
Abstract
Background:
Our aim in this research was to establish whether integrating an electronically generated calculation and report on the Drug Burden Index (DBI) in the Home Medicines Review (HMR) setting is an accurate, feasible and useful risk assessment tool to assess risk of anticholinergic and sedative medications; and to establish whether the intervention of DBI together with HMR is associated with a reduced use of anticholinergic and sedative medications in older community-dwelling adults in Australia.
Methods:
An interventional feasibility study was conducted. Accredited clinical pharmacists (APs) were recruited to participate. Each AP was educated on implementation of the DBI into HMR practice and given access to the DBI Calculator© web-based software to generate the DBI report for inclusion in HMR reports for general practitioners (GPs). APs recruited patients (⩾65 years) who were referred to them for HMRs. Patients were sent a letter about their DBI exposure, and a prompt to visit their GP to discuss their medication management options. GPs, APs and patients were asked to evaluate the feasibility and utility of the DBI report. A medication inventory was collected from patients at the time of the HMR and at 3 months to determine whether the intervention affected deprescribing of medications with anticholinergic and sedative effects.
Results:
Regarding the feasibility of the DBI report as a risk assessment tool within HMR, 89% of APs and 67% of GPs agreed that it would be feasible. The DBI Calculator© was potentially inaccurate, as 26% of DBI scores were underestimated and 7% were overestimated (at baseline). At 3 months, the median (interquartile range) DBI for patients (n = 100) significantly decreased from 0.82 (0–1.33) to 0.67 (0–1.29) (p = 0.014). Additionally, of patients with a DBI > 0 (n = 66), 36.4% had their DBI score decrease, and 6.1% had a score increase.
Conclusion:
This study demonstrated that integration of the DBI Calculator© into HMR is a feasible and useful method to prompt deprescribing of anticholinergic and sedative medications in older adults. There is potential for the accuracy of the web-based platform to be improved.
Registration of trial:
Name: Feasibility study of the Drug Burden Index with Home Medicines Review.
Website: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=368523
Trial ID: ACTRN 12615000539538.
Introduction
Among people aged over 65 years, multimorbidity (two or more chronic diseases)1,2 is present in 75–88% of people, and more than 40% in this age group have polypharmacy (use five or more medications).3,4 Polypharmacy is associated with poor clinical outcomes such as mortality, falls, disability and frailty. 5 Medications with anticholinergic and sedative properties are frequently used by older adults and are associated with adverse drug events (ADEs), including poor physical and cognitive function and neuropsychiatric ADEs, leading to increased hospitalization and nursing home admissions. In some cases, these medications may be inappropriately prescribed, contribute to polypharmacy and be targeted for deprescribing.6–9
The Drug Burden Index (DBI) is a pharmacological measure of the cumulative exposure to anticholinergic and sedative medications. The DBI was developed to estimate the risk of these medications to physical and cognitive functional impairment in older adults.10,11 Increasing DBI has been associated with poorer physical function, falls, frailty, hospitalization and mortality in older adults.12,13 To date, two interventional studies have been conducted in the primary care setting specifically aiming to reduce total anticholinergic and sedative medication use, measured by DBI.14,15 The study by Gnjidic and colleagues, which used a letter and phone-call intervention directed towards general practitioners (GPs), used DBI to prompt consideration of cessation or dose reduction of anticholinergic and sedative medications. This study observed a nonsignificant reduction of DBI in 32% of patients in the intervention group, and 19% of patients in the control group. 14 In 2018, Van der Meer and colleagues conducted a randomized controlled trial (single blind) where patients randomized into the intervention arm received a pharmacist-led medication review that focused on anticholinergic and sedative medications. This study found no difference in the proportion of patients with a ⩾0.5-point decrease in DBI scores between the intervention and control groups. 15
In Australia, the Home Medicines Review (HMR) service aims to aid in the reduction of preventable drug-related hospital admissions and improve the quality use of medicines in older adults. 16 The HMR service is a government-funded community-based collaborative service between patients, GPs and accredited clinical pharmacists (APs). An AP, a pharmacist that has undergone specialized training to undertake HMRs, receives a referral for a patient from the GP, conducts an interview with the patient in the home to gain a comprehensive medication profile, and documents medication review findings and recommendations in a report for the GP, which can then be used to formulate the patient’s medication management plan. 17 Observational studies have demonstrated the impact of medication review in reducing the number of prescribed medications and drug-related problems, including reducing DBI scores.18,19 However, there is limited evidence supporting the benefit of medication reviews on clinical outcomes. 20 Studies observing associations between pharmacist recommendations for medications with anticholinergic and sedative effects and important clinical outcomes in older adults are limited to pilot studies or studies of single drug classes.21–24
Calculation of the DBI requires knowledge of anticholinergic and sedative properties of medications, their minimum efficacious doses, and consideration of medications with the same ingredients taken in different formulations together. 11 In previous studies, we found that approximately 18% of pharmacists were unable to accurately calculate the DBI for a hypothetical patient and therefore the utility of the DBI as a clinical risk assessment tool may require software to facilitate the calculation and its interpretation.25,26 A recent Cochrane review suggested that it is unclear whether interventions using computerized clinical decision support systems (CCDSS) may improve appropriate polypharmacy, and further studies are required. 27 The HMR service model provides an ideal study setting to investigate the accuracy, feasibility and utility of an electronic intervention of implementing DBI as a risk assessment tool.
