
Abstract
Introduction:
Older adults continue to receive potentially inappropriate medications necessitating the need for medication optimization, by deprescribing. To ensure a holistic approach to deprescribing, it is essential to understand the perception of older adults towards deprescribing. This study aimed to assess the attitude of older ambulatory patients towards deprescribing and to identify factors predicting their willingness to deprescribe.
Methods:
A cross-sectional survey was conducted in central Nepal between March and September 2019 among 385 older ambulatory care patients (aged ⩾65 years) who were taking at least one regular medicine. The perception of patients towards deprescribing was assessed using the revised Patients’ Attitudes Towards Deprescribing (rPATD) questionnaire via a face-to-face interview method. Descriptive statistics were performed to describe patients’ characteristics and their attitudes towards deprescribing. A multivariate logistic regression analysis was used to determine predictors of the willingness of older ambulatory patients towards deprescribing.
Results:
The median [interquartile range (IQR)] age of patients was 72 (8) years. Nearly three in five patients (64.9%) had hypertension, with 11.2% having polypharmacy. More than half of the patients (57.4%) would be willing to stop one or more of their regular medicines if their doctor said it was possible to do so. Regression analysis showed that age [odds ratio (OR) 0.946; 95% CI 0.913, 0.981; p = 0.003] and concerns about stopping medicine score (OR 0.541; 95% CI 0.334, 0.876; p = 0.013) were predictors of the willingness of the older patients towards deprescribing.
Conclusion:
One in two older ambulatory care patients in Nepal would be willing to have one or more of their medicines deprescribed. The factors predicting their willingness to deprescribe are their age and concerns about stopping medicines. Clinicians should consider discussing the possibility of deprescribing with older patients for the prevention of potential medication-related harms.
Plain Language Summary
What do older Nepalese patients think about withdrawal or dose reduction of an inappropriate medication?
Introduction
The ageing of the population presents many challenges to the healthcare system including a high prevalence and complexity of diseases in older adults requiring healthcare providers to prescribe multiple medications for disease management.1,2 This can lead to polypharmacy, which not only increases the risk of adverse drug reactions but also raises morbidity and mortality.3,4 Advancing age alters the physiological conditions of the body such as the pharmacokinetics and pharmacodynamics response to medicines, which leads to medication-related harm and ultimately poor health outcomes.3,5
Although the impact of inappropriate prescribing on patient health outcomes is well documented, evidence suggests that older adults continue to receive potentially inappropriate medications (PIMs).6,7 There is sufficient evidence that links PIMs with poor health outcomes in older people. PIMs have been known to be associated with reduced quality of life, adverse drug reactions, falls, hospitalizations, and mortality.8,9 The health risk of continuing such medicines (or the same dose) in older patients outweighs the benefits if PIMs are not deprescribed.1,2
Deprescribing is a structured approach to optimize the use of PIMs in older adults. 10 It is a process of withdrawal or dose reduction of an inappropriate medication under the supervision of a healthcare professional.11,12 Though many Western countries have adopted the deprescribing approach, evidence on deprescribing is lacking from developing countries including Nepal, suggesting the concept is yet novel. Studies from Nepal suggest that a considerable number of older patients receive PIMs,13–17 reporting an estimated prevalence of PIM in older adults ranging from 5 to 19%. To facilitate the implementation of deprescribing practices in the Nepalese context, it is essential to understand the perception of patients who could largely benefit from this concept. This study aimed to assess the attitude of older patients towards deprescribing and factors influencing their willingness to deprescribe.
Methods
Study design and population
A cross-sectional survey was conducted in central Nepal between March to September 2019 among older ambulatory patients aged at least 65 years who visited the outpatient department of the hospital for follow-up or medication refill and taking at least one regular prescription medicine regardless of their diagnosis. Those unable to participate due to their medical conditions (physical or psychological) were excluded.
