
Abstract
This article aims to elevate children’s and caretakers’ voices in shaping reunification and reintegration planning and implementation. It takes into consideration, the priority for children to experience fulfilling and happy childhoods following reunification from residential care facilities (RCFs) to homebased care (HBC). The article is based on 23 children who were followed up, 12 months post reunification from RCFs into HBC in six districts within central Uganda, a region with the highest concentration of RCFs. We conducted 11 in-depth interviews with older children aged 8–13 years and 23 in-depth interviews from the caregivers, who also provided information on 12 children who on account of age (less than 8 years) could not be interviewed. The qualitative study was nested under a longitudinal study (Randomised Controlled Trial NCT03498469). This study has revealed positive experiences following re-unification of children with homebased caregivers such as; continuous and positive child-caregiver interactions which translated into trusting and loving relationships and bonding between children and caregivers; improved parenting practices characterised by warmth and responsiveness to children’s physical, emotional and material needs and less reliance on harsh disciplinary practices; and social reintegration exemplified by children forging positive relationships with family and community members and their active participation in ongoing social activities. Yet the voices that perceived reunification negatively point to the overarching need to prioritise household welfare through economic strengthening efforts and other forms of provisioning and more crucially, ensuring children’s continued access to quality education as key ingredients in planning and implementing successful child reintegration efforts, including assuring children of happy and fulfilling childhoods.
Introduction
Social service professionals working to reunify children with their parents predominantly rely on facts that hardly describe children’s experiences of growing up in a home setting or a setting away from home and in particular, growing up in a residential care facility (RCF). The accounts often do not bring out children’s lived experiences in the context of reunification and reintegration and what this portends to planning and implementing effective reintegration efforts. This paper aims to fill this gap and also bring out the concerns of caregivers of looking after children following a period of separation.
Research from the global north attributes far greater benefits to children being raised in a home setting under the care of parents or kinship members compared to being raised in an RCF. These include, forming and maintaining long-term meaningful relationships (Bowlby, 1969) and positive physical, cognitive and emotional development outcomes (Browne, 2009; van IJzendoorn et al., 2020). As such, efforts globally (see United Nations Convention on the Rights of the Child, 1989, articles, 3, 7, 8 and 39 and the UN Guidelines on Alternative Care of Children, 2010) prioritise children growing up in a family of their birth. Separated children and in this case, those living in RCFs, are recommended for reunification with their parents – a one-time event and subsequent reintegration, which itself is a multi-dimensional step-by-step process that evolves overtime (Wedge, 2013). Here children are expected to fit well within their families and communities and live fulfilling childhoods. While this is the ultimate goal, less priority is often placed on learning from the affected children in the context of transition and reintegration into homebased care (HBC) so as to plan child-centred and sustainable reintegration efforts.
Careful consideration should be paid to Uganda and low-income countries where children are separated mainly due to death of parents, conditions of destitution in homes, desire to access education and fleeing abuse and neglect in families (de Sam Lazaro, 2019; Font et al., 2018; Walakira et al., 2014a). While a great deal of effort is placed on reunifying and reintegrating such children, it is not clear what form of supports are critically needed to make the process more effective. It is also not clear what policy and programming implications this would present for building fulfilling childhoods for the reunified children. This notwithstanding, the Uganda government has pursued a policy of de-institutionalisation of children after it formulated an Alternative Care Framework in 2012 (Ministry of Gender Labour and Social Development [MGLSD], 2012a) in compliance with the UN Alternative Care Guidelines. With support from development partners, gate keeping processes for RCFs have been strengthened (see GOU Approved Home Rules (GOU, 2013) and the Children Amendment Act (GOU, 2016)). Targeted capacity building for improving care practices and case management and documentation has also been undertaken among others. Yet despite these efforts, an estimated 50,000 children are still under the care of RCFs, many of which are not legally registered, pointing to the need for sustained efforts in reforming care practices (MGLSD, 2012b).
Children in RCFs are considered to be separated. However, many maintain contact through visitations to RCFs and spending school holidays with their families (Walakira et al., 2014a). The consideration that children in RCFs suffer developmental deficits has been well articulated (Browne, 2009; Carter, 2005; van IJzendoorn et al., 2011). Yet developmental deficits are also documented among children growing up in families on account of multiple deprivations (UNICEF and Uganda Bureau of Statistics, 2019) symbolised by malnutrition, ill health, abuse and neglect, poor academic performance and school dropout. Thus, where reunification from RCFs is undertaken without careful consideration of those concerns, it would still affect children’s experience of healthy childhoods where their rights would not be protected.