Therefore, in a population of older community-dwelling adults (⩾65 years) receiving the HMR service in Australia, the study objectives were to:
(1) establish whether addition of an electronically generated calculation and report on DBI in the HMR setting is an accurate, feasible and useful risk assessment tool to assess risk of anticholinergic and sedative medications; and
(2) establish whether the intervention of the DBI together with HMR is associated with a reduced use of anticholinergic and sedative medications.
Methodology
Study design
This interventional feasibility study using historical controls, investigated the accuracy, feasibility and usefulness of reporting the DBI in the HMR setting (Figure 1). The study was conducted between October 2014 and November 2015. The protocol for this study was retrospectively registered with the Australian New Zealand Clinical Trials Registry (ANZCTR): ACTRN12615000539538. All study participants gave written, informed consent. Ethical approval was obtained from the Executive of the Human Research Ethics Committee of the University of Sydney, Australia (2014/648).

Flow of accredited clinical pharmacists (APs), patients and general practitioners (GPs) through the feasibility study.
Stage 1: retrospective cohort (historical data collection)
APs were recruited by advertising in professional organization electronic newsletters and were screened according to eligibility criteria (Supplementary Table 1). Stage 1 required each AP participant enrolled in the study to provide anonymous data on their 10 most recent HMRs, by extracting data from their previous HMR referrals and reports, to complete a historical data collection sheet. These data were used as the historical control dataset for this study. The data provided by APs included sociodemographics and a medication inventory for their patients. The inclusion criteria for patients in the historical control dataset were: (a) that they received the HMR service; and (b) aged ⩾ 65 years.
Stage 2: education and training
Stage 2 of the study involved education and training of AP participants on the implementation of the DBI into the HMR service. Conducted by an accredited clinical pharmacist (LKO) via a webinar, the education and training supported the development of the pharmacists’ clinical skills and provided the training to partake in stage 3. This included instructions on how to determine patient eligibility and to obtain patient consent for participation in the study. Each AP received study materials such as data collection sheets, patient/carer participant consent forms, patient education materials, patient surveys, and pharmacist reading and education materials.
Stage 3: prospective cohort (intervention data collection)
Summary of calculating DBI
The DBI for every patient was calculated according to the formula:

where B indicates burden, AC indicates anticholinergic medications and S indicates sedative medications. With the assumption that anticholinergic and sedative effects of different medications are additive, similar to a linear model of pharmacological effect, the DBI was calculated using the following formula:

where D is the daily dose, and δ is the minimum recommended daily dose as listed by the medication product information approved by the Therapeutic Goods Administration of Australia.10, 12 The approved medication product information was also used to identify medications with anticholinergic or sedative pharmacological effects. Medications with both anticholinergic and sedative effects were classified as anticholinergic. Complementary medications and medications that were prescribed ‘when required’ (PRN) were excluded from DBI calculations. 11
The DBI Calculator© and report
The DBI Calculator© is a reliable CCDSS that has been developed to calculate and report on DBI of older patients taking multiple medications. 25 The DBI Calculator© report was redesigned after receiving feedback from focus groups and interviews consisting of GPs, APs and specialist physicians in a previous study. 25 The patient’s medication list with DBI score for each medication and the patient’s total DBI and risk level were retained. Alterations to the design included a detailed explanation of the DBI, an introduction of a scale, and columns to allow APs and GPs to comment on the use of the medications (Supplementary Figure 1).
