
Abstract
Background:
Polypharmacy and potentially inappropriate medications are significant challenges in older adults’ medication management. The Consolidated Framework for Implementation Research (CFIR) is a comprehensive approach used to explore barriers and enablers to the healthcare system in guiding the effective implementation of evidence-based practices.
Objectives:
This study examines the barriers and enablers to promote safe medication management among older adults in Qatar from healthcare professionals’ perspectives. This includes identifying critical factors within the healthcare system influencing medication management and suggesting practical solutions to improve it.
Design:
The study employs a qualitative design. Focus Groups (FGs) were conducted with healthcare professionals from the geriatric, mental health and medicine departments of Hamad Medical Corporation (HMC), the leading governmental sector in Qatar serving the older adult population.
Methods:
Utilising the CFIR, this study analysed feedback from healthcare professionals through FGs at HMC. A combined inductive and deductive thematic analysis was applied to transcripts from five FGs, focusing on identifying barriers and enablers to safe medication management among older adults. Two researchers transcribed the audio-recorded FG discussions verbatim, and two researchers analysed the data using a mixed inductive and deductive thematic analysis approach utilising CFIR constructs.
Results:
We engaged 53 healthcare professionals (31 physicians, 10 nurses and 12 clinical pharmacists) in FGs. The analysis identified current barriers and enabler themes under different CFIR constructs, including inner settings, outer settings, individual characteristics and intervention characteristics. We identified 44 themes, with 25 classifieds as barriers and 19 as enablers. The findings revealed that barriers and enablers within the inner settings were primarily related to structural characteristics, resources, policies, communication and culture. On the other hand, barriers and enablers from the outer settings included patients and caregivers, care coordination, policies and laws, and resources.
Conclusion:
This study identified several barriers and enablers to promote medication management for older adults using the CFIR constructs from the perspective of healthcare professionals. The multifaceted findings emphasise involving stakeholders like clinical leaders, policymakers and decision-makers to address medication safety factors. A robust action plan, continuously monitored under Qatar’s national strategy, is vital. Further research is needed to implement recommended interventions.
Plain language summary
As people age, they often need multiple medications to manage their health conditions. However, taking medications that are not needed can cause harm. To improve medication management in this vulnerable population, it is essential to understand the barriers and enablers that healthcare professionals (HCPs) face. Our study used focus groups to explore these factors from the perspectives of healthcare providers in Qatar’s Hamad Medical Corporation (HMC). We used the Consolidated Framework for Implementation Research (CFIR) to collect and analyse the data.
Healthcare Professionals emphasised that the significant barriers to safe medication management in older adults include:
• The missing medication history in electronic health records in many cases.
• There is a lack of clinical decision support systems that guide and save prescribers time.
• There is limited access to services such as medication therapy management and telemedicine. These services could facilitate managing complex or urgent cases.
• Sometimes, communication between healthcare providers, patients, and caregivers is inadequate. It could be due to limited clinic time, HCPs’ experience, or patients’ health literacy.
• There are unclear guidelines and policies regarding prescribing, dispensing, and stopping medications for older adults.
• There is insufficient education for sub-specialists, junior HCPs, patients, and caregivers about the challenges of managing older adults’ medications.
• Limited patient engagement in their medication management plans could be due to low health literacy, social support, or physical or cognitive disabilities.
• In addition to overcoming the previous challenges, HCPs suggested implementing a national strategy to utilise, guide, and monitor all the efforts.
In conclusion, through our study, HCPs highlight the need for tailored national interventions to optimise safe medication management in older adults. The findings can inform the need for developing long-term and comprehensive strategies to help healthcare systems manage older adults’ medications, leading to better health outcomes for this vulnerable population.
Keywords
Introduction
The older adult population is expected to increase dramatically. By 2050, 16% of the world population will be 65 years or over, compared to 9% in 2019, living with chronic diseases and taking polypharmacy regularly. 1 Polypharmacy is considered one of the most significant prescribing challenges, contributing to patients’ non-adherence and increasing the likelihood of adverse drug reactions and drug interactions, which requires monitoring. 2
Potentially inappropriate medication (PIM) is used for medicines that should not be prescribed for older people because the risk of adverse events outweighs their clinical benefit, especially when there is an effective alternative therapy for the same indication. 3 It leads to a high risk of adverse drug reactions, hospital admissions, and mortality and reduces the patient’s functional capacity and quality of life. 4 PIMs in older adults, therefore, constitute a significant healthcare expenditure due to medication costs, recurrent Emergency Department (ED) visits and hospitalisations. 5 Reducing polypharmacy will reduce the likelihood of using PIMs and thus may benefit the health economy. 6
In the United States, 42.6% of ambulatory older patients were using at least one PIM, 7 while in a Qatari national retrospective study between 2016 and 2018 in the outpatient setting, 62.6% of older patients were using at least one PIM and 40.4% and 27.2% were using more than 5 and 10 medications, respectively. PIM was significantly associated with the risk of ED admission, bone fracture and constipation, while polypharmacy for more than 5 and 10 medications has also been associated with similar adverse events. 8 In another study of elderly patients under home healthcare services in Qatar, 38.2% had at least one PIM, while 56% were on drugs labelled to be used cautiously in older adults. 9 Internationally, efforts have been made to support reducing PIM use in older adults by covering barriers to improve medication management and patient safety, so it is essential to know what the barriers are to improve the healthcare system and provide the needed initiatives. International initiatives include Beers Criteria, WHO Global Patient Safety Challenge, European Union (EU) initiatives and the Canadian Deprescribing Network.10,11
Awareness of barriers is essential to facilitate a decision-maker to establish a strategy supporting improving medication management in older adults. 12 The Consolidated Framework for Implementation Research (CFIR) is the most used construct that supports the evaluation and understanding of barriers. Some developed theories ‘in-house’ adapted existing ideas or combined components of multiple approaches to meet the needs of their projects. 13 Nevertheless, the CFIR is a commonly used framework to facilitate designing, assessing and implementing evidence-based interventions in older adults’ prescribing. It provides a pragmatic structure to guide formative evaluations and build the implementation knowledge base across multiple studies and settings. 14 With its comprehensive domains (intervention characteristics, outer setting, inner setting, characteristics of individuals and implementation process), it supports a better understanding of the existing gaps and provides a roadmap for future research. 15
This study examines the barriers and enablers to promote safe medication management among older adults in Qatar from healthcare professionals’ (HCPs’) perspectives. This includes identifying critical factors within the healthcare system influencing medication management and suggesting practical solutions to improve it.