Study site, sample size and sampling
This study was conducted in three hospitals located in the Chitwan district of Nepal that included a government hospital and two private teaching hospitals. Chitwan district was purposely selected based on its geographical location as it is centrally located to the country and is considered a medical hub of the nation. The selected district-level government hospital and two teaching hospitals provide medical services to a wide array of patient groups and diseases. Given that the willingness to deprescribe in this setting was not known, the sample size was estimated to be 385 considering cross-sectional design, 50% willingness to deprescribe, 95% confidence interval, and 5% error margin. The required sample size was conveniently taken from the two hospital types on approximately equal proportion [n = 193 from one government hospital and n = 192 from two private teaching hospitals (n = 96 from each)].
Data collection
A face-to-face interview was conducted to assess patient characteristics (demography, medical condition, and polypharmacy) and data on attitude towards deprescribing. Any patient on five or more medicines was considered to be on polypharmacy. The patient’s characteristics were also assessed from their outpatient cards while the attitude was assessed using the validated revised Patients Attitude Towards Deprescribing (rPATD) tool. 18 Hospitals in Nepal use an outpatient card for ambulatory patients which generally consists of information on their demographics, disease, laboratory findings, and medications. The data on patient characteristics present in the outpatient card was confirmed in a face-to-face interview with additional information that was self-reported by the participant. The interview was conducted by pharmacists and final-year pharmacy undergraduate students who had completed their hospital internship. The interview took place within the counselling area of each hospital. The counselling area referred in this study included a separate room for counselling of patients owned by the hospital pharmacy where patients are prompted after dispensing of medication(s) or an area where patients are counselled about their medication(s) during dispensing of medicines.
rPATD tool
The permission to translate and use the rPATD tool for this study was sought from the corresponding author of the rPATD tool. The tool did not have an official licence for use, but a list of conditions was agreed prior to approval from the author. The English version of the rPATD questionnaire was first translated into the Nepali language by two recognized translator in Nepal. The translation was then reviewed by the members of the research team (SS, RG, HPS) with Nepali as their first language, and a final draft was prepared. This was blindly back-translated to English by a third translator who was proficient in both English and Nepali. The third translator was not provided with the English version of the questionnaire. Both the translations were examined by the research team and a consensus was reached with some modifications. The translated version was pilot tested in 40 participants (not included in the final analysis) for general readability of the questions and wording was appropriately adjusted for the final survey. The 5-point Likert scale was used to obtain the response of the participants to each question as in the original tool. However, while interpreting the results of the survey, the responses ‘agree’ and ‘strongly agree’ were considered as ‘agree’ and ‘disagree’ and ‘strongly disagree’ were considered as ‘disagree’.
Statistical analysis
Descriptive statistics were used to characterize data on demography, medical conditions, polypharmacy and rPATD responses using IBM-SPSS version 25.0 for Windows (IBM Corporation, Armonk, NY, USA). The normality test of the numeric data was performed using the Kolmogorov–Smirnov test to express their central tendency and dispersion, while categorical data were expressed as frequency and percentage. Factor score was calculated according to the method followed by Reeve et al. 18 Bivariate analyses were performed to assess the association of study variables (demography, medical condition, polypharmacy, burden factor score, appropriateness factor score, concerns about stopping factor score, involvement factor score and satisfaction with current medicines score) with the willingness of patients to have one or more of their regular medicine(s) deprescribed. Variables that were statistically significant in the bivariate analysis were subjected to multivariate logistic regression analysis using the backward stepwise likelihood ratio method to predict the factors influencing the willingness to deprescribe. p ⩽ 0.05 was considered a statistically significant value. For analysis, willingness to deprescribe was converted into a binary variable by combining the response ‘agree’ and ‘strongly agree’ into ‘Yes’ and all other responses into ‘No’. A multicollinearity test for the regression model was also performed.
Ethics
Ethical approval was obtained from the Institutional Review Committee of Shree Medical and Technical College (SMTC-IRC-20190721), Chitwan, Nepal. Each participant provided verbal consent followed by a written consent before data collection.
Results
Characteristics of participants
A total of 385 older ambulatory patients were included in the study from three hospitals located in the Chitwan district of Nepal. Table 1 shows the characteristics of the participants. The study population comprised 53.5% males, most with no school background (70.9%), from within the district of the study site (90.4%) and with a median [interquartile range (IQR)] age of 72 (8) years. The common medical conditions among the older adults were hypertension (64.9%), followed by diabetes (30.4%), heart disease (12.2%) and renal disease (8.6%). Polypharmacy was observed in 11.2% of the total participants.