Implementation of the DBI report into HMR
Each AP enrolled in the study was responsible for inviting their HMR patients to participate in the project (Figure 1). Patients were screened by the APs according to patient participant eligibility criteria (Supplementary Table 2) and all potential patient participants were provided with verbal and written information about the study. In cases where patients were unable to provide written informed consent but were still eligible and willing (assented) to participate in the study, consent was obtained from the patient’s carer. The HMR service continued independently of whether patients chose to participate in the study.
Upon completion of the patient interview and at the time of writing the HMR report for the referring GP, APs used the DBI Calculator© to generate a DBI report specific for the patient to attach to the HMR report. Within the HMR report to the referring GP, pharmacists also included a reference to the attached DBI report.
Intervention patient participants were provided questionnaires (at baseline, i.e. during HMR interview and 3 months after the HMR) to complete and return. The questionnaires included sociodemographic questions (collected at baseline), Beliefs about Medicines Questionnaire (BMQ)-specific questionnaire (collected at baseline), and questions about the feasibility and utility of the patient version of the DBI report (collected at 3 months; Table 1). 28 The BMQ specific was used to measure the perspectives of intervention patients on use of their multiple medications (polypharmacy). The BMQ specific comprises two scales: one assessing patients’ beliefs about the necessity of their medications for maintaining present and future health (necessity scale) and the other assessing their concerns about the potential adverse consequences of using their medications (concerns scale). All the questions are rated on a five-point Likert scale. The mean [standard deviation (SD)] of responses to the statements for each scale were calculated and reported. Higher means (midpoint of 3) indicate stronger beliefs in the concepts represented by the scale.
Summary of information gathered from patients in the prospective (intervention) arm of the study.
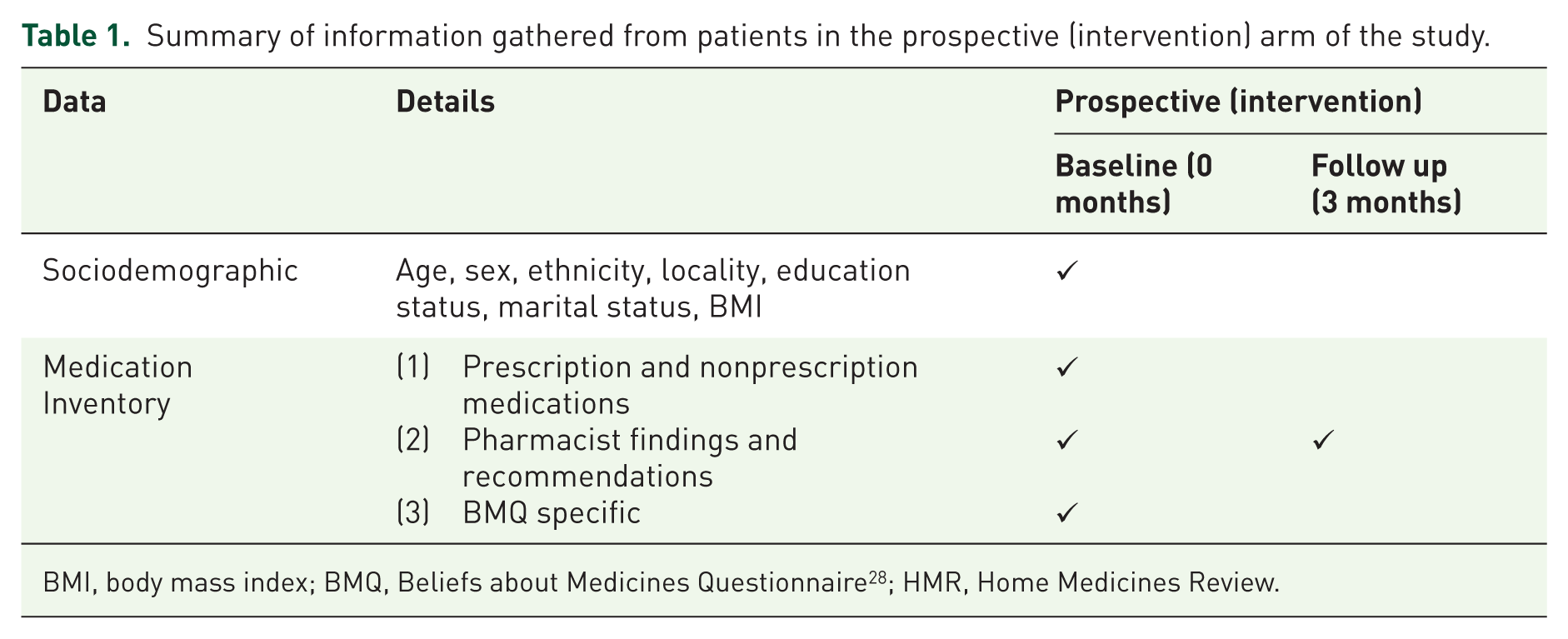
BMI, body mass index; BMQ, Beliefs about Medicines Questionnaire 28 ; HMR, Home Medicines Review.