Methods
A descriptive qualitative approach was employed by conducting in-depth face-to-face Focus Group (FG) discussions to explore the perspectives and opinions of practising physicians, clinical pharmacists and nurses with experience in older people’s medication management. They were conducted between February 2020 and January 2021 in Hamad Medical Corporation (HMC), the leading public provider of secondary and tertiary healthcare to residents and citizens of Qatar. 16 The inclusion criteria to be invited to the FGs were being a practising physician, a nurse or a clinical pharmacist in the main specialities serving older adults in HMC (Geriatric Services, Older Adults Psychiatry and Medicine). The participants were selected using a purposive sampling technique. We invited experts from each department. We selected those with the most clinical experience serving older adults who have used the HMC-Cerner system for at least 3 years. Each FG consisted of prescribers, nurses and clinical pharmacists from each speciality, making our FGs heterogeneous. The Cerner system is an electronic health record (EHR) system used across all primary healthcare centres (PHCCs) and HMC facilities for patient care management. 17 All eligible participants were approached via email. All consenting participants signed the orientation sheet and informed consent form for voluntary participation. Dates for the FGs were arranged according to participants’ convenient times and locations. All participants have identification codes, which were added as follows: if participants were involved in FG group 1 and were participant number 6, their identification code is FG16. The participant numbers were determined by data saturation. Data saturation was achieved when no new themes or information emerged from the FG discussions. The research team continually assessed this throughout the data collection process.
We used the CFIR to explore the barriers and enablers 18 at HMC as an inner setting. PHCCs, communities and services other than HMC were considered outer settings. The domain intervention characteristic was used to describe the suggested enablers. The application of the widely used CFIR ensured that all influences on safer older adults’ prescribing were captured systematically. CFIR supports focusing exclusively on the experiences of different stakeholders, which helps to understand relevant enablers and barriers better. 19
We formulated a list of predetermined open-ended questions developed according to previously published studies using the CFIR as a standardised topic guide (Supplemental Appendix 1).
Open-ended questions were designed to encourage in-depth information sharing and subdivided into six sections. The first section focused on the participants’ experiences of factors affecting the initiation, monitoring and deprescribing of medicines in older people. The remaining areas focused on factors affecting the intervention, outer setting, inner setting, people and suggestions for improvement. At least two investigators moderated each FG to obtain comprehensive perspectives to ensure everyone could share their views, encourage quiet people to share their ideas, prevent dominant voices from taking over the conversations and ensure that we collected diverse opinions from all participants. Sessions were conducted in English, recorded by audio devices and kept in a secure area to maintain confidentiality. The records were transcribed manually immediately after each session. The CFIR domains were redefined to align with our study topic. If the audio recordings were unclear, written notes were taken for the essential points as a backup tool.
In our study, thematic analysis was conducted using both inductive and deductive approaches. Initially, we employed an inductive thematic analysis to categorise HCPs quotes into relevant themes under the primary CFIR constructs (inner, outer, individual characteristics and suggested intervention characteristics). For example, the themes of policies and resources come under inner and outer settings, while capability and motivation themes come under the individual’s characteristics. This approach was beneficial because the CFIR framework was not specifically tailored for analysing healthcare system components. This inductive process identified themes directly emerging from the data, reflecting our participants’ unique perspectives and experiences. Subsequently, we engaged in deductive thematic analysis to map these emergent themes onto the broader constructs and domains of the CFIR. This method allowed us to align our specific findings with this established implementation framework, integrating our unique insights into a broader theoretical context. Such a combination of inductive and deductive approaches ensured a comprehensive exploration of barriers and enablers to safe prescribing for older adults, including detailed insights into the characteristics of HCPs and their most suggested interventions.
We developed subdomains under each CFIR domain to refine our analysis further and then identified healthcare-related components. This step was crucial in building a robust coding framework that could capture the nuances of our data. All inductive themes under their respective CFIR domains were categorised as barriers or enablers. Barriers were defined as obstacles to safer prescribing. Enablers were described as potential solutions to overcome barriers or highlighted features of an intervention or system that could lead to safer prescribing practices. This provided a clear overview of the current situation and allowed us to suggest prospective modifications in healthcare practices.