If then actors are to consider pursuing effective reintegration, what critical issues should they consider? Parenting is singled out as a key intervention area to address risk factors to family separation such as violence against children which is linked to poor mental health (Shonkoff et al., 2012; Taylor, 2010), disruptive behaviour (Boden et al., 2007), poor attachment (Suzuki and Tomoda, 2015) and poor academic performance (Devries et al., 2014). Thus, inclusion of parenting education and training would limit these risk factors and contribute towards successful children’s reintegration with their families. Alongside parenting is case management (CM) which involves decision-making, coordination and provision of services (LeVine and Sallee, 1999). CM requires that sequential steps are undertaken in planning and implementing reunification including provision of services. One of the steps involves carefully assessing children’s psychological, emotional and physical readiness for reunification. This in essence entails professional communication and interaction with children and respecting their views in relation to decisions being made for reunification. In so doing, children would not merely be passive recipients of re-integration decisions and actions, but active agents who shape the direction in planning and implementation of reunification and reintegration efforts. Other steps include but are not limited to carefully tracing and assessment of families for reunification, developing a reintegration plan and its implementation and case closure as deemed necessary. Drawing a clear line between a parenting intervention and case management processes though, is not very clear during post reunification support. Another critical support identified is economic strengthening for households. It may not be very clear though as to what form of economic strengthening (ES) is most effective given the wide variety of ES services. These include cash transfers, supporting income generating schemes, microfinance services, business and vocational skills training and agricultural support interventions (see Child Protection in Crisis Network [CPC], 2011). ES is associated with improved food intake, expansion of assets, increased income and access to education by children (Behrman et al., 2012; Mushunje and Mafico, 2010; Thurman et al., 2015) and improved nutrition and life expectancy (Aizer et al., 2016).
This paper aims to assess children’s lives and their experiences of transitioning from RCFs to HBC after a period of separation. The paper further draws on the experiences of caregivers to provide a context for planning and implementing effective reintegration efforts that enable children to have fulfilling childhoods in resource constrained settings. The paper examines the experiences of children and caregivers in light of parenting support, case-management and cash transfer given to children and their families during and post reunification.
Methodology
Study design
This study utilises qualitative data collected as part of a longitudinal randomised controlled trial study (NCT03498469) that had been designed to measure the effectiveness of parenting education on the successful re-integration of children aged 1–13 years. A few descriptive statistics have been included in this paper to provide further understanding on the situation of children prior to placement in RCFs. Data for this qualitative study was collected at time point 3 (T3), 12 months post re-unification in December 2017 and June 2019.
Study population, study area and sampling
A total of 77 children and 77 caregivers were recruited and reunified as part of the RCT (USAID Cooperative Agreement AID-OAA-A-14-00061) in nine districts (Bukomansimbi, Mpigi, Masaka, Mukono, Rakai, Ssembabule, Kyotera, Kalungu and Lwengo) within central Uganda, a region with the highest concentration of children living in RCFs. Under this qualitative study, we followed up 23 children aged 3–13 years and 23 caregivers who had completed 12 months post reunification from six of the nine districts namely, Lwengo, Mukono, Mpigi, Masaka, Rakai and Ssembabule. Only four children and four caregivers were from the control group. In the presentation of findings, we have not made any distinction between participants in the control group (those that received only cash transfer of USD 125 Ugx: 469,925 and Case Management) and those within the intervention group who in addition to the above services, they received a parenting intervention.
Profiles of study participants
Out of the 23 children followed up, we conducted interviews with 11 who were old enough (8–13 years; three females and eight males) with data on the remaining 12 collected from their caregivers. All the 23 children were attending school except one, a 9-year old girl, who had developed a mental complication. Eleven of the children were reunified with their biological parents while 12 were reunified with kinship members – mainly grandparents. Out of the 23 caregivers interviewed, four were males and 19 females, all living in rural areas. On average, each household of the reunified children had 9 members, of which 5.5 were children below 18 years. Majority of the household heads (12) depended on farming with some selling part of the harvest to earn an income. Others survived on income from casual labour (3), salaried jobs (1), carpentry (1), small scale businesses (4) and handouts (1).
Data collection
Data was collected through in-depth interviews conducted in Luganda, the local language spoken, with children (11; 8–13 years) and 23 caregivers found within their homes and by use of separate tools. Careful attention was paid to protection of children and adults and ensuring issues of confidentiality. Interviewers used note books and recorders during interviews. Descriptive statistical data (which we generally consider under the qualitative component) is derived from 44 children aged 8 to 13 years and 77 caregivers who responded to two separate questions incorporated into the quantitative tools at data collection point T3.