For each intervention patient recruited into the study, a faxback feasibility survey was provided to the patient’s referring GP. At the end of patient recruitment, APs were also provided with a feasibility survey (Table 2).
Information collected about the feasibility of the DBI with Home Medicines Review (HMR) from patients, accredited clinical pharmacists and general practitioners.
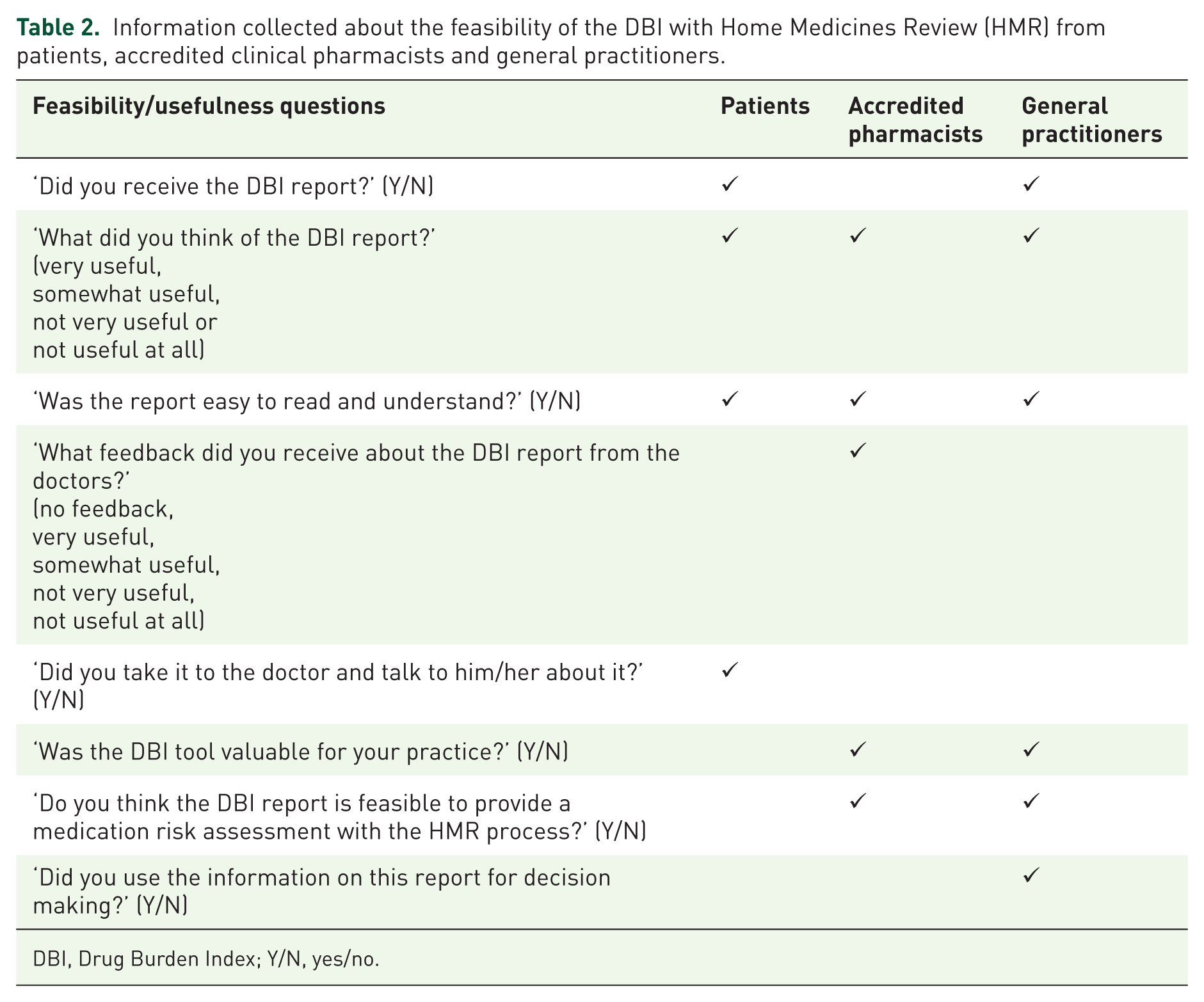
DBI, Drug Burden Index; Y/N, yes/no.