Characteristics of the study population (n = 385).
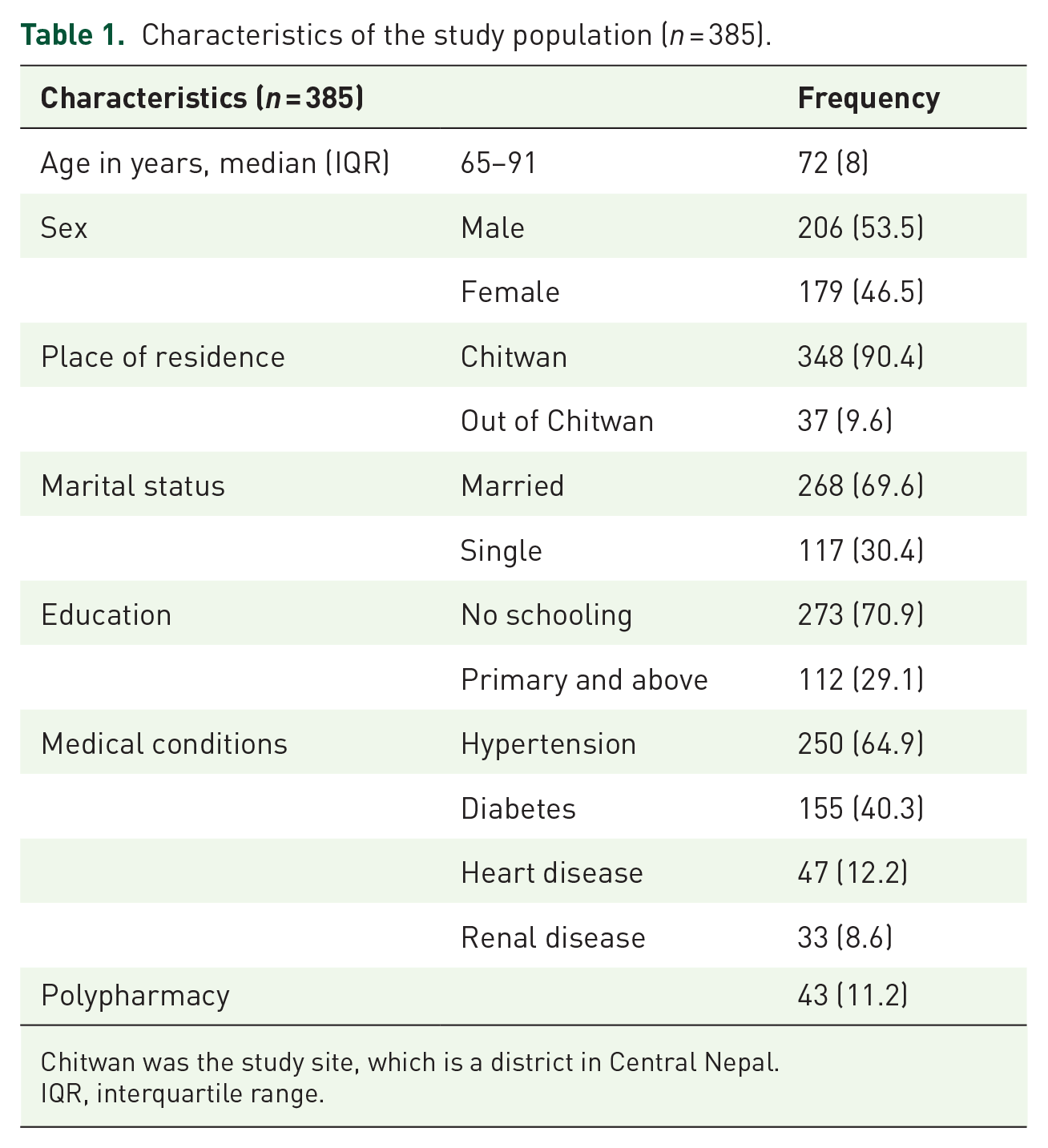
Chitwan was the study site, which is a district in Central Nepal.