To enhance the trustworthiness of our findings, we utilised several strategies to ensure they were credible, dependable, confirmable and transferable. Regarding credibility and dependability, two researchers performed manual and line-by-line coding to identify themes and correlate them with the list of CFIR subdomains. The research team continuously reviewed the domains and their definitions against our inductive and deductive coding; moreover, credibility was assured by seeking feedback from participants to validate interpretations and ensure they resonate with their experiences and to assure dependability, consensus among researchers conducting the analysis confirmed through regular meetings to discuss interpretations and resolve discrepancies. Developed themes were checked to ensure they adequately described the data they related to and that enough supporting evidence, such as append quotes, was available to support the confirmability and trustworthiness of our interpretation. For transparency, we have recorded and presented all steps undertaken in our data collection and analysis. We have presented details of the demographic and contextual settings to allow readers to understand the transferability of our findings. We have considered ensuring that our sample is as diverse as possible to represent this setting fully. The definitions of all domains and the evolved themes of barriers and enablers are detailed in Tables 1 and 2. We adhered to the Standards for Reporting Qualitative Research (SRQR) in its reporting methodology. 20 Supplemental Appendix 2 has the SRQR checklist.
The barriers themes of safe older adults prescribing emerged from focus groups and classified according to CFIR constructs.
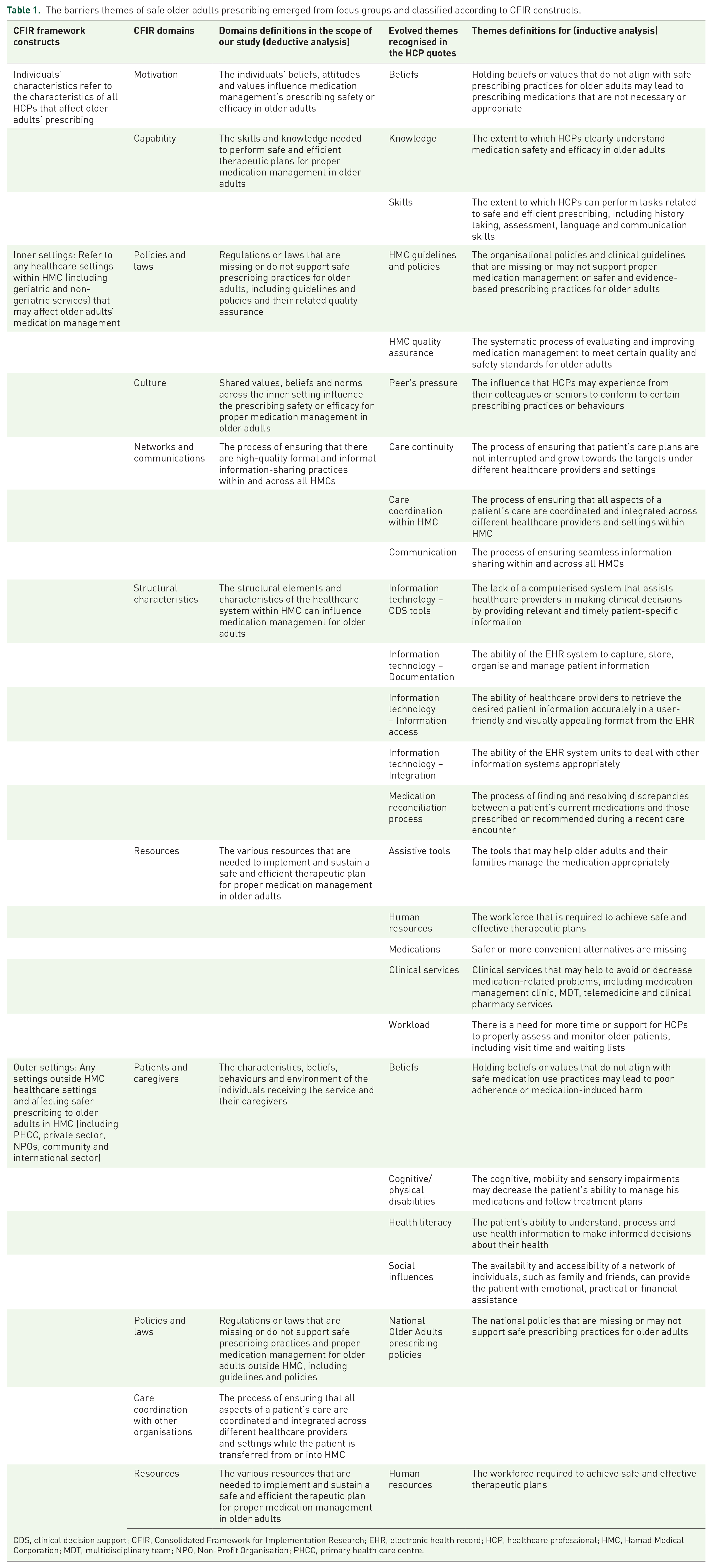
CDS, clinical decision support; CFIR, Consolidated Framework for Implementation Research; EHR, electronic health record; HCP, healthcare professional; HMC, Hamad Medical Corporation; MDT, multidisciplinary team; NPO, Non-Profit Organisation; PHCC, primary health care centre.
The suggested enablers with the relevant CFIR characteristics, details and frequency of quotes (N = 141 quotes).
