey. Also, the fact that all eligible RHCs agreed to participate could reflect the fact that the DSW had sent letters to notify them of the planned data collection and, while not the intention, this may have been interpreted as a request that could not be denied. Finally, despite the fact that efforts were made to ensure that all institutions were identified as part of the mapping, it is still possible that some, particularly those that are unregistered or informal, may have been missed.
That said, the census and survey have a number of important strengths and represent a milestone in efforts to generate high-quality and reliable evidence on residential care in Ghana for better policy, planning, and monitoring. The exercise differs from previous efforts in that it did not rely exclusively on available records but rather made an attempt to identify all RHCs, including unregistered ones, by employing key informants and to verify the accuracy of existing records through a visual verification count of children. It was also considerably more comprehensive than past mappings in terms of its scope. Such data will help the Government to track progress in implementing the Care Reform Initiative and plan how best to accelerate the process. The survey was also an opportunity to reconcile discrepancies in figures reported by different government ministries and agencies over the years that contradicted one another.
Beyond providing baseline data for planning, findings from the census and survey have enhanced understanding of the situation of residential care facilities in the country and the children living in them. This should help critically review strategies and interventions and enable stakeholders to redirect—and redouble—efforts to achieve positive outcomes for children. In that regard, the survey has shed light on some of the aspects of the current system that are not functioning well and indeed are quite concerning and raise the question of accountability. For example, despite the policy reforms, regulations and gatekeeping mechanisms in place, the finding that about 1 in 5 homes had been open for less than 6 years despite the DSW not having registered any new institutions since 2016 suggests that these homes are operating without having followed the necessary requirements for registration and licensing. Moreover, despite the amended Children’s Act, 1998 (Act 560), the Child Rights Regulations, 2003 (legal instrument no. 1705) and the 2018 national standards, which require all RHCs to be licensed, only one third were found to be operating with a valid license.
Findings that revealed some of the unacceptable conditions and protection issues facing children living in residential care point to the need for social welfare staff working with decentralized district administration to deliver better on their statutory obligation to conduct regular inspections and monitoring visits of facilities.
Despite the existence of gatekeeping mechanisms in the country, the survey revealed that many children have been admitted to RHCs without the involvement of social welfare officers or the court, meaning that these children were taken into the homes illegally. Therefore, district social welfare officers need to play a more active role in the case management of children in institutional care, participating in the development of care plans and ensuring that these encompass reintegration and/or a permanent family placement. The finding that only half of the children in RHCs have an assigned caseworker from the DSW while about one third are without an individual care plan is distressing; it also undermines the possibility of these children being permanently placed in a family-based care alternative. Additionally, without such supports in place, it will be difficult to ensure that the best interests of each individual child living in residential care is being duly considered.
The results on the impact of licensing status, size and child-to-caregiver ratios suggest that the quality of care (in terms of early stimulation and responsive care and use of violent discipline methods) does not appear to differ significantly or have a noticeable impact on developmental outcomes for young children depending on these structural qualities of RHCs in Ghana. This despite that fact that licensed homes are required, in principle, to provide a certain level of quality of care as outlined in the national standards in order to be licensed in the first place.
Conclusion
Ghana has been on a path to reform its alternative care since 2007 when the DSW, in collaboration with UNICEF Ghana, OrphanAid Africa and other donors, embarked on an initiative to reduce reliance on institutional care and move toward a range of integrated family and community-based care services (Frimpong-Manso, 2014). Through its Care Reform Initiative, new standards for institutional care were developed in 2010 and revised in 2018 (Ghana Department of Social Welfare and UNICEF Ghana, 2018a), and regional multi-agency teams were set up to inspect RHCs (Ghana Department of Social Welfare, 2018). In 2017, all 10 regions developed a 5-year road map to close substandard homes. The intention was not to close down all the RHCs but rather to ensure that, for children for whom family or kinship care is not an option, a continuum of quality temporary, long-term and permanent alternative care options is available—including family-based alternative care options such as foster care and adoption and, as a last resort, residential care. The Department has also recently developed “Deinstitutionalization Guidelines” (Ghana Department of Social Welfare and UNICEF Ghana, 2020).
While much has been done to advance care reform, the results of the census and survey highlight the need to further improve— and invest in— Ghana’s case management system to track children in need of care and protection in general, and in residential care in particular. Following completion of the survey, a series of policy documents on children in alternative care were developed and the Ministry of Gender, Children and Social Protection and its partners have implemented a digital Social Welfare Information Management System (SWIMS) using the Primero software package designed by UNICEF. The system is a case management tool to help social welfare officers and caseworkers, including those working in residential homes, better manage child protection cases, including children without parental care, and generate routine data on their situations. According to the Ministry, the system is now operational in 60 districts (out of 260). Even though it will likely take several years before the system is capable of generating real-time data at the national level, it is a step in the right direction and will replace the need to conduct large-scale (and expensive) surveys. Most importantly, it should equip the district social workers and staff of RHCs with the tools to provide better quality services and to ensure children’s best interests are upheld.
Footnotes
Acknowledgements
The authors thank Ivana Bjelic and Munkhbadar Jugder for their support with data processing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The survey was made possible through a grant from the United States Agency for International Development (USAID) and UNICEF core resources.