Data analysis
Transcripts and notes from interviews were imported into NVivo 10, a flexible qualitative data analysis software package. This was used to manage coding, following a systematic and inductive procedure. We coded the interview transcripts using the constant comparison method which ensures themes are consistently classified. It also allows for the expansion or refinement of existing codes based on the objectives of the study. We stratified data by children and caregivers’ profiles where applicable, making it possible to construct categories from salient issues emerging from children and caregivers with unique situations. Using the constant comparative method, we identified incidents, participants and categories underlining divergences and similarities in perspectives. We have included verbatim quotations to provide an illustration of situations and provide narratives that enhance the voices of children and caregivers. Statistical data was analysed using the statistical package for social sciences and presented in simple descriptive tables for illustration purposes.
Data management
Data collection included audio recordings and notes. Audio files were copied to access-protected laptops at the end of each data collection day. Audio files and notes were transcribed using English language and transferred on access protected-laptops. Handwritten notes were kept in locked file cabinets. All data were declassified with personal identifiers removed. After completion of data collection, qualitative data was stored, managed or destroyed according to Institutional Review Board (IRB) approval requirements (UNCST SS 4551 and MUREC REC 0503-2017).
Findings
Children’s entry into residential care facilities
We felt it was important to first understand the circumstances that led children to enter residential care facilities, before we embark on the discussion of their experiences. From the descriptive statistics, children mentioned schooling and ‘don’t know’ as the dominant reason for their placement while parents mentioned lack of money and schooling (see Figure 1). From qualitative interviews, caregivers explained circumstances for taking children into residential care facilities, citing child abandonment.
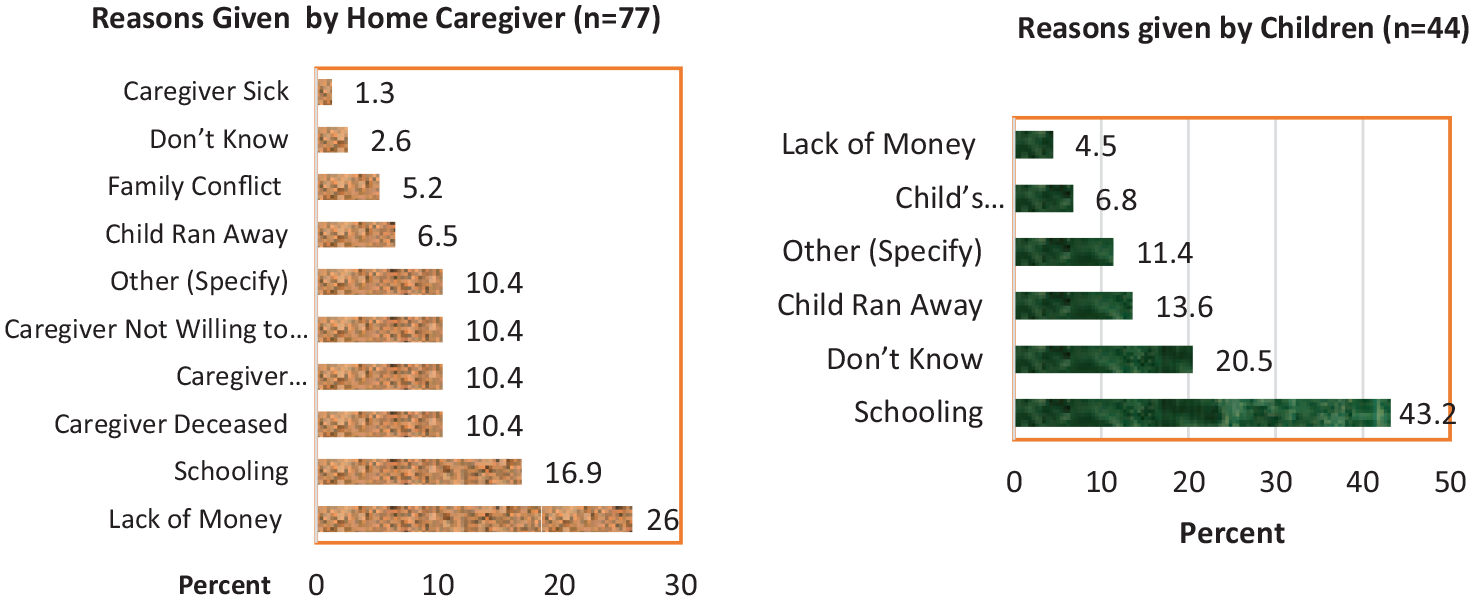
Reasons tabulated for entry into residential care institutions.