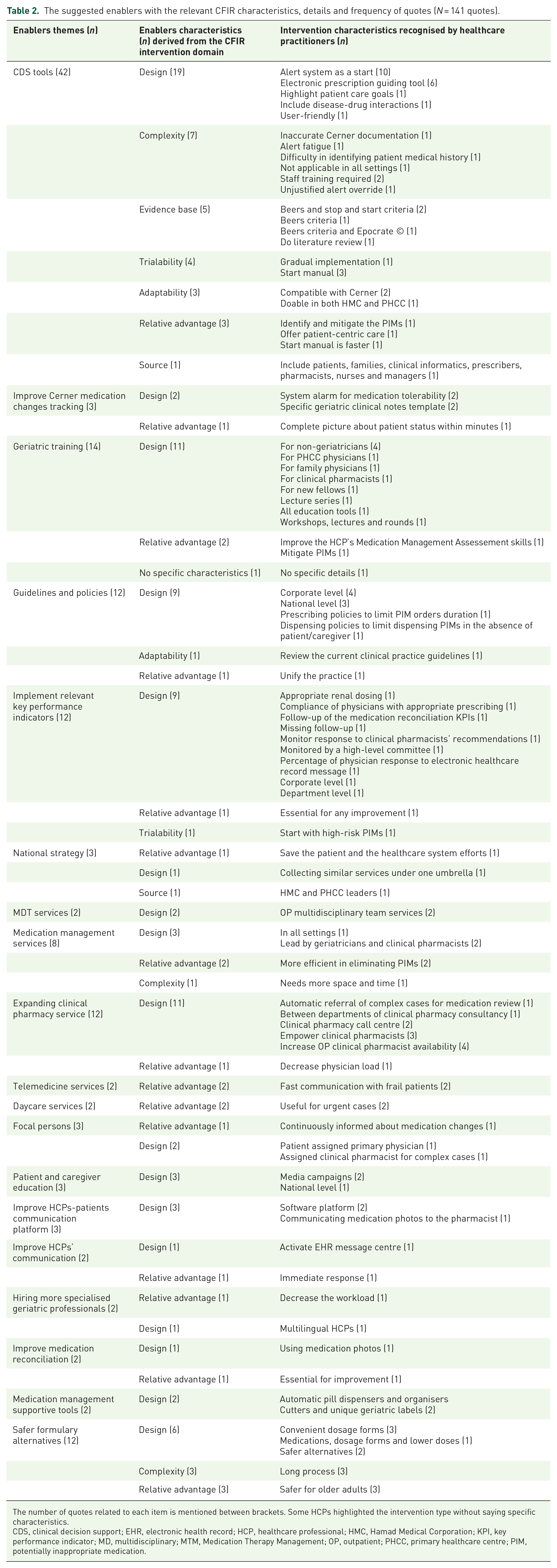
The number of quotes related to each item is mentioned between brackets. Some HCPs highlighted the intervention type without saying specific characteristics.
CDS, clinical decision support; EHR, electronic health record; HCP, healthcare professional; HMC, Hamad Medical Corporation; KPI, key performance indicator; MD, multidisciplinary; MTM, Medication Therapy Management; OP, outpatient; PHCC, primary healthcare centre; PIM, potentially inappropriate medication.
Results
Participants
The study included 53 participants (31 physicians, 10 nurses and 12 clinical pharmacists) across five FGs. The average duration of each FG was 91 min, with a standard deviation of 20 min. The participants had an average of 20.9 years of total experience and 9.1 years of experience working at HMC. On average, they had 12.0 years of experience specifically with older adults in various departments, including geriatrics (45.3%), older adults psychiatry (32.1%), internal medicine (20.8%) and physical medicine and rehabilitation (1.9%). The participants represented various professions, including physicians (58.5%), clinical pharmacists (22.6%) and nurses (18.9%). Among the participants, 37.7% were female and 62.3% were male. The participants received their training from different countries (Table 3).
Participants’ characteristics.

Frequency and percentage are mentioned between brackets unless otherwise noted in the left column.
µ (SD), mean (standard deviation); UK, United Kingdom; US, United States.
Barriers and suggested interventions to safe prescribing for older adults
The analysis identified current barriers and enablers under different CFIR constructs, including inner settings, outer settings, individual characteristics and intervention characteristics in 208, 58, 45 and 131 unique quotes, respectively. We identified 44 themes, 25 of which are barriers and 19 enablers (Tables 1 and 2). A summary diagram for all barriers is provided in Supplemental Appendix 3. The CFIR construct of Implementation of Innovation was outside the study’s remit, and thus they were not identified.
Inner settings barriers
The findings of the barriers within the inner settings domain were primarily related to structural characteristics, resources, policies, communication and culture.
Several interrelated themes belonging to the inner setting of HMC were identified as barriers that may not allow HCPs to intervene appropriately with the older adults’ medications. The complexity of and interference between factors affecting older adults’ medication management in different settings was clarified by one participant who said, ‘When we visit patients at home, we find many full bags of medications prescribed by different HCPs and even different hospitals while the carer/patient are not well oriented to handle all these medications. It is a multilevel problem’ (FG432).
HCPs reported that a barrier was the lack of coordination within HMC. They mentioned that medication management responsibility was dispersed between prescribers and spoke about communication struggles.
‘Some physicians insist that the original prescriber must be contacted before changing his medications. . .It is not easy to change others’ medication orders’ (FG110). This practice affects medication reconciliation: ‘Each prescriber handles his prescribed medication without touching other colleagues’ prescriptions’ (FG16). The participants reported peer pressure in prescribing. ‘It is difficult to change senior prescribers’ prescribing pattern to follow the recent evidence, and juniors are following their practice’ (FG113).
Additionally, participants expressed challenges in monitoring patients at home after medication changes, saying that ‘Monitoring patient at home after medication changes is difficult. . .patient could suffer from hypoglycemia or hypotension at home after changing antidiabetic or antihypertensive regimen, so they are barriers to take the appropriate action in some cases’ (FG325).