Pharmacist demographic data
APs provided data regarding their sociodemographics, including age, sex, pharmacy qualification, years of practice and locality of practice (measured by the Pharmacy Access/Remoteness Index of Australia which provides a standardized measure of the physical and professional remoteness of pharmacies throughout Australia 29 ).
Patient medication assessment
A medication inventory was provided by APs for all historical control (stage 1) and intervention (stage 3) patients. The name, dose and frequency of administration of all prescribed and over-the-counter medications at the time of the HMR were recorded on data collection sheets. The number of regular (prescribed or over the counter), PRN (as required) and complementary medications were recorded for each patient. Medications were coded according to the Anatomical Therapeutic Chemical (ATC) classification system. The DBI was measured using the previously published equation and methods.10,14 For historical control patients, the DBI was calculated manually and for intervention patients, DBI was measured manually and autogenerated using the DBI Calculator©.
Statistical analyses
All data were transferred from data collection sheets into computer databases. The collected data were analysed using IBM® Statistical Package for Social Sciences Statistics (SPSS® Version 21, Armonk, NY, USA).
To analyse the feasibility of implementing the DBI into HMR, descriptive statistics were used to report the patient, AP and GP responses to questions on feasibility and usefulness (Table 2). The written feedback provided by the APs about the implementation of the intervention was qualitatively analysed by content analysis. To analyse the accuracy of the DBI Calculator©, DBI scores calculated manually were compared with DBI scores autogenerated with the web-based platform for the intervention patient dataset. A Pearson’s correlation was used to determine the relationship between autogenerated and manually calculated DBI scores.
The Kolmogorov–Smirnov test and histogram were used to test the distribution of the DBI in the historical and intervention patient populations. As DBI was not normally distributed, the Mann–Whitney nonparametric test for continuous variables and χ2 test for categorical variables were used to compare characteristics between groups.
To analyse the effect of the DBI and HMR intervention on deprescribing anticholinergic and sedative medications in older adults, cross-sectional analyses were conducted to compare proportions of patients whose DBI increased, decreased or remained unchanged in the intervention group at baseline and 3 months.
Descriptive characteristics were summarized using means, SD [or median and interquartile ranges (IQR) for data not normally distributed] and proportions. The p value of less than 0.05 was set as statistically significant. Any missing data (not affecting the primary or secondary outcomes) were excluded from analyses.
Results
Study participation rates
As of June 2015, there were 26,179 general registered pharmacists in Australia, of whom 2396 were trained and practising APs. There were two rounds of advertising for APs to participate in this study (October 2014 and May 2015). Advertising for participation in this study reached an estimated 3196 pharmacists; 81 pharmacists enquired about the study (willingness to participate 2.5%) and were assessed for eligibility. Of these, 22 pharmacists were eligible and consented to participate in the study. Following stage 3 of the study, four pharmacists withdrew for various reasons (Figure 1). Of the 22 APs originally recruited, 21 provided data on their 10 most recent eligible HMR patients, resulting in a total of 210 historical controls. During the intervention stage, 18 APs screened a total of 354 HMR patients for eligibility and recruited 113 patients (recruitment rate 31.9%) into the study. Upon follow up, 13 patients withdrew (11.5% lost to follow up) resulting in a total of 100 patients in the intervention stage (Figure 1).
Characteristics of the accredited pharmacists
All APs had a Bachelor of Pharmacy qualification. The majority (70%) of APs had more than 15 years of experience working as a pharmacist, with 75% conducting >100 HMRs per year. APs were mainly practising in community pharmacy practice (55%) and practised in highly accessible areas in Australia (85%; Supplementary Table 3).