It all began when his mother and father abandoned him. By that time, I was living with my mother here at home. I couldn’t really take care of him because I had to take care of my mother and also take care of my home – Female caregiver, Masaka.
Some RCFs however source children from the communities by looking out for vulnerable families that would consider RCFs relieving them of the burden of care.
[My wife] . . . was not patient enough to raise the children. . . yet I had left for work in Tanzania. So, when the organization came in search of vulnerable children, they took him . . . Male caregiver, Masaka
Many parents find it attractive when RCFs offer children opportunities to access education. Although at times it starts with day schooling, eventually children are enrolled for full residential care to continue accessing education as revealed by parents.
Children used to go to that school next to the born-again church while commuting from home. The pastor later transferred the school to his home after he got sponsors . . . It was after then that they took our children but it was done after letting us know that the children had sponsors and [that] they had to start staying in boarding school. So, the children started like that to live at the institution and there was no problem – Female caregiver, Mpigi
The opportunity for the child to access support including education, food and clothing among others compelled caregivers to take children to RCFs as one caregiver revealed below.
He had no help and support. The child is an orphan, he needed help. So, they told us of a bursary where we do not pay fees or buy anything for the child. This was going to be up to university or until the child would get tired – Female caregiver, Mpigi.
From the above it is evident that taking a child to an RCF would relieve parents of the care burden.
Caregiver’s perception of re-integration experience
Caregivers were largely happy to receive back their children. Some got overwhelmed with positive emotions when they got the information concerning reunification. One caregiver started to think of the good moments this would bring about.
. . . After receiving that phone call, I was filled with joy . . . even before seeing my son. I became anxious . . . [together] with my wife who I am currently [staying] with. We were. . . [eager] . . . to see him. . . . [eventually when he came] I . . . [now] have the joy of all my children being together staying with me. I got so many good things from that. There is nothing as good as one living with their children. – Male caregiver, Masaka.
Interviews with caregivers reveal continuous parent-child interactions on a wide spectrum of issues including how the child is feeling, their needs and feelings towards other family members. Caregivers reported that this has led to the development of stronger emotional and social attachments. One caregiver pointed out that children freely talk to them and also mingle with their peers and enjoy their stay at home.
He tells me whenever he is not happy with me other than fearing. I managed to bring him closer by being free with him. I try to bring him closer by showing him that I am not only his mother but also a friend. He really enjoys being my friend because there are times he comes and sits on my laps and he tells me how he is hungry or how he needs something from me because he doesn’t fear me. – Female caregiver, Masaka.
Some caregivers pointed out changes in children’s academic performance. One caregiver attributed this to parental active involvement in supporting children’s learning.
Their academic performance was [poor] . . . they used to study just that no one used to care about assessing their performance. . . . At the RCF they used to study just for the sake but now something has changed about their education. . . . This has made me very happy. – Female caregiver, Masaka.
Caregivers further revealed that children have been able to learn and relearn different societal expectations. They are able to greet, practice good table etiquettes, use culturally and age-appropriate words and actions followed with culturally appropriate gestures.
Their [social behaviors] were not good because when they woke up, they never used to greet me. But now you can see that returning [home] has helped them a lot. It has also helped me a lot to deeply understand my children, how they behave, which habits they have and things like that. – Female caregiver, Masaka. When she returned [home] she . . . learnt how to say thank you . . . especially after eating food. When she is greeting old people, she kneels down. – Male caregiver, Masaka.
Some caregivers however observed that the children had developed errant behaviours which they found challenging to manage.
His siblings come and tell me, ‘You told all of us to wash clothes, but he refused’. Personally, I do not wash children’s clothes. They wash for themselves. That is a kind of defiance I cannot make him outgrow. I simply say to myself, “they refused me to beat you, so if you get tired, you will come and wash the clothes”. [Long silence] Only that defiance that I cannot make him outgrow. Can you make a child outgrow defiance? Even you, you cannot. So, one just has to wait for him to return and do what he has to. – Female caregiver, Mpigi.
Other caregivers felt that reunification had robbed their children of the opportunity of receiving support to continue with school. They looked forward to the day they would take back children to RCFs.
What kind of positivity? Do you want me to say that I am very excited because they brought him back and also [gave me] money? It is the same, he would still come back at home. I have nothing . . . [positive] to say. I wanted him to stay there. I won’t lie to you because there are even examples of other children that they helped till university level and in the end, they got good jobs – Female caregiver, Mpigi.