HCPs also reported the lack of clinical pharmacists: ‘Some teams have no clinical pharmacist around so that medication side effects may be overlooked’ (FG560). The pharmacist shortage could be added to the captured workload theme, where physicians highlighted other aspects of the workload burden. Insufficient time for comprehensive reviews and discussions with older patients and their families usually leads to incomplete medicine reconciliation. They expressed the challenges they face, such as the burden of reviewing frequent notes, which increases the workload due to the time-consuming nature of patients’ clinical status and the need to prioritise specific tasks due to limited time and communication. One participant shared his experience, stating, ‘We have insufficient time for each older adult to review the frequent notes and discuss all medical issues with the patient and the family’ (FG16). Another participant mentioned, ‘Due to limited time and communication, we had to do partial reconciliation only for the medications we prescribe’ (FG551).
We need to hire more specialised physicians and clinical pharmacists who understand the unique needs of older adults. (FG556)
The recruited HCPs were also recommended to be multilingual to improve communication with the diversity of languages within the community. The HCP-patient communication platform was also suggested to enhance communication for safer medication management. ‘We need to have a platform for patients to communicate with their HCPs and to be able to share medication photos with pharmacists to ensure accurate medication lists’ (FG113). Integrating telemedicine was identified as a facilitator in overcoming barriers to healthcare access for older adults, particularly those with mobility issues. Participants recommended expanding telemedicine for medication consultations, follow-ups, medicine reconciliation and medication-related education for patients and caregivers. One participant noted, ‘Telemedicine can be helpful for older adults who face difficulties in travelling, especially for medication follow-up’ (FG436).
Introducing Focal (nominated Persons) as points of contact in various departments was also suggested to communicate highly complex cases when immediate actions are required. ‘We need an immediate communication method with other specialists and clinical pharmacists in other departments’ (FG111). Additionally, assigning a primary care physician to each older adult to facilitate such communication was proposed. However, one participant expressed concern that some older adults do not have dedicated family physicians who are consistently informed about medication changes, and ‘some may not even know who their primary care physician is’ (FG434).
Participants emphasised the necessity of involving multiple specialities to address a significant percentage of polypharmacy cases. ‘up to 20% of polypharmacy patients may require the participation of different specialities in decision-making regarding medication changes in outpatient settings’ (FG435). HCPs suggested providing Medication Therapy Management (MTM) services in person or through expanded telemedicine to address complex polypharmacy cases. However, they acknowledged that this approach would require adequate space and time; one participant mentioned, ‘Deprescribing needs space and time’ (FG322). Elderly Urgent Care Units (Daycare) offering short hospital stays were proposed to facilitate urgent medication reviews for high-risk patients requiring laboratory tests and investigations to address their medication-related problems. To enhance medication management in complex cases requiring extensive discussion, one participant proposed ‘the establishment of a specialised polypharmacy clinic led by a physician and a clinical pharmacist “A special polypharmacy clinic led by physician and clinical pharmacist could help to decrease the inappropriate medication use in older adults”’ (FG556). Expanding clinical pharmacy services was suggested to alleviate the burden on physicians and minimise inappropriate medication use in older adults. Suggestions included implementing an automated referral system for complex cases to undergo medication reviews, facilitating interdepartmental consultation with clinical pharmacists, establishing a clinical pharmacy call centre and increasing the availability of clinical pharmacists in Outpatient Departments (OPDs).
If the clinical pharmacist is not present at the OPD clinic, I recommend automatically referring older adults who are prescribed a certain number of medications to undergo clinical pharmacy review. (FG555)
Other enabling factors proposed included collaboration between clinical pharmacists in geriatrics and mental health clinical pharmacists to make decisions regarding therapeutic plans as stated by (FG110) ‘Original prescribers must be contacted before changing his medications’.
. . .Geriatricians cannot change others’ medication orders. . . the geriatric clinical pharmacist could contact the clinical pharmacist in mental health, for example, to decide about the therapeutic plan. (FG110)
Establishing a clinical pharmacy call centre could provide temporary solutions to medication-related queries across all clinics, as stated by (FG550). ‘Drug information service is insufficient to solve our OP clinic medication queries. We need more clinical pharmacist support, and they need more authority to handle therapeutic problems. This is a real challenge, particularly for such a group of elderly with polypharmacy’. One participant highlighted the limitations of drug information services and the importance of having clinical pharmacists in outpatient clinics as he stated, ‘Yes, it could be beneficial to have clinical pharmacists in the OP clinics’. (FG558). Guidelines and policies were suggested to be reviewed at the corporate and national levels. Suggestions included prescribing policies to limit older adults’ PIM order duration and dispensing policies to limit dispensed PIMs without a patient/caregiver or pharmacist intervention. Participants also suggested implementing relevant key performance indicators (KPIs) to monitor the implementation of the guidelines and ensure quality improvement.
Having geriatric safe prescribing clinical practice guidelines and policies are highly recommended. (FG215) Implement relevant Key Performance Indicators (KPIs) with the corporate leadership. . .Share results with HCPs monthly and acknowledge the best performance. (FG112).
HCPs proposed policies that empower clinical pharmacists.
Clinical pharmacists should be the medication police, so we should empower them to do the job. (FG221) Clinical pharmacists should be more involved in medication therapy management and can do this through telemedicine too. (FG555)
Additionally, HCPs suggested that dispensing policies should control PIMs, emphasising the need for pharmacist involvement, documentation of the clinical need when PIM is prescribed and the availability of safer alternatives before dispensing. One participant said, ‘Pharmacists should not dispense PIM without calling the prescriber to confirm the clinical need and safer alternative availability’ (FG552).