Characteristics of the patients
Across the historical control and intervention groups, the mean age (SD), proportion of male and female participants, marital status and body mass index were comparable. There was a significantly higher proportion of patients in the intervention patients group who lived in accessible areas compared with the historical patients (p = 0.037) (Supplementary Table 4). The mean (SD) of the BMQ-specific necessity and concerns questions were 3.4 (0.5) and 3.1 (0.6), respectively, indicating patients believed that their multiple medications were necessary and were slightly concerned about the adverse consequences about their medications.
Feasibility and utility of the DBI in Home Medicines Review
During stage 3, all pharmacists were able to produce a DBI report for their patients at baseline (n = 113). Twenty-seven patients and one GP reported not receiving the patient version of the DBI letter and DBI report, respectively. Within the HMR reports written by APs and sent to GPs (at 3 months, n = 100), 92 (92%) of reports contained a reference to the attached DBI report. When comparing the accuracy of the manual (considered gold standard, n = 100) and autogenerated DBI calculations (n = 97) for the intervention patients at baseline, the autogenerated DBI calculations did not match the manual calculations for 33 (33%) of the patients. Of the 33%, 26% of the autogenerated DBI calculations were underestimated and 7% were overestimated. At baseline, the mean (SD) autogenerated DBI was 0.81 (0.9), compared with manual DBI calculations 0.92 (1.0; r = 0.95, p < 0.01). At 3 months, the mean (SD) automated DBI was 0.71 (0.9), compared with manual DBI calculations 0.83 (0.9; r = 0.96, p < 0.01).
The feasibility and utility of the DBI report or letter are presented in Table 3. Most patients (81%), APs (89%) and GPs (83%) found the DBI report very or somewhat useful. Across all three groups, most participants found the DBI report easy to read and understand. Regarding assessing the DBI report as a risk assessment tool within the HMR service as part of usual care, 89% of APs and 67% of GPs agreed that it would be feasible. Furthermore, 57% of GPs used the information in the DBI report for their decision making. GPs found the DBI report more useful and feasible, and used the information for decision making when patients’ baseline DBI > 0 compared with patients with DBI = 0 (Table 4). Overall, although APs found that the DBI report was useful and complemented the HMR report, APs reported some issues with the website and report in practice (Table 5).
Responses to feasibility and utility questions from patients, APs and GPs who received/accessed the DBI report or letter.

AP, accredited clinical pharmacist; DBI, Drug Burden Index; GP, general practitioner.
Feasibility and utility of the DBI report among patients and GPs according to baseline DBI score.

DBI, Drug Burden Index; GP, general practitioner.
Written feedback from accredited pharmacists regarding the implementation of DBI into the Home Medicines Review (HMR) service.

AP, accredited clinical pharmacist; DBI, Drug Burden Index; GP, general practitioner.
Impact of DBI report intervention on prescribing and deprescribing
The median (IQR) DBI for the historical control patients was 0.50 (0–1.00). The intervention patients had a statistically significant higher median DBI of 0.82 (0–1.33) at baseline compared with the historical control (Mann–Whitney U test, z = −2.27, p = 0.023). At 3 months, the median (IQR) DBI for intervention patients significantly decreased to 0.67 (0.00–1.29; Wilcoxon signed-rank test, z = −2.45, p = 0.014). There was an equal distribution of patients with DBI = 0 and DBI > 0 across the historical and intervention datasets. The mean number of PRN and complementary medications were significantly higher for the intervention group (Table 6).
Medication characteristics of historical control and intervention patient study populations.

Only statistically significant values are shown.
Statistically significant p = 0.023; Mann–Whitney U test compared with historical control. **Statistically significant p = 0.014; Wilcoxon’s signed rank test compared with baseline intervention patients.
Statistically significant p = 0.031 compared with historical control.
Statistically significant p = 0.022 compared with historical control.
DBI, Drug Burden Index; IQR, interquartile range; SD, standard deviation.
Although the proportion of intervention patients at 3 months with DBI = 0 (n = 34) and DBI > 0 (n = 66) did not change, 36.4% of intervention patients with a baseline DBI > 0 had their DBI score decrease, whilst 6.1% had a score increase. For patients with a DBI = 0 at baseline, 8.8% of patients had their DBI increase at 3 months.
The medications prescribed (prescription and over the counter) for each patient participant in the historical and intervention datasets was analysed by ATC therapeutic class (Supplementary Table 5). The most common medications prescribed contributing to the DBI included oxycodone, pregabalin and amitriptyline. In the intervention group, there was a nonsignificant reduction in the number of patients using oxycodone, amitriptyline and pregabalin.