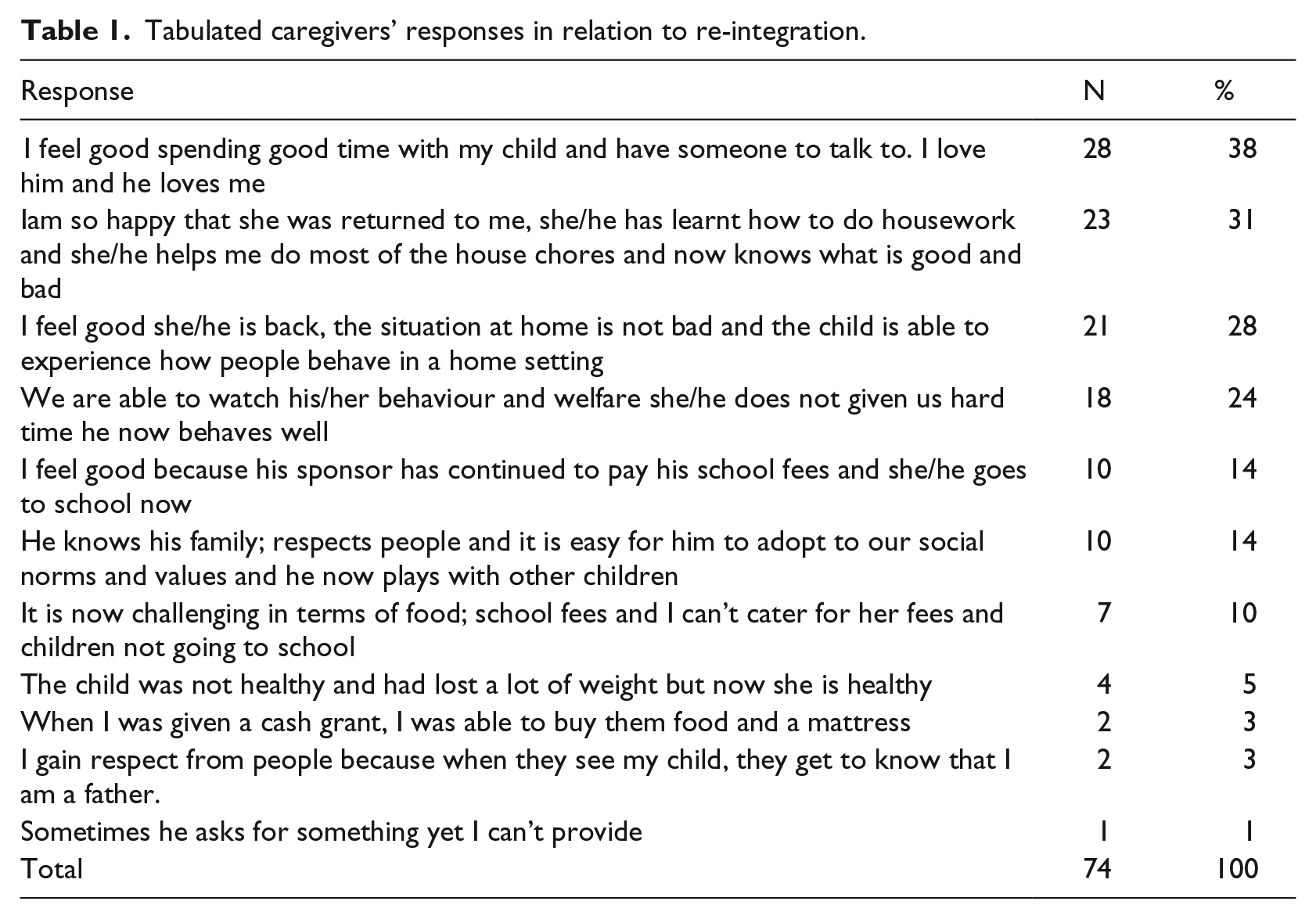
The responses of caregivers were tabulated from the quantitative tool as seen below when asked how they felt about being reunited with the child and how the experience has been. (See Table 1).
Tabulated caregivers’ responses in relation to re-integration.
Children’s response to the question on their experience of reintegration.