The national guidelines and policies subdomain emerged as a barrier to safe prescribing. Participants expressed the need for comprehensive national guidelines encompassing the public healthcare sector and the private and non-governmental organisation sectors providing geriatric services. The absence of unified guidelines and policies across these sectors hampers the achievement of safe prescribing goals. As one HCP emphasised, ‘Private and other governmental and Non-Profit Organisations (NPOs) sector providing health care geriatric services are part of the challenge. National Guidelines are mandatory to achieve these targets’ (FG114).
Suggested enablers included incorporating guidelines in the electronic clinical decision support (CDS) systems tool.
‘CDS can help us identify and stop PIMs and offer patient-centric care for older adults at different encounters’ (FG112). Physicians, pharmacists and nurses agreed that the EHR should facilitate proper documentation and access to information to guide prescribers for appropriate prescribing in older adults without clear guidelines and supportive technologies.
Concerns have been raised regarding technical issues such as system bugs, ‘Technical difficulties to add new orders due to system bugs can waste HCP time’ (FG330). Some were worried about the IT system (Cerner) not supporting mandatory documentation of medication management.
Medications are prescribed from other specialities without clear documentation of the indication or treatment plan, for example, dual antiplatelets without specific reason’. (FG557)
Participants also highlighted the absence of medication administration supportive tools and devices, such as automatic pill dispensers, organisers, cutters and unique labels for older people with specific needs.
No available medication administration supportive tools and devices, such as automatic pill dispensers and organisers, cutters, and special geriatric labels. (FG239).
Outer setting barriers
Barriers related to the outer settings of the healthcare system encompass various factors that impact prescribing safety. The outer setting barriers consist of themes related to patients and caregivers, coordination with other organisations, policies and resources. Within the patients and caregivers domain, certain beliefs and cognitive/physical disabilities were identified as barriers to safe prescribing. HCPs encountered challenges in deprescribing medications when patients held strong beliefs in favour of their current medication regimen, even in cases where there was no clear indication. One HCP shared, ‘One patient has prescribed four antipsychotics from abroad without real indication; we failed to convince him to deprescribe’ (FG215). Moreover, the rapidly changing needs of older adults, particularly those with cognitive or physical disabilities, further complicate prescribing decisions and require individualised approaches to ensure medication safety. As one HCP stated, ‘Many of our older adults cannot read or write, so it is difficult to educate them using the ordinary ways’ (FG113).
Furthermore, inadequate human resources, particularly in the private sector, pose a significant barrier to effective medication management. The lack of sufficient staff, including family physicians and clinical pharmacists, undermines the ability to monitor and follow-up on medication changes, especially outside the primary healthcare system.
Family physicians and clinical pharmacists should follow up on medication changes, but there are not enough staff to do the job, particularly outside HMC. (FG432)
In the domain of care coordination with other organisations, HCPs highlighted the lack of access to documentation and communication methods with professionals in the private healthcare sector as a barrier. The absence of seamless information sharing and communication channels can lead to critical information gaps in clinical decision-making processes, potentially compromising medication safety.
We do not have access to private healthcare sector documentation or contact method with their professionals, so vital information in clinical decision-making could be missed. (FG588)
The barriers related to the characteristics of HCPs
All the previous complex challenges in older adult prescribing make the knowledge of HCPs the most reported theme under the individual characteristic’s domains: capabilities and motivations. Participants highlighted that ‘older adults have unique disease presentation and management, which requires special training to choose appropriate treatment’ (FG110). Under the skills theme, it was noted that ‘evaluating the patient’s/carer’s medication management capacities is usually overlooked, leading to significant failure to achieve therapeutic goals’ (FG239). Lack of this vital skill could lead to the failure of therapeutic plans. It was captured under the motivation domain.
‘Avoiding medication changes due to the consequences and responsibility of monitoring these changes’. (FG112), which could be intercorrelated with previously stated barriers of not having clear assigned responsibility for who should monitor the patient when there are changes in previously prescribed medication due to lack of guidance or policies to monitor prescribers’ performance. The motivation domain also captured the belief theme, with physicians ‘avoiding medication changes due to the consequences and responsibility of monitoring these changes’ (FG112). These gaps in knowledge and skills make CDS tools more crucial to guide and monitor performance and quality improvement in medicine reconciliation.
Most participants suggested that better education about pharmacy in older people should be provided for HCPs from other specialities through lecture series, workshops and grand rounds. ‘Geriatric training should be for the Primary Health Care Corporation (PHCC) physicians to appropriately identify, manage appropriately, and – if needed – refer older adults with PIM or polypharmacy’ (FG435). Participants emphasised the importance of improving medication management capacities and assessment skills: ‘Evaluating medication management capacities should be part of the regular assessment for older adults and their health care professionals’ training courses. This includes social, physical, cognitive, and psychological capacities (FG239).
Characteristics of the suggested interventions/enablers
The development of CDS tools was viewed as a collaborative effort involving various stakeholders. This inclusive approach was seen as crucial for achieving successful implementation. ‘Patients, families, clinical informatics, prescribers, pharmacists, nurses, and managers should be part of introducing the process of CDS. . .’ (FG329). The design of the CDS tool emerged as a prominent topic of discussion. These included providing a comprehensive patient medical history and care goals, addressing disease-drug interactions and ensuring user-friendliness. Participants highlighted implementing an alert system as a crucial starting point for the tool. Additionally, if applicable, including electronic prescription guiding tools was considered beneficial. An HCP expressed that ‘EHR alerts would be useful for identifying high-risk drugs for the elderly’ (FG214).