Discussion
This is the first study exploring the feasibility of implementing the DBI report, generated by the DBI Calculator©, into the HMR service as a risk assessment tool to guide medication review. Most patient participants, APs and GPs considered the DBI report very useful or somewhat useful. Regarding the feasibility of the DBI report as a risk assessment tool as part of usual care within the HMR service, 89% of APs and 67% of GPs agreed that it would be feasible (Tables 3 and 4). Further analysis demonstrated that the utility of the DBI report in practice was based on the patient’s DBI score: GPs considered the DBI report more useful for patients with DBI score > 0 compared with DBI score = 0 (Table 4). This may be due to the accustomed behaviour of GPs to recognize and act on a patient’s results when the score is above or below target ranges. The APs also provided written feedback relating to the implementation of the DBI report into HMR practice (Table 5). Barriers to implementation were identified mainly relating to the practicalities and content of the report. This feedback is different from the pilot study, where 80% of AP participants agreed or strongly agreed that the generation of the DBI report was feasible and may be implemented into routine practice as part of the usual HMR service with ease. 25 This feedback will be considered for future studies and demonstrates the importance of conducting feasibility studies in practice settings. 30
Feasibility studies are used to determine whether an intervention is appropriate for further testing and to estimate important parameters that are required to design larger randomized control studies. 31 These parameters include willingness of clinicians to recruit participants, number of eligible patients, follow-up rates, and characteristics of the proposed outcome measure. 32 Feasibility studies also include testing procedures for their acceptability and are an essential step in the development and testing of an intervention, prior to a largescale evaluation. 33 Regarding the feasibility of conducting this study, 2.5% of accredited pharmacists expressed interest in participating in the study, whilst only 18 pharmacists completed the study. Factors limiting the participation of APs in the research project may have included finding it difficult to recruit patients in research, and research protocols that were time consuming and not straightforward. 34 For patients screened for participation in the intervention arm, there was a recruitment rate of 31.9%, and 11.5% of those recruited were lost to follow up. Key factors likely to influence patient participation were the time taken for collection of additional data in person and by phone at baseline and follow up. A systematic review investigating the factors affecting the recruitment of patients to randomized controlled trials found that poor recruitment is common, many studies fail to meet recruitment targets, and factors such as educating clinicians, and incentives to participants, may help recruitment rates. 35 As patients and GPs involved in this study were not provided with incentives, this may have contributed to the low recruitment rates. Future studies should consider these factors.
Regarding the potential inaccuracy of the web-based DBI Calculator©, differences between manual and autogenerated DBI calculations (at baseline and 3 months) may have been due to data entry errors by the APs or to errors within the web-based calculator, such as discrepancies due to combination formulations or multiple drugs with the same ingredient.
At 3 months, the median (IQR) DBI for patients in the intervention arm of the study significantly decreased from 0.82 (0.00–1.33) to 0.67 (0.00–1.29) (p = 0.014; Table 6). In this study, the baseline median DBI for intervention patients was higher than previous studies, which may reflect patient selection bias by the study pharmacists.14,18,19 However, the median DBI score for patients in the historical control was 0.50, which is similar to two previous retrospective studies conducted in similar settings.18,19
Although the proportion of patients at 3 months with DBI = 0 and DBI > 0 did not change from baseline, 36.4% of patients with a DBI > 0 at baseline had their DBI score decrease, whilst 6.1% had a score increase at 3 months. This reduction in DBI score is higher than the proportion of patients who were exposed to DBI medications and received an HMR only 18 and slightly higher than the proportion of patients who had a decrease in their DBI scores in the pilot randomized controlled trial. 14 For the intervention patients in this study, there were more sedative than anticholinergic medications prescribed where doses were ceased or reduced that resulted in a reduction in DBI scores. A trial involving deprescribing of anticholinergic and sedative medications (using DBI) in residential aged care facilities is currently in progress in New Zealand, and the results of this study will provide the opportunity to compare and determine rates of deprescribing these medications in older adults. 36
This study has determined the recruitment rate of pharmacists and patients, follow-up rates of patients, pharmacists and GPs, the feasibility of implementing the DBI report as an intervention into the HMR setting, and the characteristics of measured outcomes: for example, proportion of patients referred for an HMR with a DBI > 0, and the proportion of patients who had their DBI changed as a result of the intervention. As this study was a feasibility study, the sample size was based on numbers required to test feasibility of conducting the intervention, and to estimate the sample size for a future randomized controlled trial. This was comparable with guidance on feasibility studies and published feasibility studies. 37