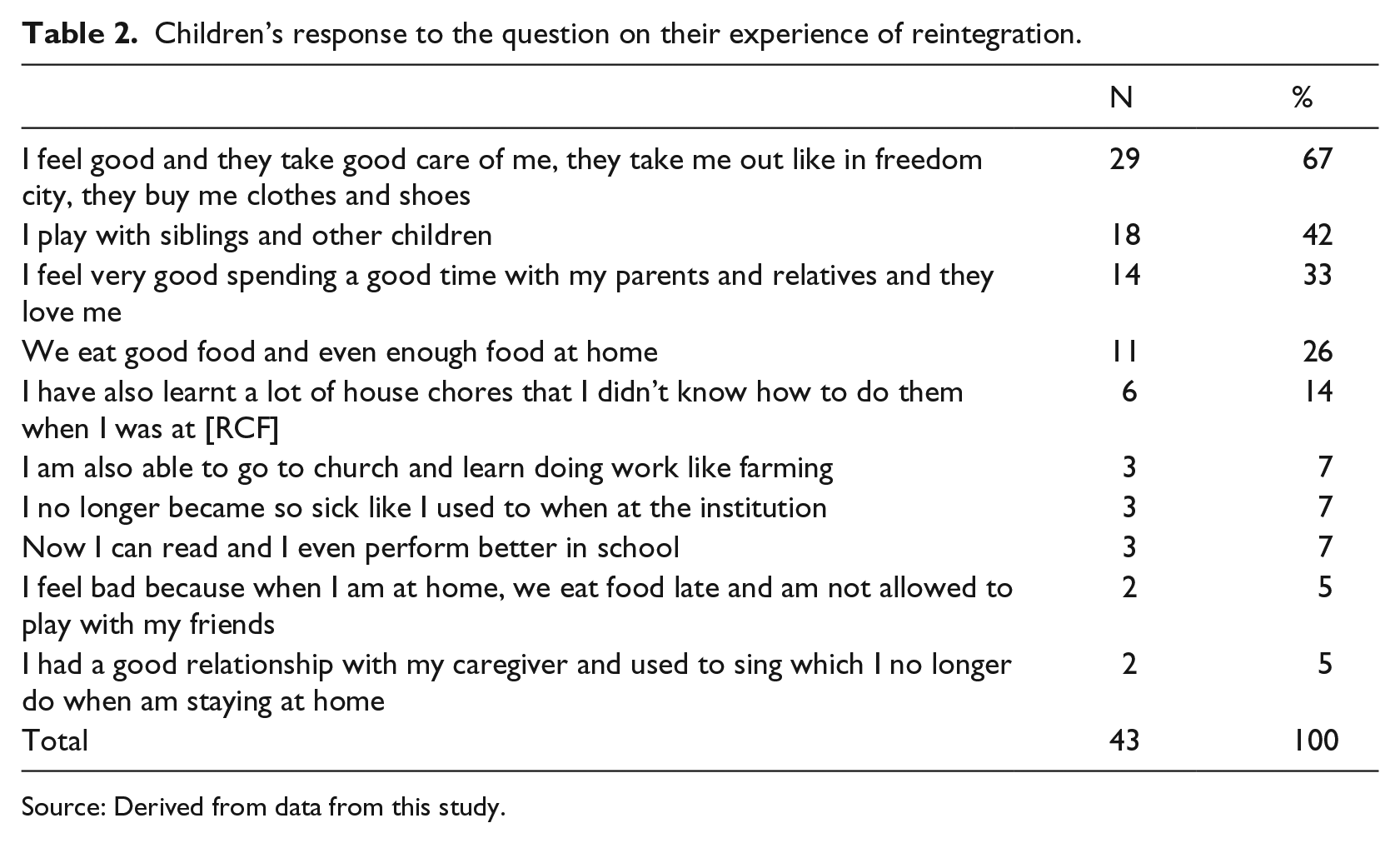
Source: Derived from data from this study.
Over all, parents expressed a positive experience of receiving back children ranging from feeling good, being extremely happy and pointing out the benefits of being with their children including having an opportunity to mentor them in the right way regarding social behavioural expectations, social norms and imparting livelihood and other life skills into their children.
Children’s experience of family-based care
Some children felt there was a difference between the training they received at home compared to the one they received at RCFs pointing out that the training at home was rigorous and accompanied with disciplinary practices.
At home mum wants us to be disciplined. She wants us to be hygienic, something that was not emphasized RCF. Flies used to be in our breakfast tea cups and we would be at a very high risk of getting diseases like cholera. . . . However, here at home sometimes mum canes us but not too much when you annoy her or behave in an inappropriate way. – Girl Child, 11 years, Mpigi.
Many children indicated that they had developed loving, caring and trusting relationships involving open communication with homebased caregivers following reunification.
The relationship . . . is very good because my mother loves me so much, she cares about me, and she even buys me clothes whenever she gets money – Girl Child, 12 years, Lwengo. I tell mum my secrets because she looks after us very well for example when I get a wound, she takes me to hospital and they give me treatment. Even when am worried about anything I usually tell my mother – Girl child, 11 years, Mpigi.