However, participants also acknowledged potential challenges associated with CDS tool design, such as alert fatigue, unjustified alert overrides, difficulty accessing patient medical history, issues with inaccurate Cerner documentation and limited applicability in all healthcare settings. A participant suggested, ‘Alarming systems should be refined and monitored to overcome the problem of inappropriate alert override’ (FG219). Another participant questioned the feasibility of capturing all patient details from the system, stating, ‘Tool should be able to identify all patient details from the system. Do you think it is easy to do?’ (FG112). It was also noted that while electronic tools were preferred over paper-based tools, improvements in Cerner documentation, particularly regarding diagnoses, were necessary. One participant mentioned, ‘Start as electronic tools, paper tools are not useful, but the Cerner documentation as diagnoses need to be improved first’ (FG435).
Participants suggested that the CDS tools incorporate established criteria such as the ‘Beers’ or ‘Stop and Start’ criteria. Additionally, they emphasised the importance of conducting a literature review to ensure an evidence-based design for the tool. Regarding implementation, participants highlighted the need for the CDS tool to be usable in both the HMC and PHCC settings. They recommended a gradual implementation approach, starting with testing the tool’s usefulness and incorporating their feedback to refine the final framework of the CDS tool.
Check the tool’s usefulness with one physician and a few patients and apply their suggestions to reach the final framework of the CDS. (FG111)
Discussions
This study explored the barriers and enablers to safe medication management of older adults in Qatar from the HCP’s perspective. Our findings show many intercorrelated factors that require the involvement of multiple stakeholders, decisions and policymakers at departmental, corporate and national levels. The analysis identified barriers under different CFIR constructs, including inner settings (HMC), outer settings (PHCCs, private sectors and community) and individual characteristics of HCPs.
The key findings focus on the need to improve information technology, such as empowering Cerner documentation and access to information, using a CDS system, which has a well-known impact in reducing medication error, 21 supporting implementing policies and guidelines for older adults prescribing, prescribing quality monitoring, communication, care coordination, patient and caregiver engagement, and HCP knowledge, skills and competencies.
The study identified barriers and enablers that can significantly impact the safety and effectiveness of medication management. Several studies addressed communication between HCPs and patients through multidisciplinary approaches to avoid patient resistance, the need for CDS, clinical pharmacists, geriatric medicine multidisciplinary services and education as a multifaceted intervention. Any agenda to improve prescribing should address and account for these causes and consider the different needs of patients, prescribers and the environment.22,23
Information technology, such as EHRs and CDS, represents both a barrier and an enabler of medication management. A systematic review explores trials showing that CDS enhances clinical decision-making and potentially reduces medication errors. 24
Missing functions in the EHR for quick access to patients’ medication-related problem information and time-consuming for getting clear medication history, inadequate CDS can result in medication errors. Clinical services, medication management clinics and safe formulary medication alternatives as resources are essential. Patients and caregivers lack adequate clinical services and resources to enhance medication management, address medication-related challenges and manage medications effectively. This barrier is similar to the obstacle faced by community pharmacists in Qatar, who reported concerns about time, dedicated consultation area and support staff as significant barriers towards Medication Use Review implementation. 25
Policies and guidelines represent significant barriers to medication management, which causes no clear PIM deprescribing responsibilities among prescribers from different schools and training backgrounds. Providing a standardised framework would be an enabler to reduce PIM and polypharmacy. Protocol and clinical guidelines include KPIs with proper monitoring that significantly promote appropriate medication management.
It is worth noting that the barriers identified are general, interrelated and not independent of each other. Addressing these comprehensive medication management programmes that provide adequate clinical services and resources is required. The Qatar National Strategy has a crucial role in supporting and ensuring that HCPs under different sectors (inner and outer settings) follow evidence-based guidelines and apply KPIs to monitor safe medication management and performance improvement across different sectors.
Communication and care coordination represent other significant enablers of medication management suggested for inner and outer settings, emphasising the need for collaboration among healthcare providers, patients and caregivers.
There are not enough clinical professionals in the geriatric medicine speciality, unlike other HMC facilities. This is exacerbated by a lack of specialised clinical services for older adults, including clinical pharmacists, medication management clinics, telemedicine, clinical pharmacy and multidisciplinary services with a clear role in solving medication-related problems, particularly among different specialities in outpatient settings to facilitate communication.
Patient and caregiver knowledge, skills and competencies are essential for medication management, as patients and caregivers play a critical role in managing medications effectively. 26 Education and support can empower them to self-manage their medications, identify medication-related challenges and enhance medication adherence. Education and support interventions have been recognised as crucial in empowering patients to proficiently self-manage their medications, effectively identify medication-related challenges and enhance medication adherence, thus significantly improving treatment outcomes.
A systematic review comprehensively examines the impact of educational and support interventions in this domain, shedding light on their effectiveness and emphasising their importance in patient-centred care. 27
This study’s findings are consistent with previous research, which has also highlighted the need for interventions such as CDS systems, optimising the use of EHRs, laws and policies, and KPIs, in addition to providing MTM clinics, and education to improve medication management in older adults.28,29 The real-world initiatives aimed at improving medication management in older adults internationally. For instance, the European SIMPATHE project focuses on stimulating innovation in managing polypharmacy and enhancing adherence among the elderly population. 30 Similarly, Qatar’s national strategy prioritises healthy ageing, underscoring the importance of appropriate medication management. This involves concerted efforts from leaders and decision-makers across governmental and private sectors to develop and implement action plans that promote effective medication management practices for older adults.