There were several strengths in this study. Recent evidence, based on comprehensive systematic reviews of reducing polypharmacy in older adults to improve clinical outcomes, conclude that successful studies incorporate multidisciplinary and multifactorial interventions, including patient education and clinician reminders.38,39 This study involved: (a) patients, GPs and APs receiving or generating information about patients’ DBIs; (b) patients receiving information about the benefits and harms of using anticholinergic and sedative medications; (c) the education of APs on deprescribing anticholinergic and sedative medications in practice by implementation of the DBI report into practice; and (d) GPs receiving the patient’s DBI report (acting as an educational tool and reminder). The multidisciplinary and multifactorial aspects of this study are likely to have contributed to the observed significant decrease in median DBI scores at 3 months. Previous studies using the pharmacist-led medication review model have demonstrated that recommendations provided by pharmacists in this setting are evidence based and are accepted as appropriate by GPs.40,41 Therefore, in our study, GPs would have been accepting of AP recommendations to change anticholinergic and sedative medications dependent on information provided in the HMR and DBI reports. Additionally, use of a CCDSS platform to administer the intervention is an innovative approach in research conducted involving HMRs.
There were several potential limitations in this study. Due to the study design, not all GPs responded to the feasibility questions, resulting in a very poor response rate. Therefore, we were unable to obtain representative usability or feasibility data from the end users of the DBI Report. Additionally, pharmacists volunteered to be in this study by responding to advertising and were not specifically recruited. This may have attracted pharmacists who were knowledgeable and keen to be involved in medication management of older adults resulting in selection bias in the study. A high proportion of pharmacists recruited in this study (85%) practised in highly accessible (urban) areas in Australia. In 2012, 92% of employed pharmacists worked in major cities or inner regional centres, therefore the high feasibility as demonstrated by the opinions of healthcare practitioners may not be generalizable to other settings. 42 There was also no consistency in the content or style of HMR reports written by pharmacists, with highly variable levels of detail in HMR reports sent to GPs. This may have contributed to the variability in GP uptake of recommendations relating to anticholinergic and sedative medications, and performance bias to the study. Future studies should analyse recommendation acceptance rates to assess the effectiveness of the intervention. Due to the retrospective nature of the historical control dataset and the difficulty of obtaining patient medication plans, direct comparisons could not be made on the effect of implementing the DBI report in the HMR service. Technical improvements to the DBI Calculator© may also improve the accuracy of reporting the DBI to GPs, such as upgrading the website and accuracy of the medications used to calculate DBI scores, especially with combination formulations.
Conclusion
Overall, implementation of the DBI report generated by the DBI Calculator© into the HMR service was feasible and useful, as reported by older adults, APs and GPs. The median (IQR) DBI of intervention patients was reduced from 0.82 (0.00–1.33) to 0.67 (0.00–1.29) (p = 0.014), demonstrating the deprescribing of anticholinergic and sedative medications in this patient cohort. Of those patients with a DBI > 0 at baseline (n = 66), the DBI score was reduced in 36.4% of patients at 3 months.
The role of the DBI Calculator© in practice would be to raise awareness and understanding of the cumulative risk of an older patient’s anticholinergic and sedative medications to their physical function, minimizing but not necessarily eliminating their exposure. Future studies to evaluate the recommendations of pharmacists, opinions of treating clinicians, and clinical outcomes of patients would help elucidate the clinical appropriateness of these medications for each patient.
Supplemental Material
Supplementary_131218 – Supplemental material for Integration of an electronic Drug Burden Index risk assessment tool into Home Medicines Reviews: deprescribing anticholinergic and sedative medications
Supplemental material, Supplementary_131218 for Integration of an electronic Drug Burden Index risk assessment tool into Home Medicines Reviews: deprescribing anticholinergic and sedative medications by Lisa Kouladjian O’Donnell, Danijela Gnjidic, Timothy F. Chen and Sarah N. Hilmer in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
This work was conducted during LKO’s PhD candidature with the support of an Australian National Health Medical Research Council (NHMRC) Primary Healthcare Scholarship. DG is supported by the Australian NHMRC Dementia Leadership Fellowship. The Drug Burden Index Calculator ©. All rights reserved 2019.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.