The positive relationships were not limited to caregivers, but extended to children at home and to peers within the community, a sign of social reintegration.
I do have a good relationship with the children at the neighborhood as we do relate and interact very well. We play together especially on weekends and holidays we play football. We fetch water together and I also at times stay at their homes in case my mother has gone somewhere for a while because she doesn’t allow me to stay at home alone. By the way, I also go to the same school with some of these children so we go and come back together. When I don’t have eats, they give me and if they also don’t have, I do give them. – Boy child, 11 years, Mpigi.
As part of learning to take responsibility, children appreciated their involvement in household work and also felt it was helping them to acquire life skills.
At school [RCF] they used not to teach us how to do housework at all yet girls are supposed to know how to work even do ‘technical’ work like making small craft bags and mats. But here at home mum and my grandmother teach us these things of weaving mats. It is so unfortunate that she’s now so sick but we have learnt so much from her and we are going to carry on the skills to continue making mats for sale and get our school requirements – Girl child, 11 years, Mpigi -CG. I feel good when am doing the house work because I do not over work, generally I feel free and comfortable – Boy Child, 11 years, Mpigi.
Children were positive about disciplinary practices their caretakers opted for since returning home. Without ruling out the use of harsh discipline, they explained that parents often first applied positive techniques, opting for harsh techniques as a last resort. This approach, in children’s view, allowed them to reflect and positively change one’s behaviour.
I like the way my father disciplines me because he just talks to me, advices me in case I have done anything. He shows me what’s good and bad – Boy child, 12 years, Mpigi. They ignore us on the 1st day [and] 2nd day, then on the third day, we are beaten in case we do something wrong. I like it because they give us some grace period to correct ourselves and stop whatever wrong activity we are engaged in – Boy child, 13 years, Mukono.
Some children however, did not live peacefully within their homes citing lack of cooperation, conflict, unfair and discriminative treatment.
At home we don’t cooperate. At home even when my siblings are playing, I don’t join them – Boy child, 12 years, Mpigi.
A few others felt that their welfare had severely deteriorated owing to material deprivations and the perceived risk of dropping out of school.
At home they cook very little food that is not enough for us. As for food mostly, I like rice and matooke but the food that is available at home is cassava and sweet potatoes. That is the food we get most at home – Boy Child, 12 years, Mpigi. . . . Me I always do not settle in class. They keep sending me back home for school fees. This makes me sad . . . I sometimes need support for scholastic materials like books, pens, shoes in order to learn well [but fail to get them] . . . Students at school take porridge but I don’t take and I stay very hungry. . . . I wish I could tell my mother and father to understand this situation and help me [out so that I] . . . – Girl child, 12 years, Lwengo.
When asked ‘Overall, how do you feel about having left and moving in with your family last year? How has the Experience been?’ the children gave their responses as tabulated below.
Similar to the caregivers, children expressed feelings of happiness, feeling good and more so having space to play with siblings and other children while at home suggesting that the institutional environment was restrictive in many ways.
Discussion
This study has revealed positive experiences following re-unification of children with homebased caregivers. In particular, there was continuous caregiver-child interactions prompting children to open up about their experiences of returning home as well as expressing their positive emotions and fears. Predominantly, children and caregivers expressed happy feelings and pointed to the growing trusting and loving relationships and responsiveness by parents towards children’s emotional, psychological, social and material needs. Perhaps because of the parenting training sessions, caregivers showed warmth, were supportive and responsive while relating with their children. In part, these practices are attributed to positive parenting which is associated with forming meaningful and secure attachments (Yousafzai, 2020), positive results in children’s growth such as higher child self-control and improved behaviour (reduced externalising and internalising behaviour); positive attitude towards criticism and self-respect and constructive communication with parents (Jouriles et al., 2008; Tildesley and Andrews, 2008). The adoption of positive parenting addressed some of the reasons for placement in RCFs related to family conflict and violence as Figure 1 revealed. Thus, capacity building for caregivers is a critical area in planning children’s reintegration.
There was a category of parents who perceived reunification negatively pointing out children’s exclusion from accessing free education offered by RCFs. While other parents were positive about receiving children, they were at the same time worried about the care burden and the risk of failing to support children’s education, a major reason why several children were sent to RCFs. These two categories of parents taken together, comprise those who experience daily struggles in providing for their families and largely live from hand to mouth. On one hand, their situation points to a failure of the formal social service and welfare system to effectively complement the non-formal support systems in providing relief for such households. Such poverty-stricken households face deep rooted stressors conducive for developing depression and anxiety among family members, with their children likely to perform poorly and risk school dropout (Vander Stoep et al., 2003); while an increased in stressors can lead to social impairments (Thapar et al., 2012) among children and family members.