Strengths and limitations
Our study has several strengths. To the best of our knowledge, this is the first study in the Middle East that explored the medication management challenges of older adults from HCPs’ perspectives. The study included many participants from different clinical and administrative roles, including physicians, nurses and clinical pharmacists, among others, from various specialities, such as geriatrics, mental health and medicine departments. This diverse background of participants provided a comprehensive understanding of challenges faced in Qatar about the medicine management of older adults, and we can identify a wide range of possible enablers to overcome these challenges.
In addition, we utilised the CFIR approach to categorise the identified barriers and enablers, providing a standardised data analysis framework. Therefore, our findings can inform the development of national strategies in Qatar to assist HCPs in better managing older adults’ medications, leading to better health outcomes for this vulnerable population.
We recognise certain constraints as well. All participants in our study were employees of the HMC, potentially resulting in a conservative outlook and a lack of diverse perspectives and experiences. As reported by these participants, the barriers from the outer setting are presented through the lens of HMC’s viewpoint. Despite these limitations, our study offers valuable insights into the barriers and enablers for enhancing medication management in older adults. These insights came from the perspectives of HCPs from various disciplines, encompassing a wide range of aspects and areas with potential for improvement.
The study was applied to promote safe medication management for older adults, mainly in HMC, but the result is applicable to all similar healthcare systems in Qatar and abroad. Additionally, as with all similar FG studies, our study entails interpreting quotes. This might have introduced bias and misunderstanding, mainly when participants come from diverse nationalities with non-native English proficiency.
Conclusion
In this study, we have identified several barriers and enablers to promoting medication management for older adults using the CFIR constructs from the perspective of HCPs. Our study, therefore, provides deeper insight into HCPs’ challenges in managing older adults’ medications, which can inform interventions tailored to the local context. The comprehensive, multifactorial findings highlight the need to involve multiple stakeholders, including clinical and administrative leaders, policymakers and decision-makers, to identify and improve the factors impacting medication safety in older adults. We recommend developing a robust action plan with continuous monitoring of improvement processes across various sectors under the national strategy in Qatar. Further research is necessary to investigate the implementation of recommended interventions to promote safe medication management for older adults in Qatar and similar healthcare systems.
Supplemental Material
sj-docx-2-taw-10.1177_20420986241272846 – Supplemental material for Enhancing medication management of older adults in Qatar: healthcare professionals’ perspectives on challenges, barriers and enabling solutions
Supplemental material, sj-docx-2-taw-10.1177_20420986241272846 for Enhancing medication management of older adults in Qatar: healthcare professionals’ perspectives on challenges, barriers and enabling solutions by Ameena Alyazeedi, Carrie Stewart, Roy L. Soiza, Derek Stewart, Ahmed Awaisu, Cristin Ryan, Moza Alhail, Abdulaziz Aldarwish and Phyo Kyaw Myint in Therapeutic Advances in Drug Safety
Supplemental Material
sj-jpg-3-taw-10.1177_20420986241272846 – Supplemental material for Enhancing medication management of older adults in Qatar: healthcare professionals’ perspectives on challenges, barriers and enabling solutions
Supplemental material, sj-jpg-3-taw-10.1177_20420986241272846 for Enhancing medication management of older adults in Qatar: healthcare professionals’ perspectives on challenges, barriers and enabling solutions by Ameena Alyazeedi, Carrie Stewart, Roy L. Soiza, Derek Stewart, Ahmed Awaisu, Cristin Ryan, Moza Alhail, Abdulaziz Aldarwish and Phyo Kyaw Myint in Therapeutic Advances in Drug Safety
Supplemental Material
sj-xlsx-1-taw-10.1177_20420986241272846 – Supplemental material for Enhancing medication management of older adults in Qatar: healthcare professionals’ perspectives on challenges, barriers and enabling solutions
Supplemental material, sj-xlsx-1-taw-10.1177_20420986241272846 for Enhancing medication management of older adults in Qatar: healthcare professionals’ perspectives on challenges, barriers and enabling solutions by Ameena Alyazeedi, Carrie Stewart, Roy L. Soiza, Derek Stewart, Ahmed Awaisu, Cristin Ryan, Moza Alhail, Abdulaziz Aldarwish and Phyo Kyaw Myint in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
We want to express our sincere gratitude to Dr Abdelaziz Darwish, Deputy Chief Medical Officer and A/CEO of RH, for his invaluable support and guidance throughout this research project; Dr Hanadi, chairperson of the Geriatric and Medical Director of the Geriatric department; and Dr Ahmed Al-Mohammed, Head of the medicine department; Dr Youssef Almoslimani, Medical Director of Hamad General Hospital; and Dr Nasser Masoudi for their support in securing the necessary resources and facilitating access to facilities subjects. Their continuous encouragement and belief in the significance of our research motivated us to overcome challenges and strive for excellence. We would also like to thank the entire RH, Medicine and Mental Department team for their support and collaboration throughout this project. Their contributions have been invaluable to the successful completion of this research. Lastly, we thank the Medical Research Centre (MRC) for funding this research and providing Research Assistant Dr Ahmed Fouad. We appreciate his effort. We also thank all the participants and individuals who generously devoted their time and effort to this study. Without their cooperation, this research would not have been possible.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.