IQR, interquartile range.
Attitudes towards deprescribing
The attitude of older patients towards deprescribing assessed using the rPATD tool is presented in Table 2. The items B1–B5, A1–A5, C1–C5, I1–I5 and G1–G2 represent questions of burden factor, appropriateness factor, concern about stopping factor, involvement factor and global questions, respectively. The responses to four factors and global questions are discussed below.
Attitudes of older patients towards deprescribing using revised Patient Attitude Towards Deprescribing (rPATD) questionnaire (n = 385).
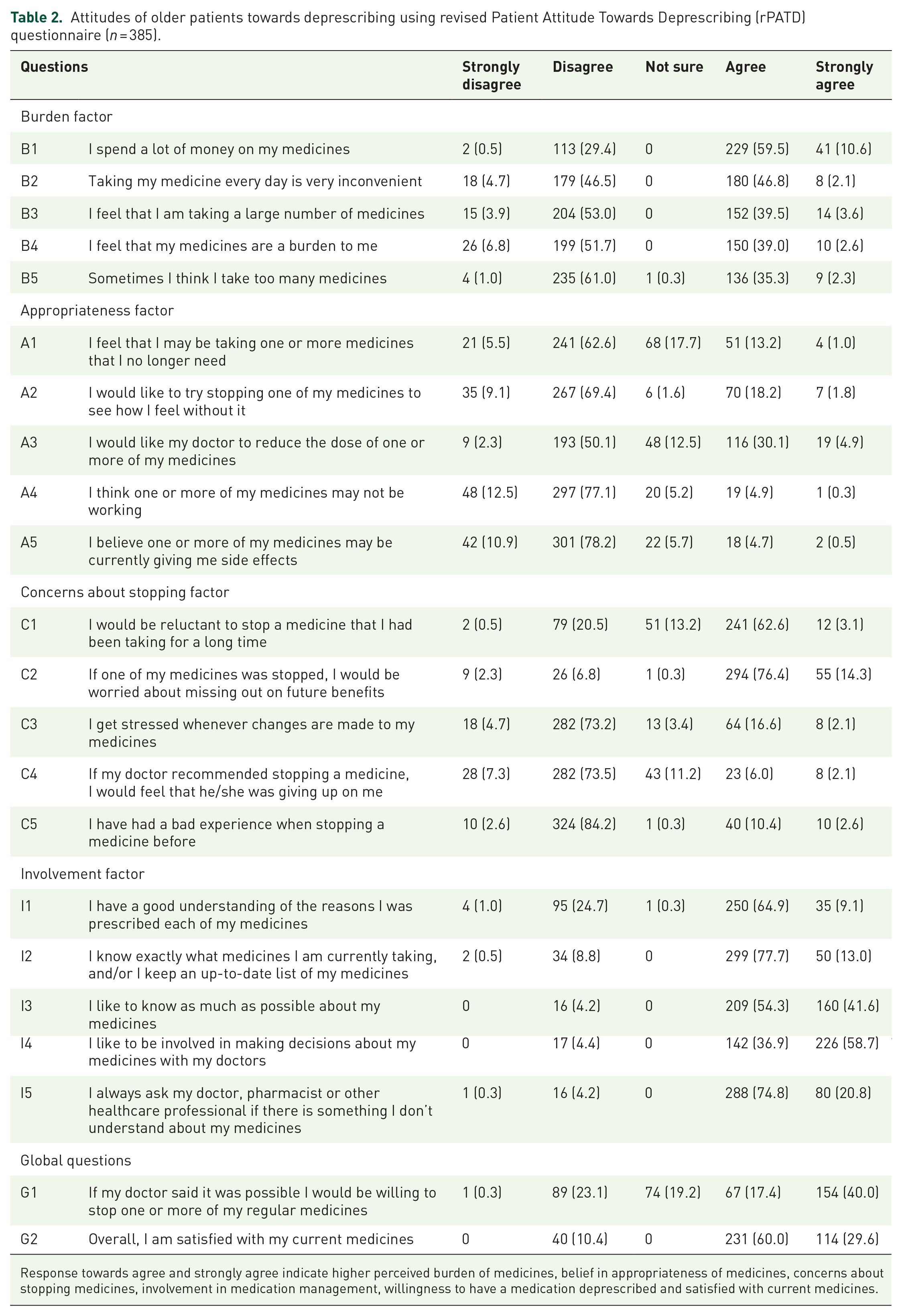
Response towards agree and strongly agree indicate higher perceived burden of medicines, belief in appropriateness of medicines, concerns about stopping medicines, involvement in medication management, willingness to have a medication deprescribed and satisfied with current medicines.