Furthermore, where parents exhibited a negative attitude towards reintegration, it suggests that reintegration planning and implementation had limitations particularly, where the concerns of children and caregivers may not have been fully addressed. Font et al. (2018) argue that in such circumstances, reunified children are bound to re-enter residential care.
The findings revealed evidence of reintegration within the community given that children formed positive relationships with family and community members. Among fellow children, this was mainly through sports, an activity that increases a sense of competence, confidence and cooperation among children (Fraser-Thomas et al., 2005); and one that enhances stimulation and results into children’s cognitive, physical and social development. Such positive relationships result into social assets and opportunities that one needs to flourish in adulthood (Goldman et al., 2020).
Participant’s narratives indicate improvement in quality of care in relating with children and parental involvement in supporting children’s school learning tasks. It appears supportive programmes given to parents including case management, parenting education and a cash transfer grant could have made a positive contribution to the wellbeing of the reunified children. While RCFs often excel in meeting children’s basic needs compared to HBC they fall short in meeting psychosocial needs (James et al., 2017). Thus, reintegration followed by social support could make an important contribution towards improving reintegration outcomes (Walakira et al., 2014b). Children were also positive about the caretakers’ approach to discipline. Positive discipline was the preferred option for parents, however, with violent discipline still an option, this illustrates the complexity of behaviour change. Children did not consider negatively, disciplinary practices such as caning, which suggests normalisation of elements of harsh discipline. Yet harsh disciplinary practices during childhood have greater potential to reproduce violence in adulthood and present a risk factor for ill health and poor judgement (Maughan et al., 2013; World Health Organization and Calouste Gulbenkian Foundation, 2014).
Some children reunified with their biological parent’s experience behavioural and emotional problems (Lau et al., 2003). In this study, there were children that caregivers identified with errant behaviour, but associated this behaviour with the time they stayed in RCFs. The affected children though had difficulties in developing trusting relationships with caregivers which affected the quality of care they received. Vanderfaeillie et al. (2016) attribute the behavioural and emotional problems after reunification to the separation trauma that children experience when they return to their families of origin. The study findings suggest that the behavioural and emotional problems some of the returning children experienced and had to endure, were a result of cultural shocks and point towards the need for enhanced capacity building for caregivers.
Often, families to which children return have limited access to resources and thus their return could result in further deprivation. In some cases, children have to deal with reductions in access to the various necessities especially if the families cannot access required support (James and Roby, 2019). Under such circumstances, the assumption that institutions are the best place for meeting children’s basic needs is strengthened (James et al., 2017). Comparable experiences were documented by the current study and point to the need for strengthening livelihoods and social support services for families that receive back children. Heightened deprivations that children experience when they return home can negatively impact not only the physical, emotional and behavioural gains, but also psychosocial gains children experience in the long-term including happiness, positive relationships, emotional and psychological stability.
Conclusion
The study findings have revealed children’s and caregivers’ experiences following reunification with homebased caregivers. The key finding is that children and caregivers experienced reunification more positively and realised social, physical, emotional and psychological benefits, culminating into children’s reintegration. The positive experience of reunification underlines the role of core support services such as parenting, case management and financial support to affected families. Notwithstanding, the glaring inadequacy of social support to families facing the risk of separation highlights the enormity of the task in planning and implementing successful child reintegration efforts and the risk of undermining children’s experience of happy childhoods. The overarching need to meet family provisioning and more crucially, ensuring children’s continued access to quality education appear to underlie prospects for successful reunification and reintegration of children from residential to HBC, in resource constrained settings.
Footnotes
Acknowledgements
The study was funded under the Coordinating Comprehensive Care for Children (4Children) programme supported by the United States Agency for International Development (USAID Co-operative Agreement #AID-OAA-A-14-00061) (see ULS link: ![]() ) and was code named ‘Keeping Children in Healthy and Protective families). It was implemented by partners including Catholic Relief Services (CRS), Intra-Health and Maestral USA. Westat Inc. (USA) and Makerere University (Uganda) were responsible for the implementation of the study and worked in collaboration with CRS, Child’s I Foundation and TPO among other local partners.
) and was code named ‘Keeping Children in Healthy and Protective families). It was implemented by partners including Catholic Relief Services (CRS), Intra-Health and Maestral USA. Westat Inc. (USA) and Makerere University (Uganda) were responsible for the implementation of the study and worked in collaboration with CRS, Child’s I Foundation and TPO among other local partners.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received no financial support for the research through USAID Cooperative Agreement AID-OAA-A-14-00061.