The response to burden factor showed that the majority of the participants (270, 70.1%) would agree that they spend a lot of money on their medicines (B1), though most of them (225, 56.9%) would disagree that their medicines were a burden to them (B4).
The appropriateness response indicated that the majority of participants would disagree that they might be taking one or more medicines that they no longer need (262, 68.1%) (A1) and would also disagree to try stopping one of their medicines to see how they feel without it (302, 78.5%) (A2). However, there was some agreement (135, 35.0%) that they would like their doctor to reduce the dose of one or more of their medicines even though most would disagree that one or more of their medicines might not be working (345, 89.6%) (A4) or currently giving them side effects (343, 89.1%) (A5).
The response to questions on concerns about stopping factor reflects that most of the participants agreed that they would be reluctant to stop a medicine that they had been taking for a long time (253, 65.7%) (C1) and that if one of their medicines was stopped they would be worried about missing them out on future benefits (349, 90.7%) (C2). However, a majority of them disagreed that they would be stressed whenever changes are made to their medicines (300, 77.9%) (C3) and if their doctor recommended stopping a medicine they would disagree that they would feel that s/he is giving up on them (311, 80.8%) (C4). Most of them (334, 86.8%) disagreed that they had a bad experience when stopping a medicine before (C5).
The responses to involvement factors showed that the majority of participants agreed that they had a good understanding of the reasons why they were prescribed each of their medicines (285, 74.0%) (I1) and that they knew exactly what medicines they were currently taking and/or they kept an up-to-date list of their medicines (349, 90.7%) (I2). Almost all of them agreed that they would like to know as much as possible about their medicines (369, 96.9%) (I3) and be involved in decision-making about their medicines with their doctors (368, 95.6%) (I4).
The response to global questions suggests that the majority of participants would agree that they would be willing to stop one or more of their regular medicines if their doctor said it was possible (221, 57.4%) (G1) even though most agreed that they were satisfied with their current medicines (345, 89.6%) (G2).
The factor scores (Table 3) shows that the median scores of perceived burden of medications, belief in the appropriateness of medications, concerns about stopping medications and involvement in medication management were 2.8, 2.6, 2.8 and 4.0, respectively.
Factor score (n = 385).

Score ranged between 1 and 5. Higher scores indicate the greater perceived burden of medications, belief inappropriateness of medications, concerns about stopping, and involvement in medication management. q1 and q3 represent the 25th and 75th percentile.
Table 4 shows the explorative analysis of potential factors influencing the willingness of older patients to have one or more of their regular medicine(s) deprescribed (now onwards used ‘willingness towards deprescribing’). The table also depicts the differences in the descriptive statistics between those who would have or would not have a willingness towards deprescribing. The bivariate analysis showed that age (p = 0.006), renal disease (p = 0.045), polypharmacy (p = 0.043) and concern about stopping medications (p < 0.020) were significantly and independently associated with the willingness to have one or more of their regular medicine(s) deprescribed among older patients. However, multivariate logistic regression analysis showed that age (p = 0.003) and concern about stopping the medications (p = 0.013) among older patients were statistically significant predictors of the willingness towards deprescribing. The regression model suggests that an increase in age by 1 year decreases the odds of willingness to deprescribe by 0.946 times (95% CI 0.913, 0.981). Also, those with high concerns about stopping medication scores (⩾2.8/5.0) have 0.541 times lesser odds (95% CI 0.334, 0.876) of willingness towards deprescribing than those with low concerns (score <2.8).
Factors influencing the willingness of older patients to have one or more of their regular medicine deprescribed (n = 385).

Statistically significant.
Median (IQR).
CI, confidence interval; IQR, interquartile range; OR, odds ratio; rPATD, revised Patients’ Attitudes Towards Deprescribing; SE, standard error.
Discussion
Our study on older patients who visited the selected hospitals of Chitwan district of Nepal for the outpatient services suggests that more than half of the older ambulatory patients would be willing to have one or more of their regular medication stopped if their doctor said it was possible. The predictors of potential factors influencing the willingness to deprescribe were age and score on concerns about stopping medications factor.
We found that, despite the willingness of more than half of Nepalese older patients to deprescribe their medications, this is comparatively lower than other countries including resource-limited settings such as Ethiopia (82%) 19 or higher income setting such as Australia (88%). 20 Studies show that 5–19% of older patients in Nepal receive PIMs.13–17 These include medications that should generally be avoided in older adults due to high risk to their health. PIMs are often associated with poor health outcomes such as hospitalization, falls and reduced quality of life.7–9,21 Older adults are prone to physiological changes due to ageing and this change could alter the pharmacology of medications.5,22 Deprescribing could be a good opportunity to reduce the risk associated with such medications. With reference to the finding from our study, the majority of older patients would agree to deprescribe on confirmation from doctors. This also reflects that older adults are open for discussion on deprescribing and that healthcare professionals, particularly doctors, could also consider this as a part of their discussion with patients or with their caregivers in routine care.
The findings of our study on rPATD factors suggest that the older adults had a moderate perceived burden of medications, moderate concerns about medications, higher belief in the appropriateness of medications and higher involvement in medication management. Also, the satisfaction with current medication was higher. This finding is similar to the findings in Australia. 20
With regards to the perceived burden of medicine, we found that nearly three-quarters of the older patients considered that they spent a lot of money on their medicines, though most of them would not consider medicines as a burden. This also suggests that the burden of medicine is more related to the financial aspect. A similar finding was reported in a resource-limited setting, 19 and this is of particular concern in countries with a similar economic status as Nepal where the healthcare system mainly depends on out-of-pocket payment (OPP) from patients. 23 Withdrawing medications that do not benefit the patients for an improved health outcome could also be beneficial for those who depend upon OPP for their medications and treatment.
We found that our study population had a high belief in the appropriateness of their medications. Few participants would try stopping one of their medicines to see how they feel without it, and that they would not believe that one or more of their medications might not be working or currently giving them side effects. Nevertheless, a comparatively higher number of participants would like the doctor to reduce the dose of one or more of their medicines. These findings reflect that older patients in Nepal might consider deprescribing but with a thorough consultation with their doctors.
The response on concerns of the older patients about stopping medications in our study depicts that most of them would be reluctant to stop medications that they have been taking for a while and would be worried about missing their medications on future benefits if stopped. There is no exact reason for this, but it could be possible that prescribers might be educating patients on these aspects for medication adherence. Patients should also be educated that some medications could be discontinued if they become harmful, non-beneficial or less relevant. Our study also found that majority of the patients would not consider that they would be stressed if changes are made to their medicines, and they would not consider that doctors are giving up on them if they were to recommend stopping their medications. These findings suggest that there exists some positive attitude towards deprescribing and that Nepalese older patients trust their doctors for deprescribing. Patients trust in doctors has been known to influence deprescribing24,25 and could act as both barrier and enabler.26,27 However, in the present study, we did not explore the influence of trust in physician on the willingness of older patients to have one or more of their medication deprescribed.
Our study shows that older patients were highly interested in medication management. Almost all of them would want to know as much as possible about their medications and be involved in decision-making on the medications with their doctors. Patients having a greater interest in shared decision-making could provide a greater opportunity for healthcare professionals to deprescribe PIMs. In a study conducted in 11 European countries, the desire of older people to be involved in medicine-related decisions was known to be highly heterogeneous and would require a tailored approach. 28 A study in Australia found three kinds of older patients when it comes to the preference to be involved in decision-making and openness to deprescribing: type 1 with a positive attitude towards medications with a preferred role for doctors to decide, type 2 with an ambivalent attitude towards medications with a preferred proactive role and open to deprescribing, and type 3 who tend to be frail with perceived lack of knowledge on medicines and deferring the most decision to their doctors or caregivers. 29 Our study participants seem to fall under type-1, that is, they tend to have a positive attitude towards medications and trust doctors to decide.
The regression analysis in our study suggested that with a year increase in age, patients aged 65 years and above tend to have a reduced willingness towards deprescribing. A better approach might be to discuss the possibility of deprescribing in the future with these patients at the commencement of the prescription and follow-up visits, particularly in medications that could have potential risk associated with them. A similar result was observed in a study conducted in Singapore, but this study included participants 45–84 years and only 37% were older adults. 30 Besides age, in the present study we also found concerns about stopping medication as one of the significant predictors of willingness to deprescribe. Those with greater concerns about stopping their medication (median score of ⩾2.8 out of 5.0) had lesser odds of willingness to deprescribe as compared with those with lower concerns (median score <2.8). This suggests that concerns about stopping the medication are a significant barrier for deprescribing in older Nepalese patients. Therefore, it is essential to understand the reason for the concerns of these patients before approaching to implement deprescribing in the Nepalese scenario. The overall concern scores were derived from the concerns about stopping their long-term medication, concerns about missing out on future benefits, concerns when changes are made to their medications, concerns about giving up on them when a doctor would recommend stopping their medication and prior bad experience when medication was stopped. Hence, these concerns might need to be appropriately addressed. A study in older Australian also found that those with higher concerns on stopping the medication (score ⩾2.4) had 0.12 times lesser odds for willingness to have a medication deprescribed. 20
In the context of Nepal, this study is probably the first attempt to assess the attitude of patients towards deprescribing. However, the results might need careful interpretation for generalizability as this study was conducted in a purposefully selected geographical location, via a convenient sampling procedure and did not represent a diversified population of Nepal. This study was conducted in an urban district of Nepal and the majority of participants were from within the district. Studies have found variation in the health-seeking behaviour of people living in urban and rural settings.31,32 So, further exploration might be needed to clarify whether the attitudes among those living in the rural areas or even other urban areas of Nepal remain the same. The majority of the participants involved in this study had either no formal schooling or lower education level; therefore, the findings might not well represent the perception of older adults with a higher level of education towards deprescribing. The other limitation of this study is that the statistical validity of the translated rPATD tool used in this study is yet to be determined.
Conclusion
A significant percentage of Nepalese older adults visiting the hospitals for ambulatory care services would be willing to stop one or more of their regular medications under the advice of their doctor. Age and concerns about stopping medications are predictors of willingness to deprescribe in this population. The concept of deprescribing is novel to Nepal and it might be worth exploring the understanding and preparedness of all stakeholders on deprescribing, that includes patients, caregivers, and healthcare providers.
Supplemental Material
sj-pdf-1-taw-10.1177_20420986211019309 – Supplemental material for Attitudes of ambulatory care older Nepalese patients towards deprescribing and predictors of their willingness to deprescribe
Supplemental material, sj-pdf-1-taw-10.1177_20420986211019309 for Attitudes of ambulatory care older Nepalese patients towards deprescribing and predictors of their willingness to deprescribe by Shakti Shrestha, Roshan Giri, Hari Prasad Sapkota, Siddhartha Sharma Danai, Ahsan Saleem, Shreeshab Devkota, Sagar Shrestha, Bhojraj Adhikari and Arjun Poudel in Therapeutic Advances in Drug Safety
Research Data
sj-sav-2-taw-10.1177_20420986211019309 – for Attitudes of ambulatory care older Nepalese patients towards deprescribing and predictors of their willingness to deprescribe
sj-sav-2-taw-10.1177_20420986211019309 for Attitudes of ambulatory care older Nepalese patients towards deprescribing and predictors of their willingness to deprescribe by Shakti Shrestha, Roshan Giri, Hari Prasad Sapkota, Siddhartha Sharma Danai, Ahsan Saleem, Shreeshab Devkota, Sagar Shrestha, Bhojraj Adhikari and Arjun Poudel in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
We would like to sincerely thank all the participants for their involvement in this study. We appreciate the support from Bharatpur District Hospital, Chitwan Medical College Teaching Hospital and College of Medical Sciences for assisting with recruitment and data collection.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.